

🧵A thread on HHT therapies 🩸
With the publication of the largest powered RCT of a systemic therapy for the 2nd most prevalent inherited bleeding disorder, let’s discuss our systemic therapies for bleeding in hereditary hemorrhagic telangiectasia (#HHT)⤵️
#hemetwitter
1/21
With the publication of the largest powered RCT of a systemic therapy for the 2nd most prevalent inherited bleeding disorder, let’s discuss our systemic therapies for bleeding in hereditary hemorrhagic telangiectasia (#HHT)⤵️
#hemetwitter
1/21
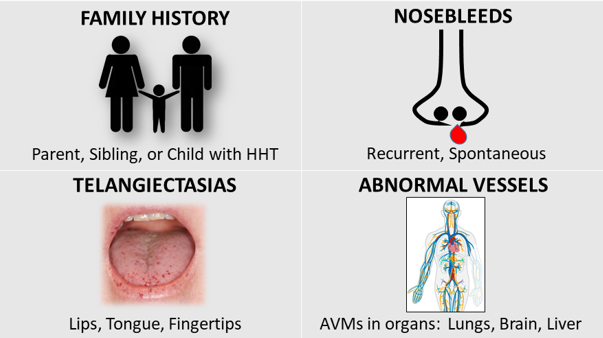
Briefly, HHT
➡️affects 1/3800 ppl
➡️causes extensive mucocutaneous telangiectasias and visceral arteriovenous malformations (AVM)
➡️has pathogenic variants affecting TGFβ–BMP signaling
➡️leads to epistaxis, the primary sx affecting QoL
2/
➡️affects 1/3800 ppl
➡️causes extensive mucocutaneous telangiectasias and visceral arteriovenous malformations (AVM)
➡️has pathogenic variants affecting TGFβ–BMP signaling
➡️leads to epistaxis, the primary sx affecting QoL
2/
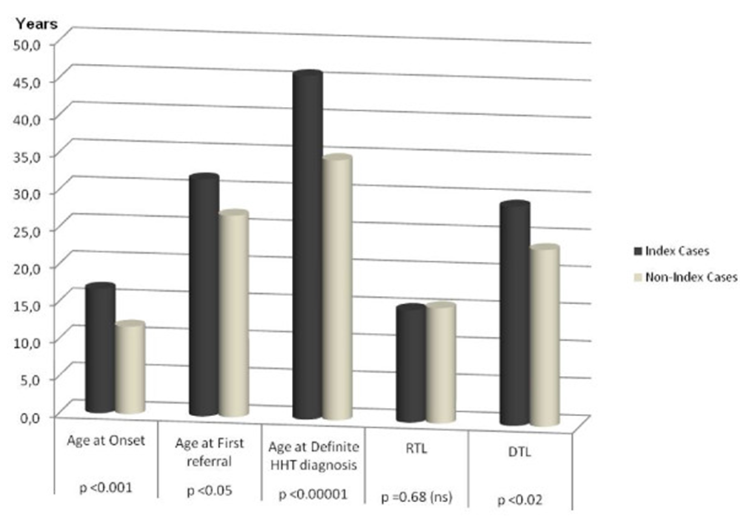
HHT is underdiagnosed - only ~1/10 affected individuals carry the dx - and has significant delays in dx - estimated >25 year delay from sx to dx
No FDA-approved therapies exist
Few randomized trials have been done, and even fewer, are powered appropriately
3/
No FDA-approved therapies exist
Few randomized trials have been done, and even fewer, are powered appropriately
3/
First systemic therapy 👉antifibrinolytics
For mild-mod epistaxis or GIB, tranexamic acid is a mainstay
ATERO is the largest TXA study, randomizing 118 pts in cross-over design, and showing 17% shorter epistaxis duration - a modest but significant effect on epistaxis
4/
For mild-mod epistaxis or GIB, tranexamic acid is a mainstay
ATERO is the largest TXA study, randomizing 118 pts in cross-over design, and showing 17% shorter epistaxis duration - a modest but significant effect on epistaxis
4/
Antifibrinolytic quick notes:
➡️Pill burden creates a real adherence issue (TXA is q8, ε-ACA is q6)
➡️Thromboembolic risk exists theoretically but hasn’t been borne out in trials
➡️ε-ACA likely has similar efficacy but is less well-studied in HHT
sciencedirect.com
5/
➡️Pill burden creates a real adherence issue (TXA is q8, ε-ACA is q6)
➡️Thromboembolic risk exists theoretically but hasn’t been borne out in trials
➡️ε-ACA likely has similar efficacy but is less well-studied in HHT
sciencedirect.com
5/
Antiangiogenic therapies target the pathobiology of telangiectasia and AVM via VEGF signaling, though it’s somewhat unclear whether VEGF directly affects pathogenesis or causes a “second hit” on angiogenesis on in the mutated BMP/TGF-β signaling pathway
6/
6/
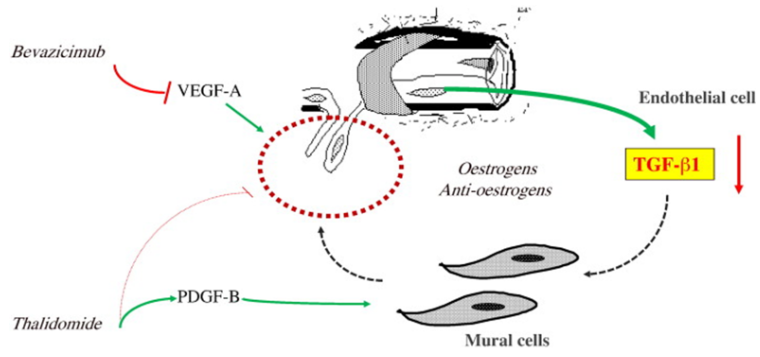
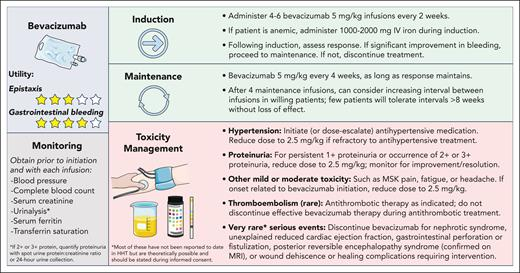
👉Bevacizumab (bev)
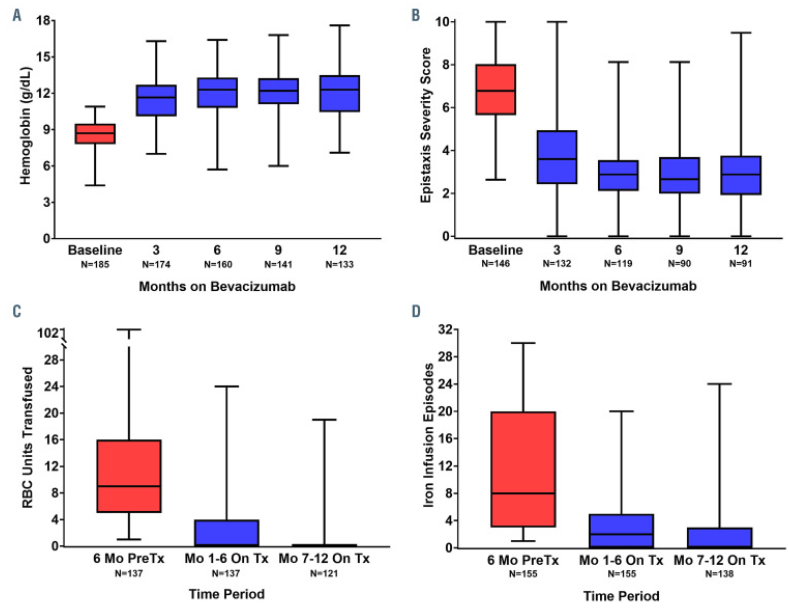
Bev is an anti-VEGF mAb that had prevalent off-label use in HHT preceding the multicenter retrospective InHIBIT-BLEED study, which showed improved anemia, ESS, and transfusions in a pre/post analysis
ncbi.nlm.nih.gov
7/
Bev is an anti-VEGF mAb that had prevalent off-label use in HHT preceding the multicenter retrospective InHIBIT-BLEED study, which showed improved anemia, ESS, and transfusions in a pre/post analysis
ncbi.nlm.nih.gov
7/

The phase 2 TRUST-HHT study is currently recruiting to study the efficacy of bev on RBC transfusion and iron infusion dependence in a prospective pre/post design
This should certainly offer more reliable point estimates of its efficacy than are currently available
8/
This should certainly offer more reliable point estimates of its efficacy than are currently available
8/
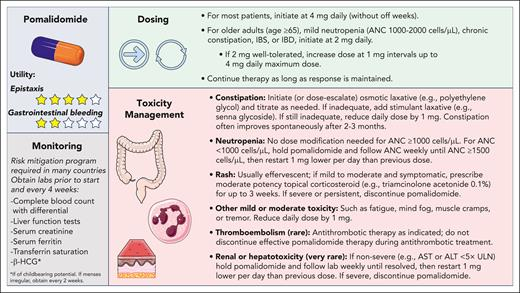
👉Pomalidomide (pom) has antiangiogenic and immunomodulatory effects just like thalidomide, which has shown efficacy in phase 2 study in HHT
PATH-HHT was published in @NEJM this week!
Topline results:
9/
PATH-HHT was published in @NEJM this week!
Topline results:
9/
144 pts with HHT, epistaxis severity score (ESS) >3 at baseline, and anemia or iron/pRBC dependence were randomized 2:1 to pom vs. placebo with a primary outcome of ESS with results showing a mean difference in ESS of -0.94 at 24 wks
(min important diff in ESS is 0.71)
10/
(min important diff in ESS is 0.71)
10/
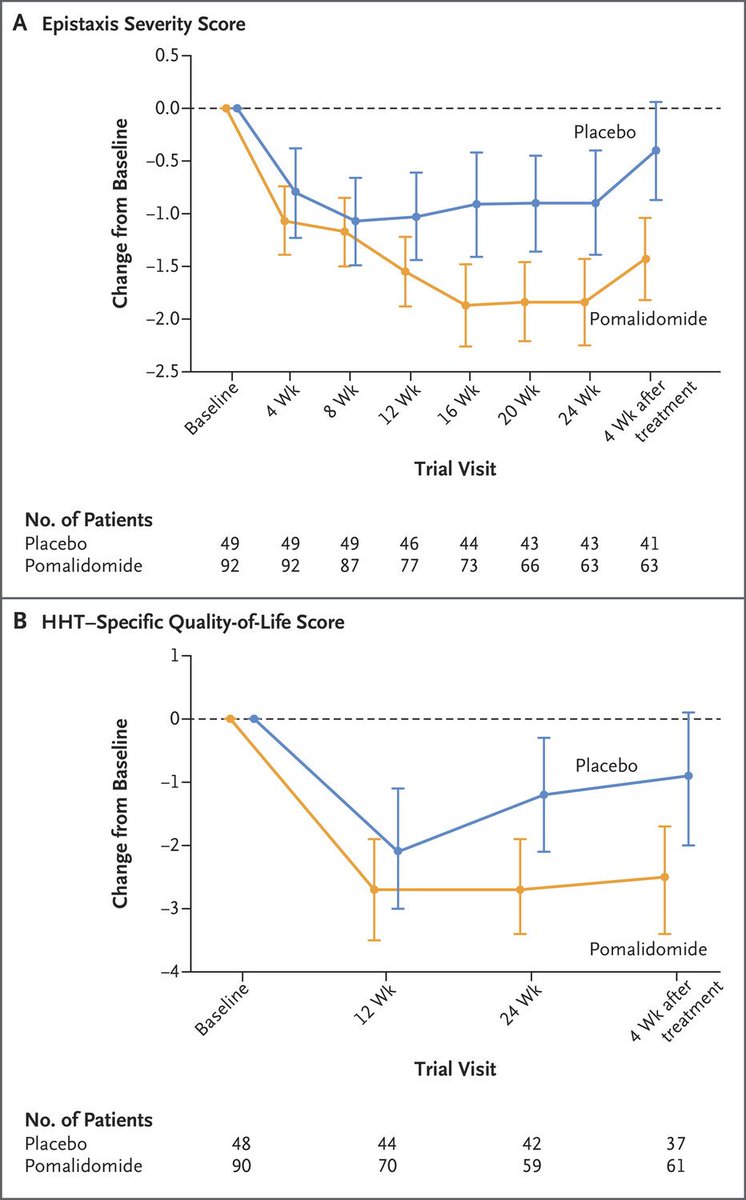
Cohen's d=0.57, indicating medium effect size
ESS diff becomes apparent ~12 wks after pom initiation and even maintains at 1 month post-treatment, suggestive of persistent effect, perhaps via improved vascular integrity, continued VEGF or bFGF suppression, or other MoA...?
11/
ESS diff becomes apparent ~12 wks after pom initiation and even maintains at 1 month post-treatment, suggestive of persistent effect, perhaps via improved vascular integrity, continued VEGF or bFGF suppression, or other MoA...?
11/
There’s a notable discontinuation rate for pom, which isn’t unexpected but seems a bit higher than in myeloma...maybe that’s due to continuous dosing vs MM 3 wk on / 1 wk off dosing ? Open to other ideas here.
Maybe we just have higher thresholds for holding cancer therapy?
12/
Maybe we just have higher thresholds for holding cancer therapy?
12/
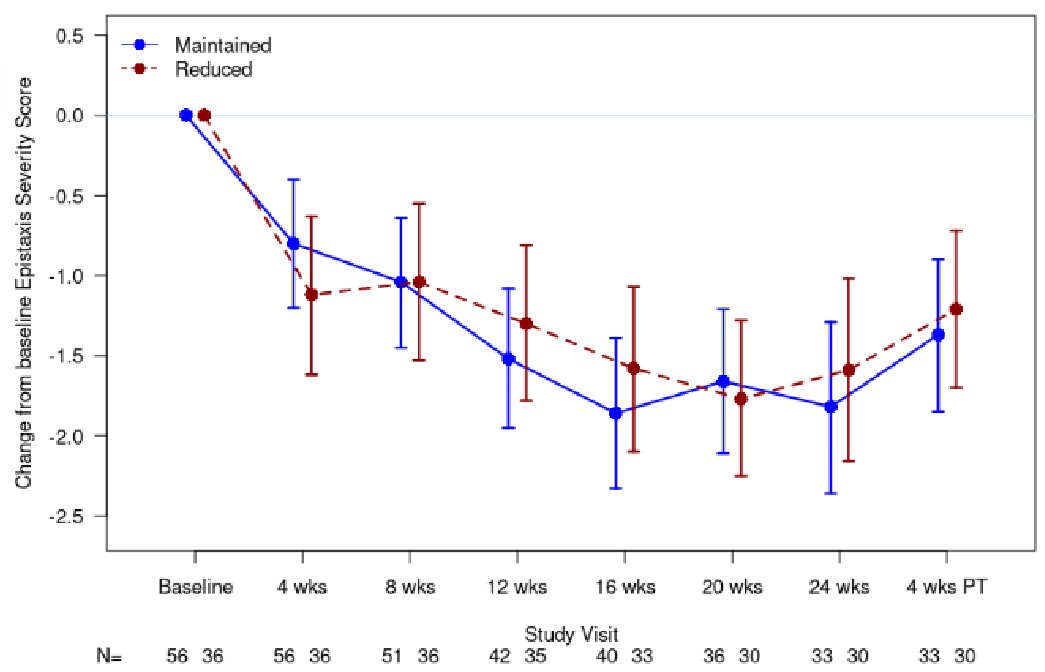
Pom was discontinued in 16%, interrupted in 40%, and dose reduced in 13% owing to adverse events
Those who had doses reduced had similar efficacy-- maybe doses lower than 4mg would better balance efficacy and safety
13/
Those who had doses reduced had similar efficacy-- maybe doses lower than 4mg would better balance efficacy and safety
13/
It’s encouraging that there was a low rate of thrombosis in this trial as HHT predisposes to VTE and IMiDs have increased thrombosis risk in MM trials
Likewise, neutropenia was quickly reversible and seemed to have low infxn risk
14/
Likewise, neutropenia was quickly reversible and seemed to have low infxn risk
14/
Eventually, studies will compare bev and pom, hopefully in randomized design, but in the meantime, comorbidities and preferences are salient to shared decision-making
Expert opinion suggests bev is preferred for GIB vs pom for epistaxis
How may comorbidities sway you?
15/
Expert opinion suggests bev is preferred for GIB vs pom for epistaxis
How may comorbidities sway you?
15/
CHF, uncontrolled HTN, osteoporosis requiring antiresorptive tx, and nephrotic syndromes may favor pom over bev
Pre-existing neutropenia or thrombocytopenia, EtOH use, constipation, IBS, or IBD may favor bev over pom
16/
Pre-existing neutropenia or thrombocytopenia, EtOH use, constipation, IBS, or IBD may favor bev over pom
16/
There are no approved therapies for HHT but a few others of note:
👉Pazopanib - antiangiogenic TKI, esp targeting VEGF-R
👉Octreotide / lanreotide - somatostatin analogs with observational data on ⬇️GIB
👉Thalidomide - IMiD with worse safety profile than pom - bye!👋
17/
👉Pazopanib - antiangiogenic TKI, esp targeting VEGF-R
👉Octreotide / lanreotide - somatostatin analogs with observational data on ⬇️GIB
👉Thalidomide - IMiD with worse safety profile than pom - bye!👋
17/
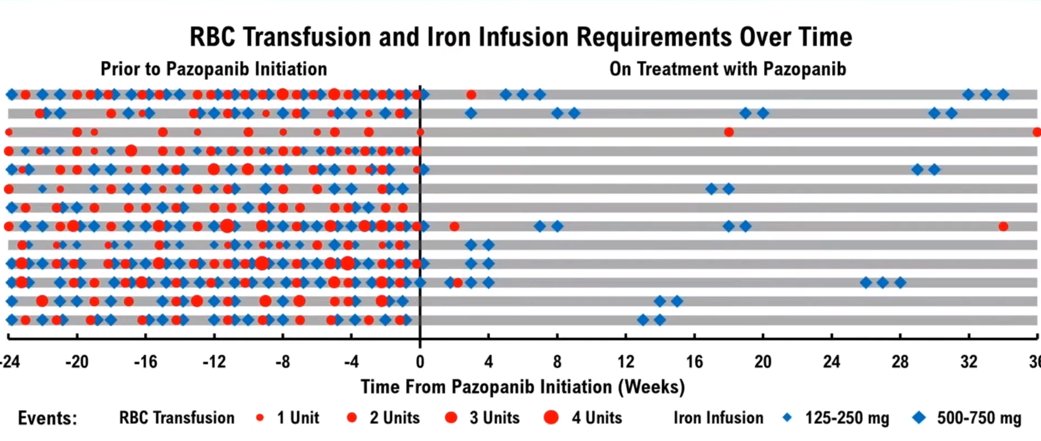
Pazopanib is currently in a placebo-controlled phase 2/3 trial (NCT03850964) at very low dose relative to dosing across malignancies
Prior observational data suggests its utility in reducing transfusion dependence
ncbi.nlm.nih.gov
18/
Prior observational data suggests its utility in reducing transfusion dependence
ncbi.nlm.nih.gov
18/

Finally, I’ll leave estrogens/SERMs aside for a later deep dive as data is mixed across small studies and there’s a notable thrombotic risk
Doxycycline is often considered as well but has negative results across a couple trials
19/
Doxycycline is often considered as well but has negative results across a couple trials
19/
The ability for the trial to recruit enough participants in a condition as rare as HHT speaks to the collaborative nature of the HHT Centers of Excellence model and to patient organizations like @CureHHT that raise awareness and fund research
#raredisease
20/
#raredisease
20/
A round of applause for the authors on conducting a randomized and well-powered study for a systemic agent in a rare disease - a labor of love surely. Such data doesn’t exist for bevacizumab or pazopanib yet, but soon it may!
A great recent ref: ashpublications.org
end!
A great recent ref: ashpublications.org
end!

Loading suggestions...