

1/
25-yo M p/w status epilepticus.
He has been paranoid and confused in the previous weeks.
MRI 👇. A large abdominal mass was identified on imaging.
You know what this is, but do you know why we treat it the way we do?
A #ContinuumCase on immunomodulators
25-yo M p/w status epilepticus.
He has been paranoid and confused in the previous weeks.
MRI 👇. A large abdominal mass was identified on imaging.
You know what this is, but do you know why we treat it the way we do?
A #ContinuumCase on immunomodulators

2/
ok ok, everyone gets to vote on what's going on before we dive in on how we are going to treat it and why.
so what do you think?
ok ok, everyone gets to vote on what's going on before we dive in on how we are going to treat it and why.
so what do you think?
3/
Anti-NMDA receptor encephalitis is caused by anti-neural antibodies against the cell surface proteins (in this cause the NMDA receptor) this causes in a stereotyped way a progression through
⭐️Psychosis
⭐️Seizures
⭐️Sympathetic storming
⭐️Orofacial dystonias
Anti-NMDA receptor encephalitis is caused by anti-neural antibodies against the cell surface proteins (in this cause the NMDA receptor) this causes in a stereotyped way a progression through
⭐️Psychosis
⭐️Seizures
⭐️Sympathetic storming
⭐️Orofacial dystonias
4/
Like many suspected autoimmune cases, the patient was treated with 1g IV methylprednisolone for 5 days.
Why?
Broad anti-inflammatory effects! And BONUS: steroids help restore the blood-brain barrier integrity
Like many suspected autoimmune cases, the patient was treated with 1g IV methylprednisolone for 5 days.
Why?
Broad anti-inflammatory effects! And BONUS: steroids help restore the blood-brain barrier integrity

5/
The 1g/kg methylprednisolone has been routinely used. I honestly can’t find any great evidence for why we use this dose. So if anyone has insight, please share.
However steroids cause insomnia, hyperglycemia, mania, weight gain etc.. this is not a long term solution.
The 1g/kg methylprednisolone has been routinely used. I honestly can’t find any great evidence for why we use this dose. So if anyone has insight, please share.
However steroids cause insomnia, hyperglycemia, mania, weight gain etc.. this is not a long term solution.

5/
The patient is then treated with plasma exchange every other day for 5 days.
Why?
This is an antibody-mediated disease.
PLEX removes circulating antibodies+ immune complexes, cytokines ➡️➡️reducing the amp’ed up immune system.
The patient is then treated with plasma exchange every other day for 5 days.
Why?
This is an antibody-mediated disease.
PLEX removes circulating antibodies+ immune complexes, cytokines ➡️➡️reducing the amp’ed up immune system.
6/
For PLEX: ☝️ reminder that you need to stop ACE inhibitors (otherwise risk for bradykinin mediated hypotension).
Other SE include CVL complications, hemodynamic instability, and hypofibrinogenemia and hypoMg and Ca
For PLEX: ☝️ reminder that you need to stop ACE inhibitors (otherwise risk for bradykinin mediated hypotension).
Other SE include CVL complications, hemodynamic instability, and hypofibrinogenemia and hypoMg and Ca
7/
Of these, I think the one to worry most about is the hypofibrinogenemia – it can be managed with cryoprecipitate to keep the fibrinogen level > 150.
I have personally seen this cause bleeding and severe complications. not great. but this is preventable!
Of these, I think the one to worry most about is the hypofibrinogenemia – it can be managed with cryoprecipitate to keep the fibrinogen level > 150.
I have personally seen this cause bleeding and severe complications. not great. but this is preventable!
8/
IVIG works in a different way, but basically neutralizes antibodies.
It wouldn’t have been wrong to use IVIG here. But sometimes we then get tempted to try a different induction immunosuppressant if the first one doesn't work
IVIG and *then* PLEX is a silly thing to do.
IVIG works in a different way, but basically neutralizes antibodies.
It wouldn’t have been wrong to use IVIG here. But sometimes we then get tempted to try a different induction immunosuppressant if the first one doesn't work
IVIG and *then* PLEX is a silly thing to do.

9/
Whereas PLEX and then IVIG…?
I dunno, you probably aren’t getting a lot of bang for your buck (research in GBS would suggest more immunosuppression is not better).
But, you also aren’t just flushing away the expense treatment you previously gave.
💸💸💸💸
Whereas PLEX and then IVIG…?
I dunno, you probably aren’t getting a lot of bang for your buck (research in GBS would suggest more immunosuppression is not better).
But, you also aren’t just flushing away the expense treatment you previously gave.
💸💸💸💸
10/
Both steroids and PLEX (and IVIG for that matter) are induction medications. They work relatively quickly, but will not have long term modulation effects.
Often patients are put on 60mg of prednisone and a steroid sparing agent.
But which one to choose????
Both steroids and PLEX (and IVIG for that matter) are induction medications. They work relatively quickly, but will not have long term modulation effects.
Often patients are put on 60mg of prednisone and a steroid sparing agent.
But which one to choose????
11/
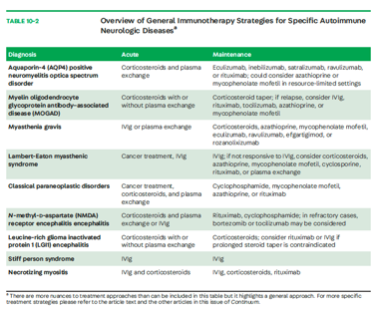
There are SO many new ones. And I do think, being thoughtful here really does matter. For example, NMOSD causes damage through complement activation and destruction. Using a c5 inhibitor like eculizumab makes sense (and is evidence based, PREVENT study)
There are SO many new ones. And I do think, being thoughtful here really does matter. For example, NMOSD causes damage through complement activation and destruction. Using a c5 inhibitor like eculizumab makes sense (and is evidence based, PREVENT study)
12/
For the paraneoplastic disorders like the tumor-associated NMDA receptor encephalitis in this case, the patient got what I think of as the “Keppra of immunosuppression” – rituximab.
So why do we like this drug so much??
For the paraneoplastic disorders like the tumor-associated NMDA receptor encephalitis in this case, the patient got what I think of as the “Keppra of immunosuppression” – rituximab.
So why do we like this drug so much??
13/
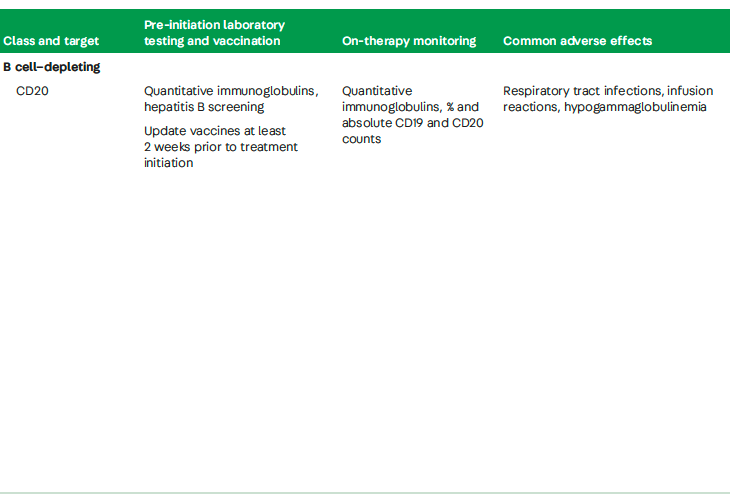
Rituximab is an anti-CD20 drug which means that it causes B-cell depletion. Other drugs in this class are ocrelizumab, ofatumumab and ublituximab. Of immunomodulators it has a relatively favorable side effect profile.
Rituximab is an anti-CD20 drug which means that it causes B-cell depletion. Other drugs in this class are ocrelizumab, ofatumumab and ublituximab. Of immunomodulators it has a relatively favorable side effect profile.
14/
However, it is important to screen for Hep B before initiation to prevent a fatal reactivation.
JCV causing PML is rare, but has been reported! You must consider this for new neurologic symptoms after treatment
However, it is important to screen for Hep B before initiation to prevent a fatal reactivation.
JCV causing PML is rare, but has been reported! You must consider this for new neurologic symptoms after treatment

14/
Rituximab can also cause infusion reactions and by depleting B cells, makes the patients response to vaccines much lower.
This became a major concern in the COVID19 pandemic (!!) and it’s recommended that vaccines should be updated 2 weeks priot to tx.
Rituximab can also cause infusion reactions and by depleting B cells, makes the patients response to vaccines much lower.
This became a major concern in the COVID19 pandemic (!!) and it’s recommended that vaccines should be updated 2 weeks priot to tx.
15/
This is an excellent summary from the article:
This is an excellent summary from the article:
16/
This article by @StaceyLClardy and Tammy Smith, MD PhD is an in-depth look at all the new treatments: the evidence, what to watch for, & how to select an immunosuppressant with evidence!
I learned a ton and you will too!
journals.lww.com
This article by @StaceyLClardy and Tammy Smith, MD PhD is an in-depth look at all the new treatments: the evidence, what to watch for, & how to select an immunosuppressant with evidence!
I learned a ton and you will too!
journals.lww.com

Loading suggestions...