

1/10
A 60 y/o woman presents with subacute, progressive, severe hyponatremia (Na 118).
Let’s walk through an approach to this common problem.
A 60 y/o woman presents with subacute, progressive, severe hyponatremia (Na 118).
Let’s walk through an approach to this common problem.

2/10
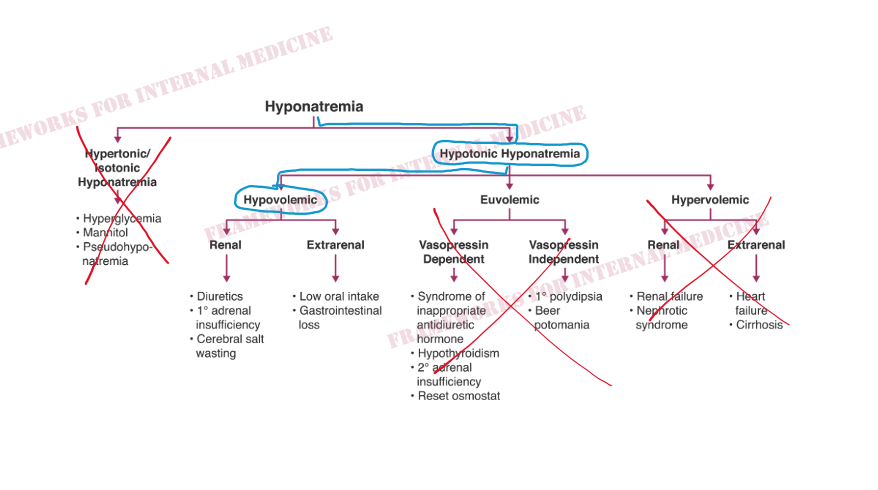
First we confirm we are dealing with hypotonic hyponatremia.
This begins to narrow our differential.
First we confirm we are dealing with hypotonic hyponatremia.
This begins to narrow our differential.


3/10
Next we want to know the status of extracellular fluid volume. Our patient has low JVP, no peripheral edema, and dry mucous membranes, narrowing our differential even further.
Next we want to know the status of extracellular fluid volume. Our patient has low JVP, no peripheral edema, and dry mucous membranes, narrowing our differential even further.
4/10
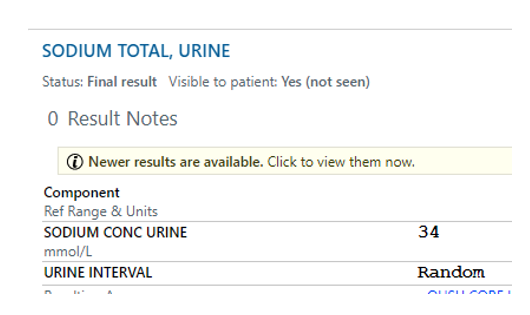
Is the hypovolemia renal or extrarenal? Urine sodium can be helpful here. Usually in the setting of hypovolemia, urine Na should be very low (usually <10) as the kidneys try to hold on to salt/water to preserve volume.
In our case, urine sodium is unexpectedly high at 34.
Is the hypovolemia renal or extrarenal? Urine sodium can be helpful here. Usually in the setting of hypovolemia, urine Na should be very low (usually <10) as the kidneys try to hold on to salt/water to preserve volume.
In our case, urine sodium is unexpectedly high at 34.
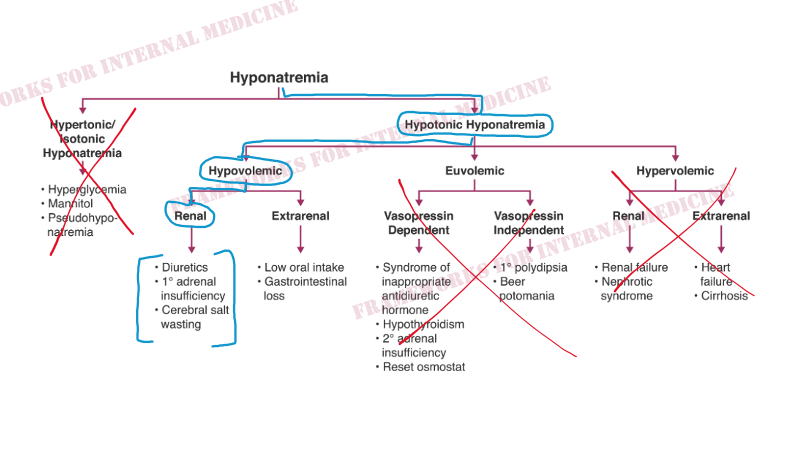
5/10
There are a few conditions in which hypovolemic hyponatremia is associated with an unexpectedly high urine Na, because the urine IS the source of the Na/fluid loss.
There are a few conditions in which hypovolemic hyponatremia is associated with an unexpectedly high urine Na, because the urine IS the source of the Na/fluid loss.
6/10
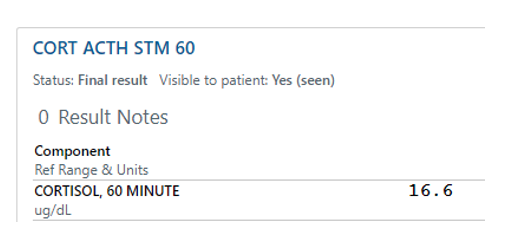
Our patient is not on diuretics. But she does have a history of RCC with nephrectomy/adrenalectomy, leaving a solitary adrenal gland. An ACTH stim test is in order.
It's positive (meaning that cortisol did not appropriately rise above 18), confirming adrenal insufficiency.
Our patient is not on diuretics. But she does have a history of RCC with nephrectomy/adrenalectomy, leaving a solitary adrenal gland. An ACTH stim test is in order.
It's positive (meaning that cortisol did not appropriately rise above 18), confirming adrenal insufficiency.
7/10
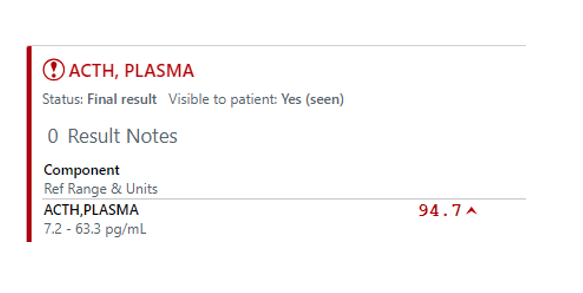
Plasma ACTH levels drawn prior to the stim test are elevated, indicating that we are dealing with primary (ACTH-independent) adrenal insufficiency.
Plasma ACTH levels drawn prior to the stim test are elevated, indicating that we are dealing with primary (ACTH-independent) adrenal insufficiency.
8/10
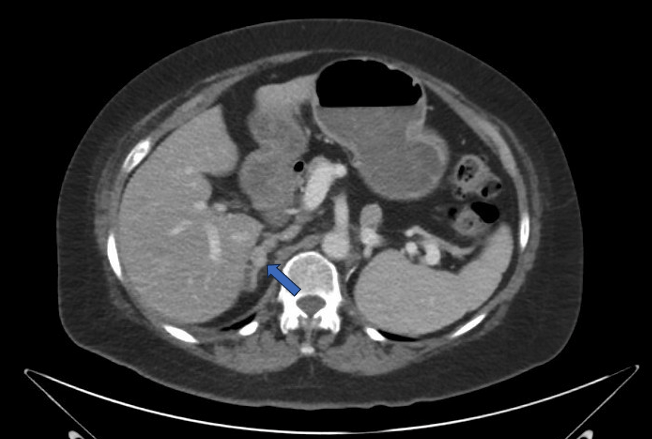
The solitary right adrenal gland is full of tumor (metastases from previously known RCC).
The solitary right adrenal gland is full of tumor (metastases from previously known RCC).
9/10
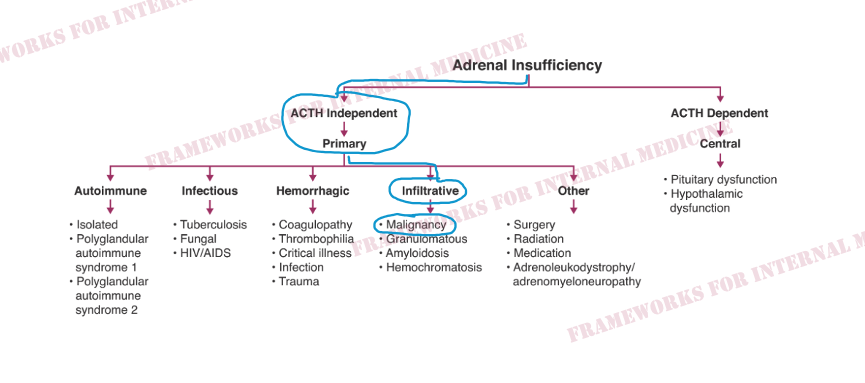
The cause of our patient’s hyponatremia is adrenal insufficiency secondary to malignant infiltration of the adrenal gland.
The cause of our patient’s hyponatremia is adrenal insufficiency secondary to malignant infiltration of the adrenal gland.
10/10
If you find these types of frameworks and approaches helpful, you might like this resource: #customerReviews" target="_blank" rel="noopener" onclick="event.stopPropagation()">amazon.com
If you find these types of frameworks and approaches helpful, you might like this resource: #customerReviews" target="_blank" rel="noopener" onclick="event.stopPropagation()">amazon.com
Loading suggestions...