

🌟 HYPOMAGNESEMIA
A🧵
Hypomagnesemia has been described as the most underdiagnosed electrolyte abnormality in current medical practice.
A must know topic. Read on..👇
A🧵
Hypomagnesemia has been described as the most underdiagnosed electrolyte abnormality in current medical practice.
A must know topic. Read on..👇
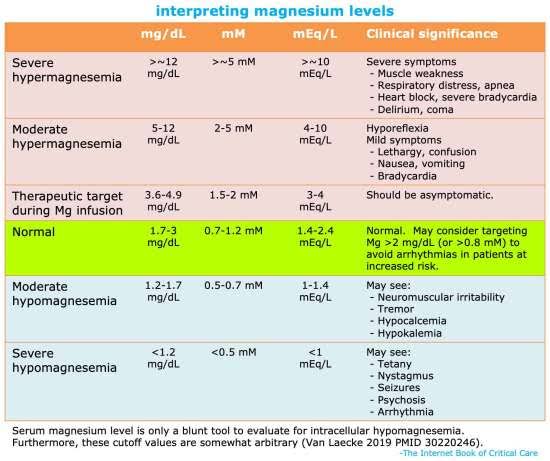
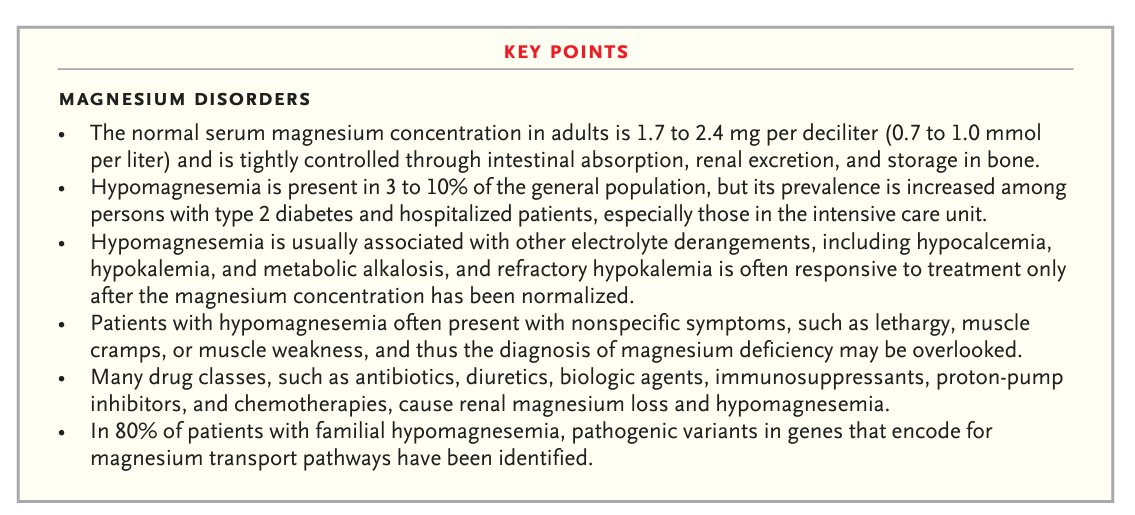
Normal range of Mg is 1.7 to 2.4mg/dL.
But serum levels doesn't reflect the actual body stores as majority of magnesium is in the extravascular space.
So a person can have magnesium deficiency even with normal serum levels.
But serum levels doesn't reflect the actual body stores as majority of magnesium is in the extravascular space.
So a person can have magnesium deficiency even with normal serum levels.
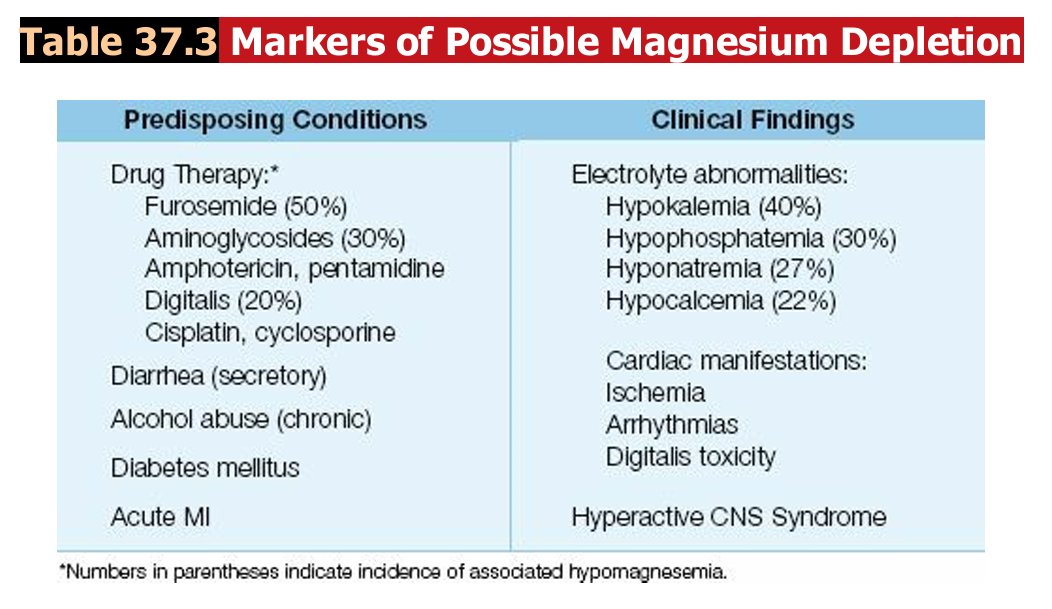
Hypomagnesemia is reported in as many as 80% of patients with acute myocardial infarction.
The mechanism is unclear, but may be due to an intracellular shift of Mg from excess catecholamines.
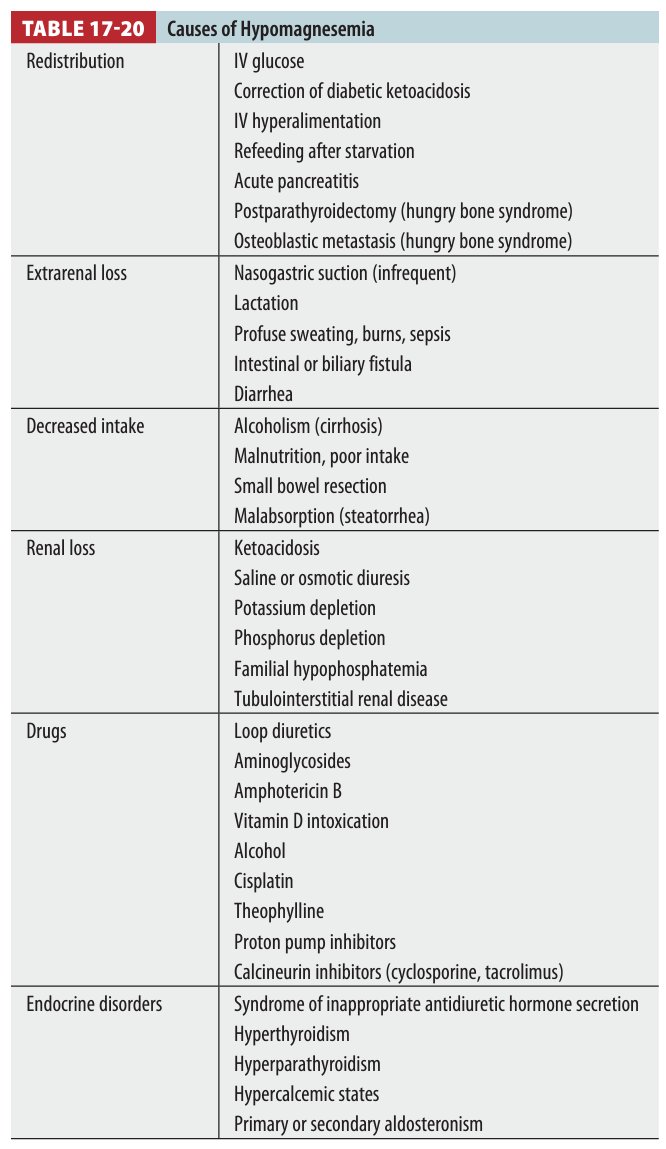
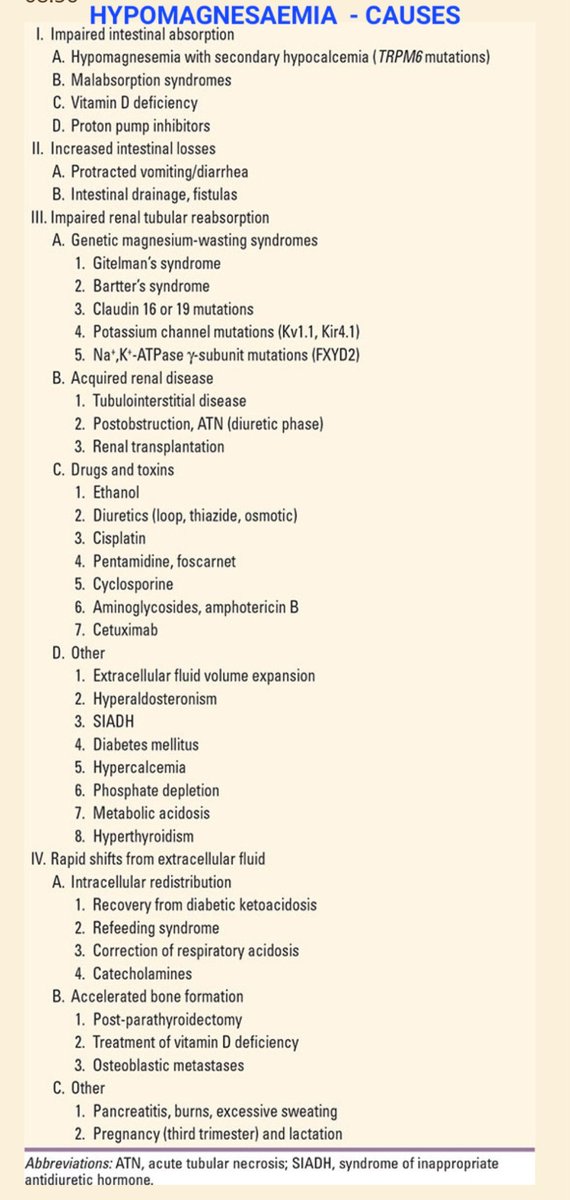
Causes of magnesium deficiency👇
The mechanism is unclear, but may be due to an intracellular shift of Mg from excess catecholamines.
Causes of magnesium deficiency👇
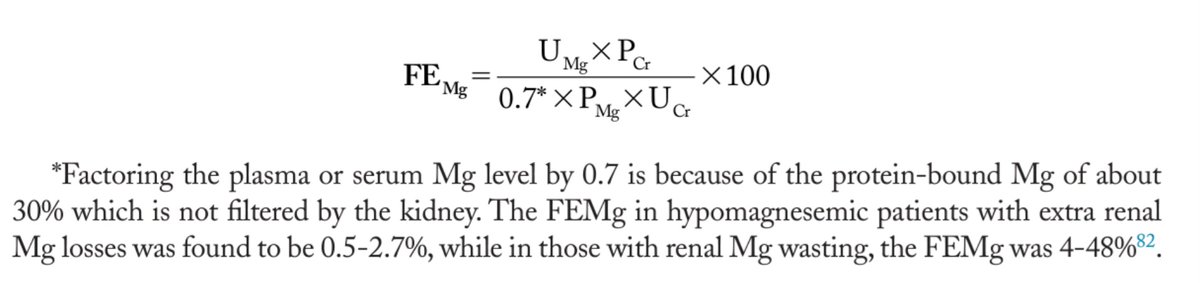
The diagnosis of GI versus renal losses of Mg in hypomagnesemic patients can be made by calculating the fractional excretion of magnesium (FEMg) as follows from a spot urine sample
( Not a mandatory test for evaluation but nevertheless helpful)
( Not a mandatory test for evaluation but nevertheless helpful)
Moderate Mg deficiency can be asymptomatic.
Severe Mg deficiency is marked by various clinical manifestations.
Hypomagnesemia can be accompanied by
-hypokalemia( as Mg is essential for renal reabsorption of K)
-hypocalcemia( Mg is required for PTH secretion)
-hypophosphatemia
Severe Mg deficiency is marked by various clinical manifestations.
Hypomagnesemia can be accompanied by
-hypokalemia( as Mg is essential for renal reabsorption of K)
-hypocalcemia( Mg is required for PTH secretion)
-hypophosphatemia
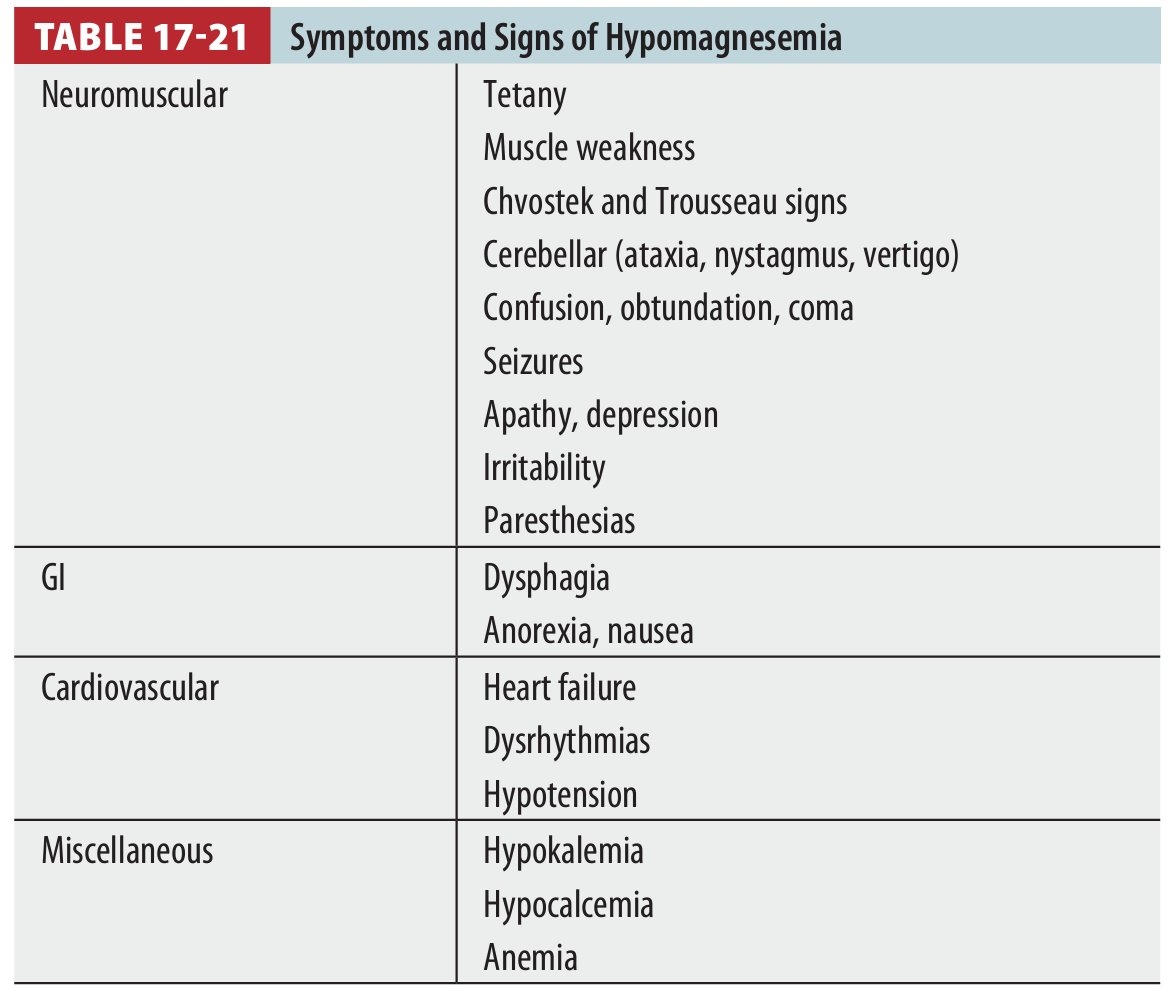
Chvostek sign and Trousseau sign, findings traditionally associated with hypocalcemia, may be elicited in hypomagnesemic patients.
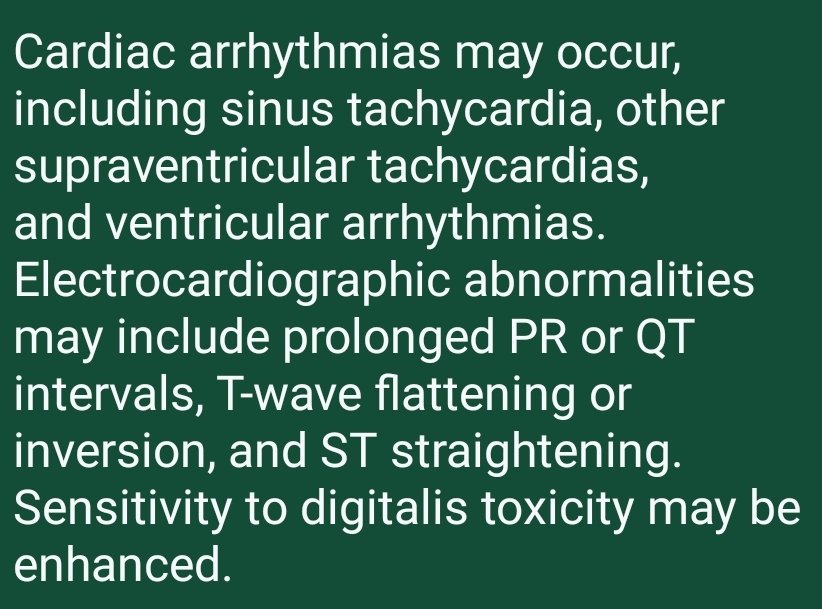
ECG manifestations can also due to concurrent hypokalemia and hypocalcemia.
ECG manifestations can also due to concurrent hypokalemia and hypocalcemia.
Mild, asymptomatic hypomagnesemia may be treated with oral magnesium salts in divided doses totaling 20–30 mmol/d (40–60 meq/d).
Diarrhea may occur with larger doses.
Diarrhea may occur with larger doses.

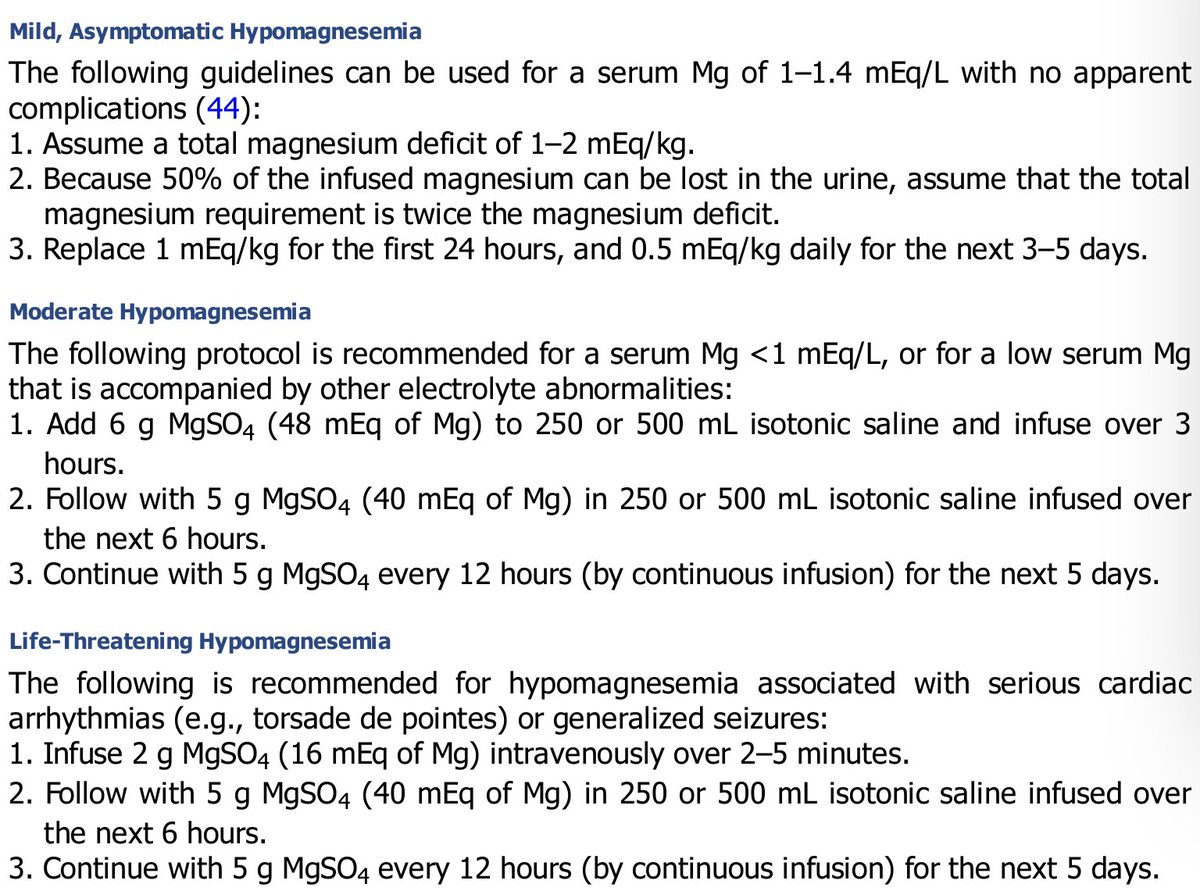
Management of severe hypomagnesemia ( serum levels <1.2mg/dL)
Conversion⤵️
1mmol Mg = 2mEq Mg= 24mg Mg
2ml of 50% MgSO4 ( one ampoule) contains 1gm MgSO4 which has 4mmol Mg = 8mEq Mg= 96mg Mg
Monitor Mg/Ca/K/PO4 levels atleast 12hrly
Conversion⤵️
1mmol Mg = 2mEq Mg= 24mg Mg
2ml of 50% MgSO4 ( one ampoule) contains 1gm MgSO4 which has 4mmol Mg = 8mEq Mg= 96mg Mg
Monitor Mg/Ca/K/PO4 levels atleast 12hrly
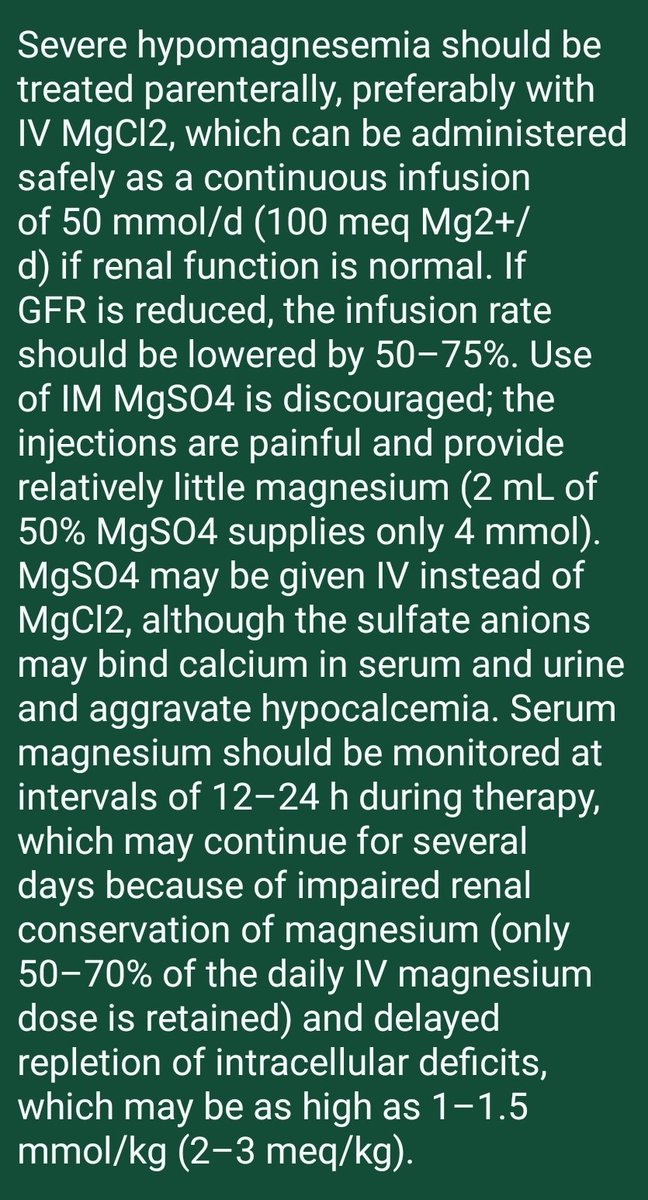
A 50% magnesium sulfate solution (500 mg/mL) has an osmolarity of 4,000 mosm/L, so it must be diluted to a 10% (100 mg/mL) or 20% (200 mg/mL) solution for intravenous use.
MgCl2 if available is better.
MgCl2 if available is better.
A common assumption is that 1 g of IV MgSO4 should raise the serum Mg by ∼0.15 mEq/L.
Serum Mg levels will rise after the initial MgSO4 bolus, but will begin to fall after 15 minutes.
Therefore, it is important to follow the bolus dose with a continuous magnesium infusion.
Serum Mg levels will rise after the initial MgSO4 bolus, but will begin to fall after 15 minutes.
Therefore, it is important to follow the bolus dose with a continuous magnesium infusion.
S. Mg levels may normalize after 1 to 2 days, but it will take several days to replenish the total body Mg stores
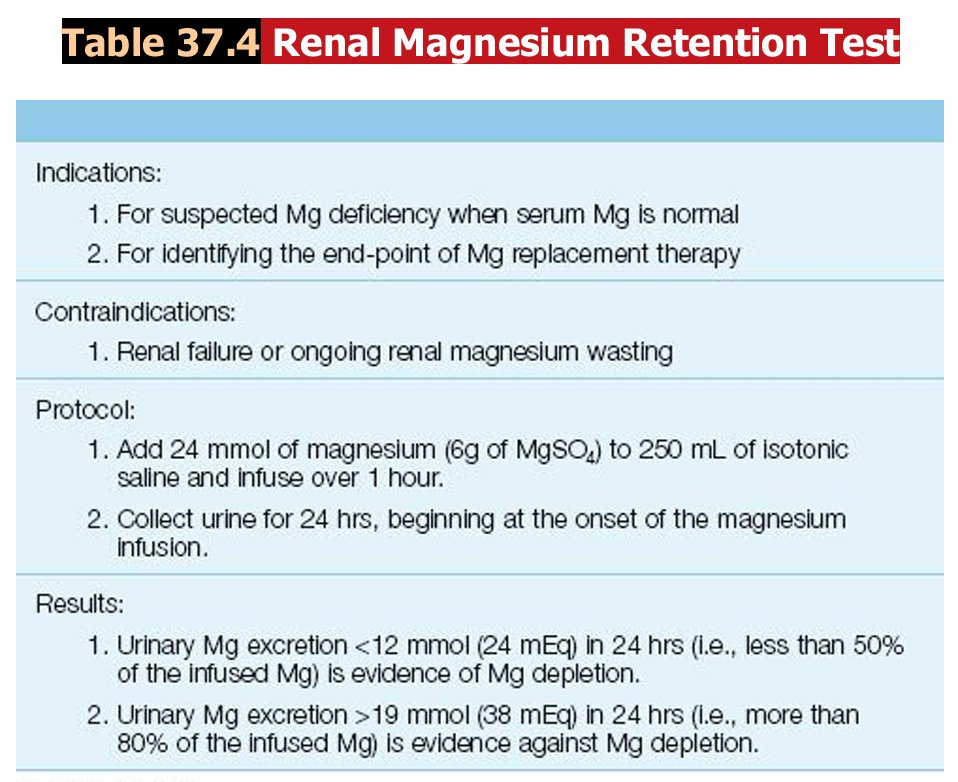
The magnesium retention test can be used for end-point of replacement therapy; Mg replacement is continued until urinary Mg excretion is ≥80% of the infused Mg load
The magnesium retention test can be used for end-point of replacement therapy; Mg replacement is continued until urinary Mg excretion is ≥80% of the infused Mg load
When magnesium is replaced in the setting of renal insufficiency, no more than 50% of the magnesium in the standard replacement protocols should be administered and the serum Mg should be monitored carefully.
Consider the need for calcium, potassium, and phosphate supplementation in
patients with hypomagnesemia.
Vitamin D deficiency frequently
coexists and should be treated
with oral or parenteral vitamin
D( cholecalciferol/ergocalciferol)
Calcitriol should not be used
patients with hypomagnesemia.
Vitamin D deficiency frequently
coexists and should be treated
with oral or parenteral vitamin
D( cholecalciferol/ergocalciferol)
Calcitriol should not be used
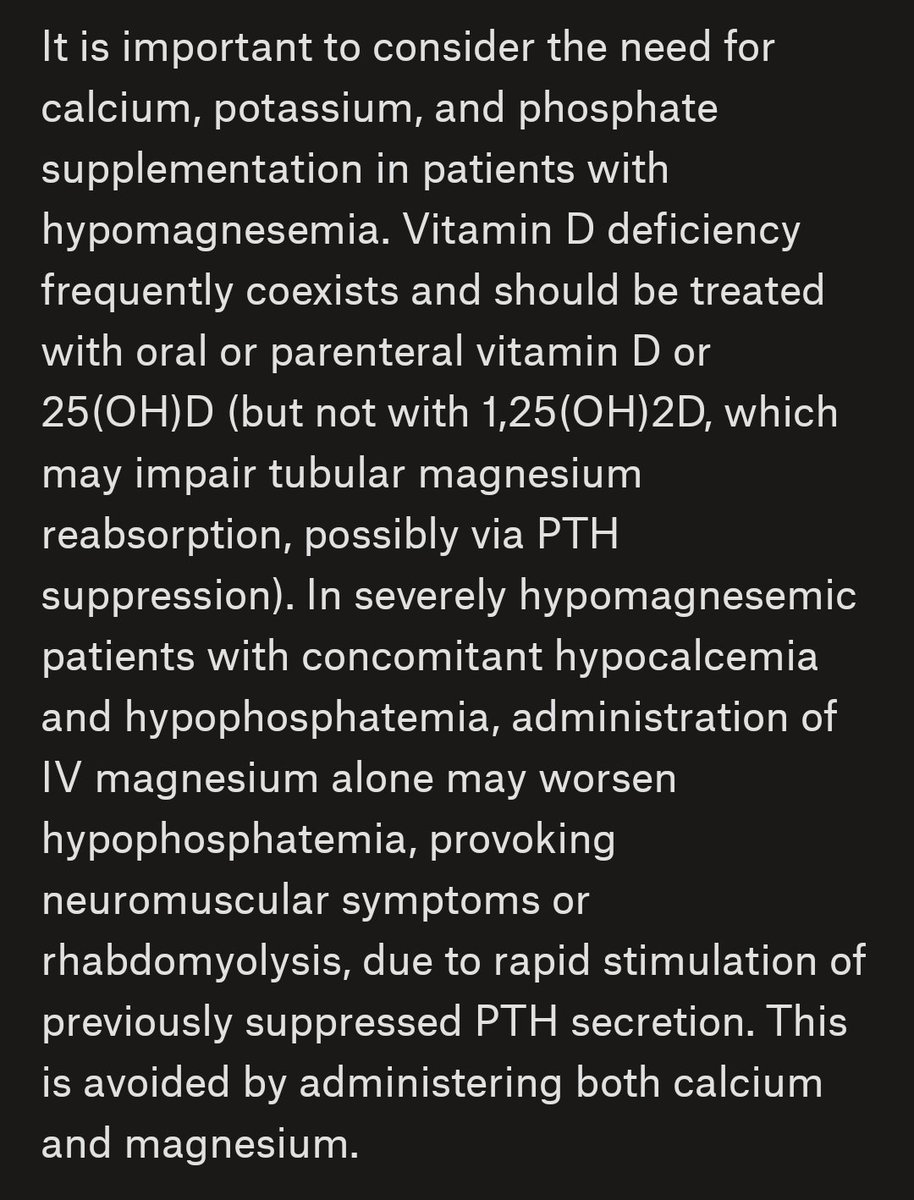
Hypocalcemia and hypokalemia secondary to hypomagnesemia will not correct unless magnesium is repleted.
Thank you for reading till the end🙏
Do post your appreciation and criticism in the comments below
Thank you for reading till the end🙏
Do post your appreciation and criticism in the comments below
Loading suggestions...