


Mechanical valves can be classified as:
1st generation - Ball in cage
2nd generation - Single tilting disc
3rd generation - Bileaflet tilting disc
Although the first 2 are no longer used, many patients will have these valves, so it's important to know what they look like
1st generation - Ball in cage
2nd generation - Single tilting disc
3rd generation - Bileaflet tilting disc
Although the first 2 are no longer used, many patients will have these valves, so it's important to know what they look like
So, let's start with the ball in cage
Most famous version was the Starr Edwards valve
The ball moves up and down in systole & diastole, so even when the valve is 'open', blood has to flow around the ball - not exactly laminar flow!
Most famous version was the Starr Edwards valve
The ball moves up and down in systole & diastole, so even when the valve is 'open', blood has to flow around the ball - not exactly laminar flow!

Here is a TTE of a ball in cage valve in the mitral position, image courtesy of @BonitaEcho (from Twitter a few yrs ago)
You can see the ball moving up and down within the cage
You can see the ball moving up and down within the cage

Here is the mitral ball in cage valve as seen on TOE (TEE for 🇺🇲)
Note how the blood (as seen on colour Doppler) has to flow around the ball rather than through the middle of the valve
Note how the blood (as seen on colour Doppler) has to flow around the ball rather than through the middle of the valve

Now, moving on to single tilting disc valves
These are also no longer implanted, but the Bjork-Shiley was the most widely used mechanical prosthesis in the late 70s & early 80s so there remain many patients with these valves
These are also no longer implanted, but the Bjork-Shiley was the most widely used mechanical prosthesis in the late 70s & early 80s so there remain many patients with these valves

Here are PLAX & AP4Ch views on transthoracic echocardiography
You can clearly see only one disc opening & closing...
You can clearly see only one disc opening & closing...


So when this valve is open, there are two orifices for flow, a major (larger) one & a minor (smaller) one
I have slowed the colour Doppler loop so you can see the two flow jets in diastole...
I have slowed the colour Doppler loop so you can see the two flow jets in diastole...


For what it's worth, here is that single tilting disc on 3D TTE!

This is the appearance of a single tilting disc valve on TOE

Right, moving on to bileaflet tilting disc valves
In routine use for over 30 years
Note THREE orifices when open - a smaller central orifice & 2 slightly larger orifices, one on either side...
In routine use for over 30 years
Note THREE orifices when open - a smaller central orifice & 2 slightly larger orifices, one on either side...

Here is the typical appearance in the apical 4 chamber view
Note two occluders opening and closing...
Note two occluders opening and closing...

Here you can see clearly two discs (see arrows) and 3 distinct jets on colour Doppler imaging



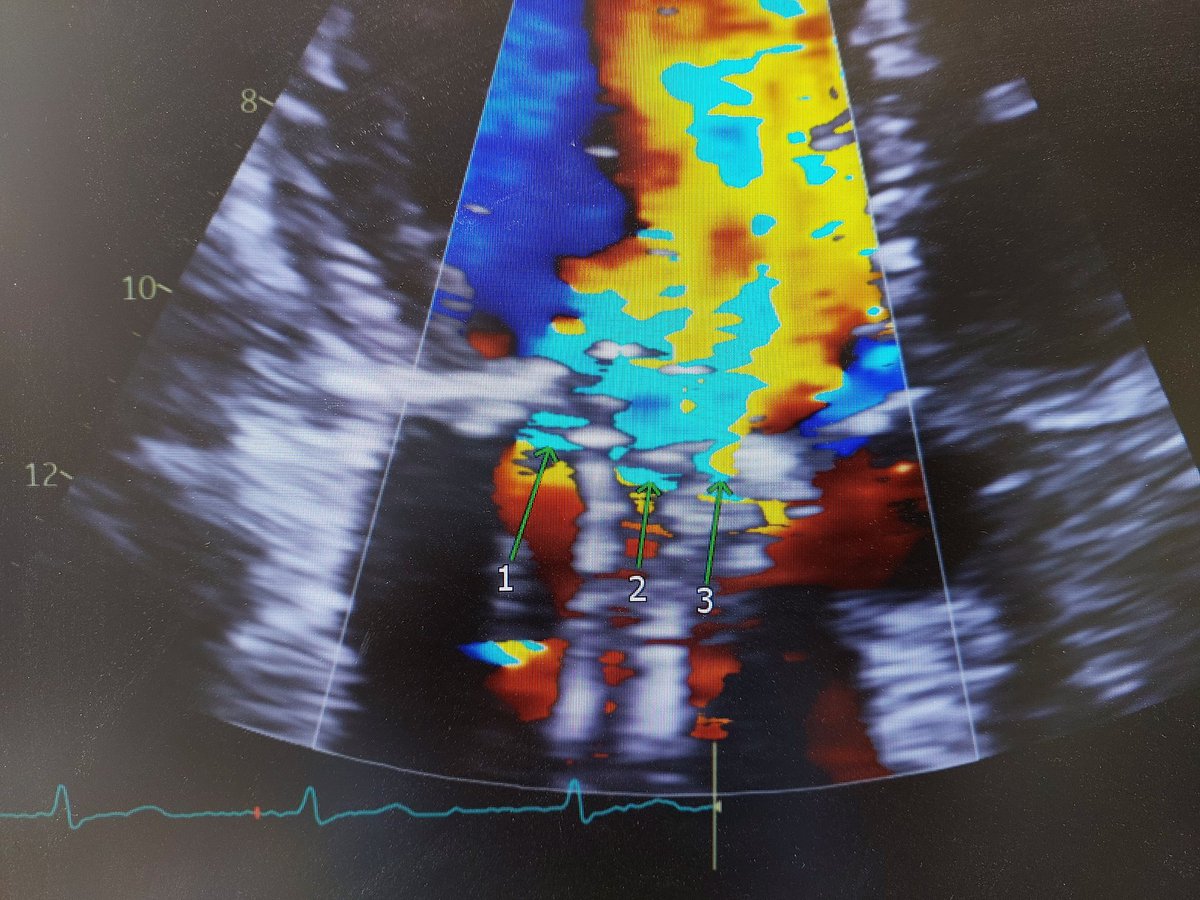
Here is the valve on transoesophageal imaging


Here is the colour Doppler still and 3D of a bileaflet mechanical valve


So, we've seen TTE & TOE images of all 3 generations of mechanical valve (for illustration I've stuck to mitral, these could of course be in the aortic position also)
Some other rules and tips to follow...
Some other rules and tips to follow...
Recall that in the apical views on TTE, a prosthetic mitral valve will invariably cause significant reverberation artefact across the LA, so colour Doppler should *not* be relied upon to detect mitral regurgitation (transvalvular or paravalvular)
There will be other clues...
There will be other clues...
Clues there is significant MR:
1) Physical signs (e.g. dynamic apex beat, pansystolic murmur)
2) Unusually dynamic/supranormal LV systolic function
3) Increased transmitral gradient
Recall, the MV gradient could be ⬆️ due to stenosis, regurgitation or tachycardia
1) Physical signs (e.g. dynamic apex beat, pansystolic murmur)
2) Unusually dynamic/supranormal LV systolic function
3) Increased transmitral gradient
Recall, the MV gradient could be ⬆️ due to stenosis, regurgitation or tachycardia
If it's stenosis, you may see hypomobility of an occluder on 2D imaging and the EF slope will be prolonged (long deceleration time)
In regurgitation, despite the high gradient the deceleration time will be shorter
This is often your main clue there is MR, and TOE may be needed
In regurgitation, despite the high gradient the deceleration time will be shorter
This is often your main clue there is MR, and TOE may be needed
Here is an old case illustrating this point quite nicely...
x.com
x.com
That's all! 😁
Loading suggestions...