

SEIZURE SEMIOLOGY #TWEETORIAL
#Epilepsy #Seizure #NeuroX
🧵1/ What is abdominal (or epigastric) aura?
Abdominal aura is characterized by an uncomfortable sensation in the abdominal region w/wo nausea and w/wo a characteristic 'rising' quality.
#Epilepsy #Seizure #NeuroX
🧵1/ What is abdominal (or epigastric) aura?
Abdominal aura is characterized by an uncomfortable sensation in the abdominal region w/wo nausea and w/wo a characteristic 'rising' quality.

2/ In majority of cases, this feeling is localized to the epigastric area, hence the other term 'epigastric aura'. #AurasInEpilepsy #SeizureSemiology


3/ The subjective descriptions of the abdominal aura are quite variable such as 'pain', 'nausea', 'sinking feeling', 'butterflies', 'fluttering', 'fullness', etc. Hence, this aura is mainly defined by the location of the body region affected, rather than type of sensation.


4/ Abdominal aura is one of the most commonly reported auras in epilepsy patients. In 1901, Gowers reported epigastric aura in 9.5% of all 2013 unselected cases of epilepsy. In selective studies of focal epilepsies, the prevalence is much higher 17-61%.
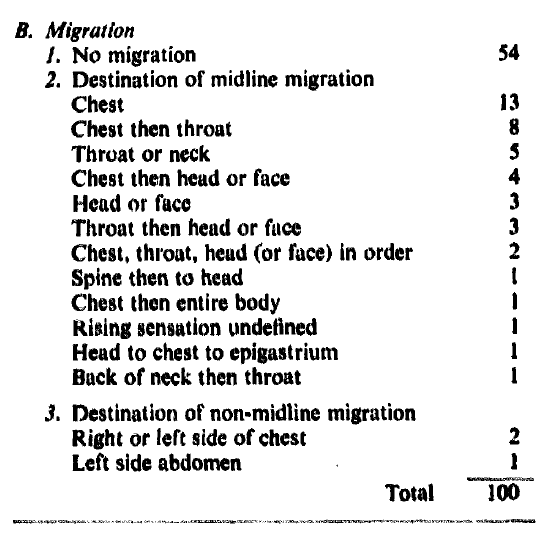
5/ In a detailed study of 100 patients with abdominal auras by Van Buren, ~54% did not report any migration, whereas in the other 46%, a rising quality was noted, upwards toward the thorax or throat, almost always remaining in the midline.
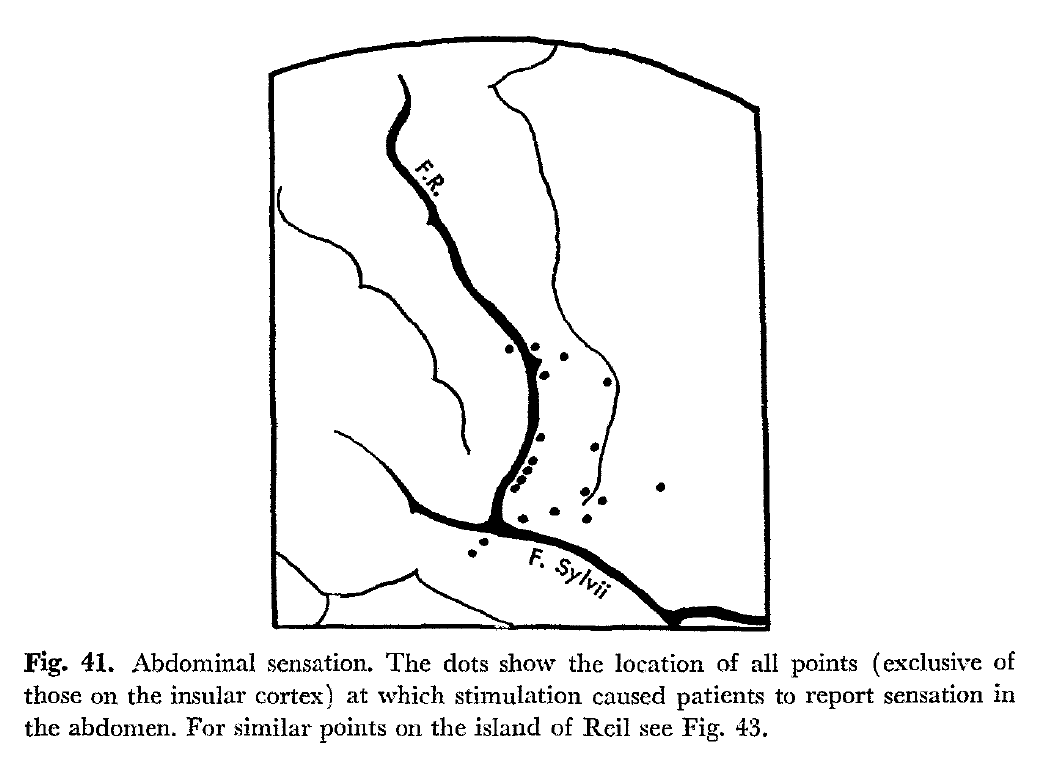
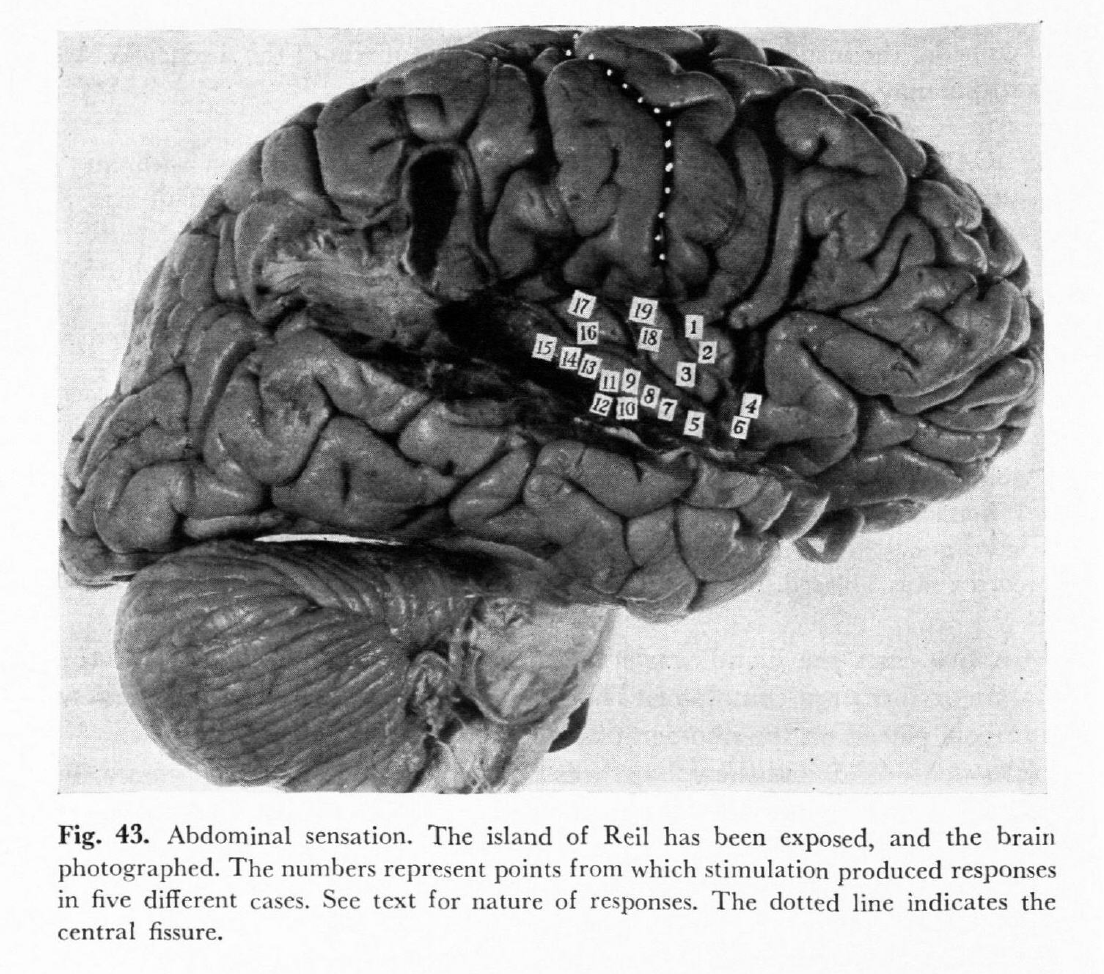
6/ The most likely symptomatogenic zone of the abdominal aura is the insula. The other potential candidate is the operculum along the superior bank of the sylvian fissure.

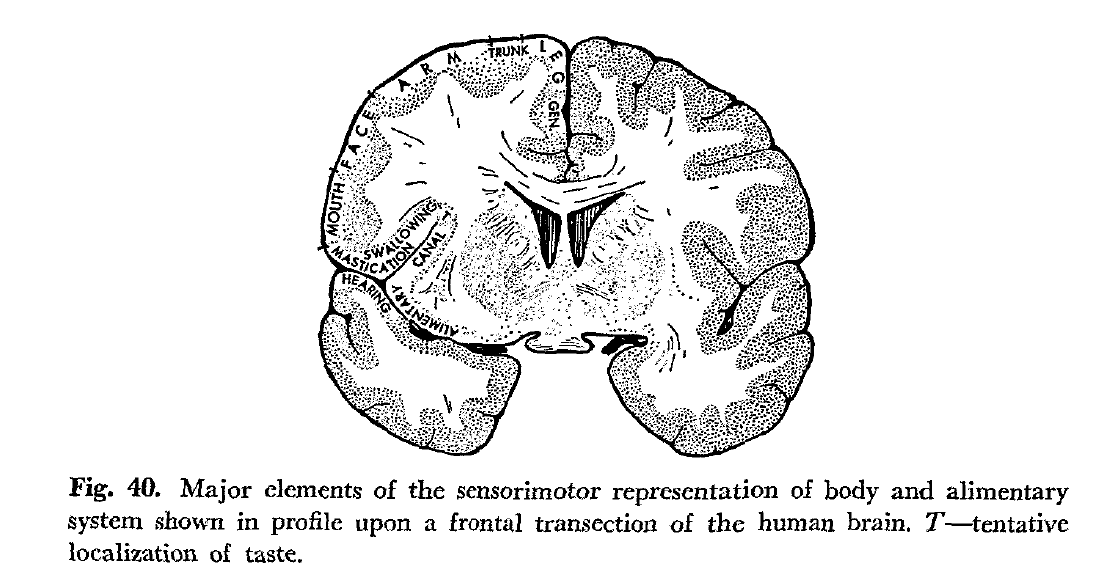
7/ According to Penfield & Rasmussen (1950), the representation of the visceral organs continues at the inferior end of the central sulcus after the mouth with the throat represented in the operculum. Sensory function is post-central and motor is pre-central.
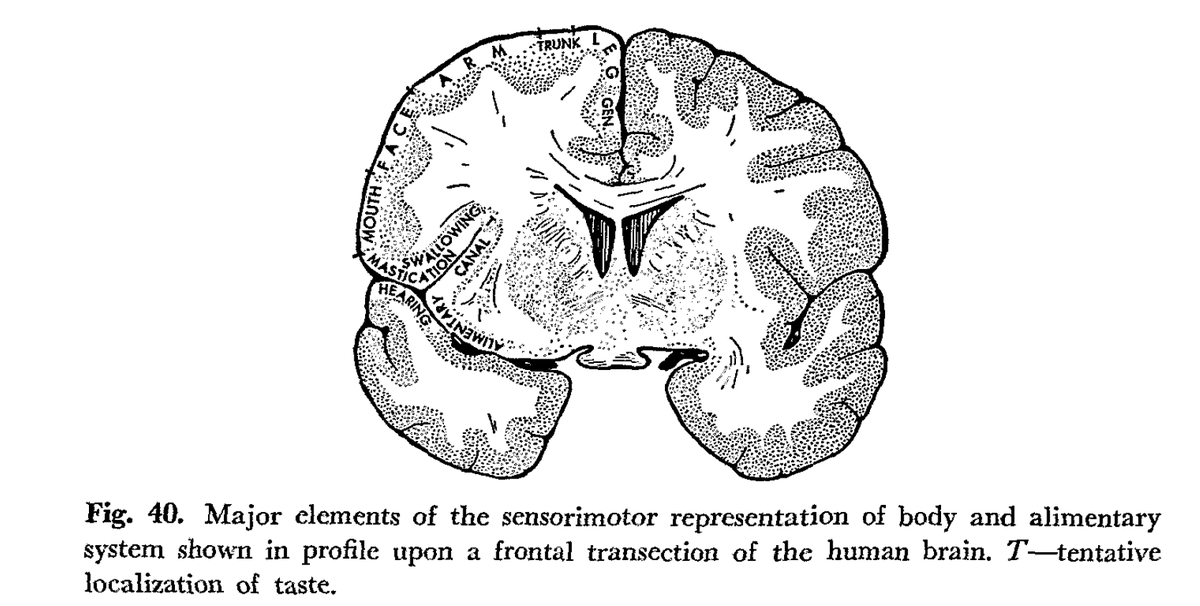
8/ Interestingly, Penfield and Rasmussen were able to reproduce abdominal sensations by stimulating near the inferior bank of the central sulcus but in the pre-central gyrus. However, it is important to note that they did not control for afterdischarges!

9/ They were also able to reproduce the abdominal aura by stimulating insula. Penfield & Rasmussen also postulated that the migration of epigastric sensation into throat was due to propagation of the discharge from insula into the superior bank of sylvian fissure (throat area).
10/ Van Buren was able to reproduce the abdominal aura sensation by stimulation of the mesial temporal lobe structures using depth electrodes, however, in many of these patients, he induced seizures as well.
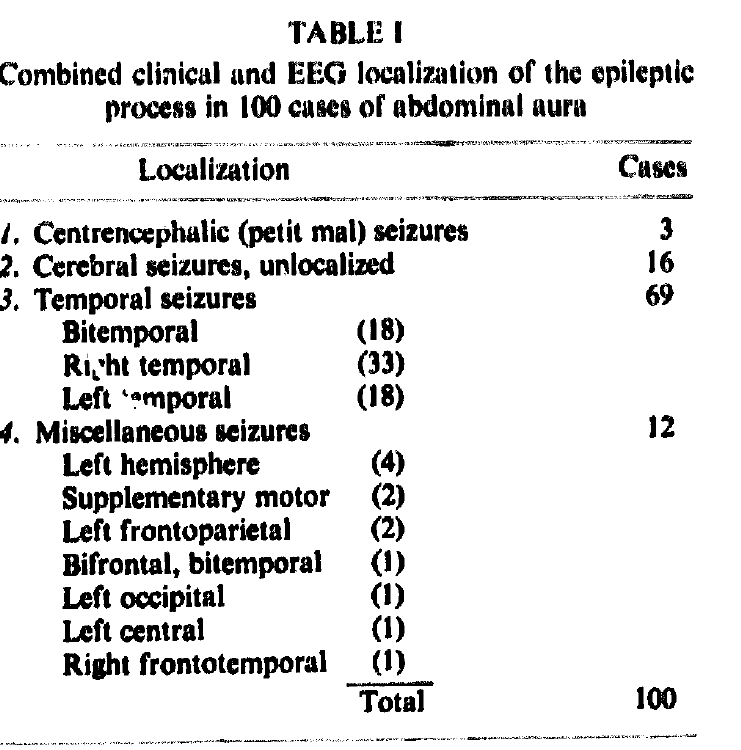
11/ The most common epileptogenic zone associated with abdominal auras is temporal lobe. This was first demonstrated systematically by Van Buren. 69 out of the 100 cases with abdominal auras had temporal lobe epilepsy.
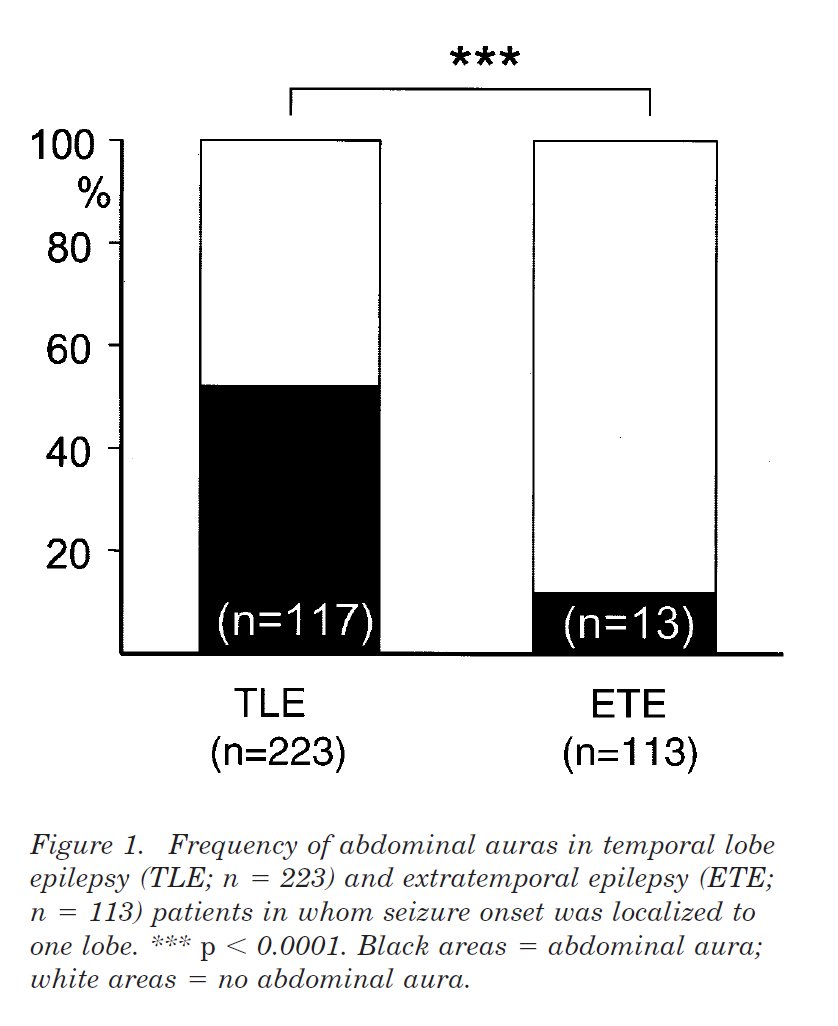
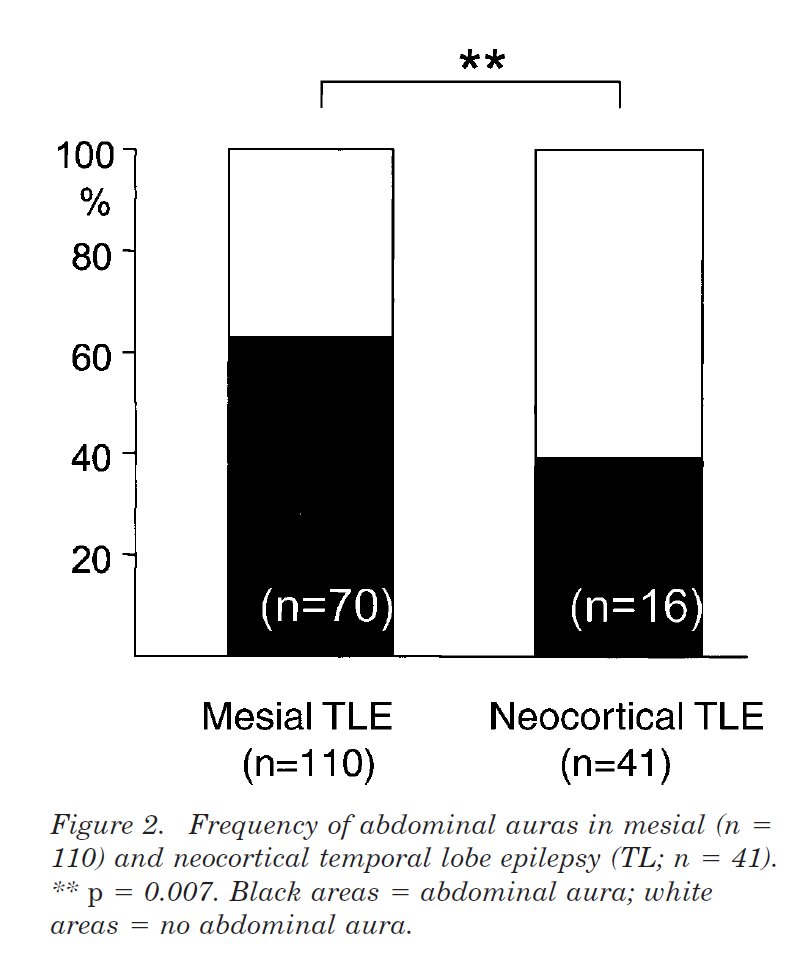
12/ In a very large study by Henkel, et al., out of a total of 491 patients, abdominal auras were much more common in TLE (52%) compared to extratemporal epilepsy (12%, p<0.0001). Also, abdominal auras were more common in mesial TLE v neocortical TLE (64% v 39%, p=0.007).
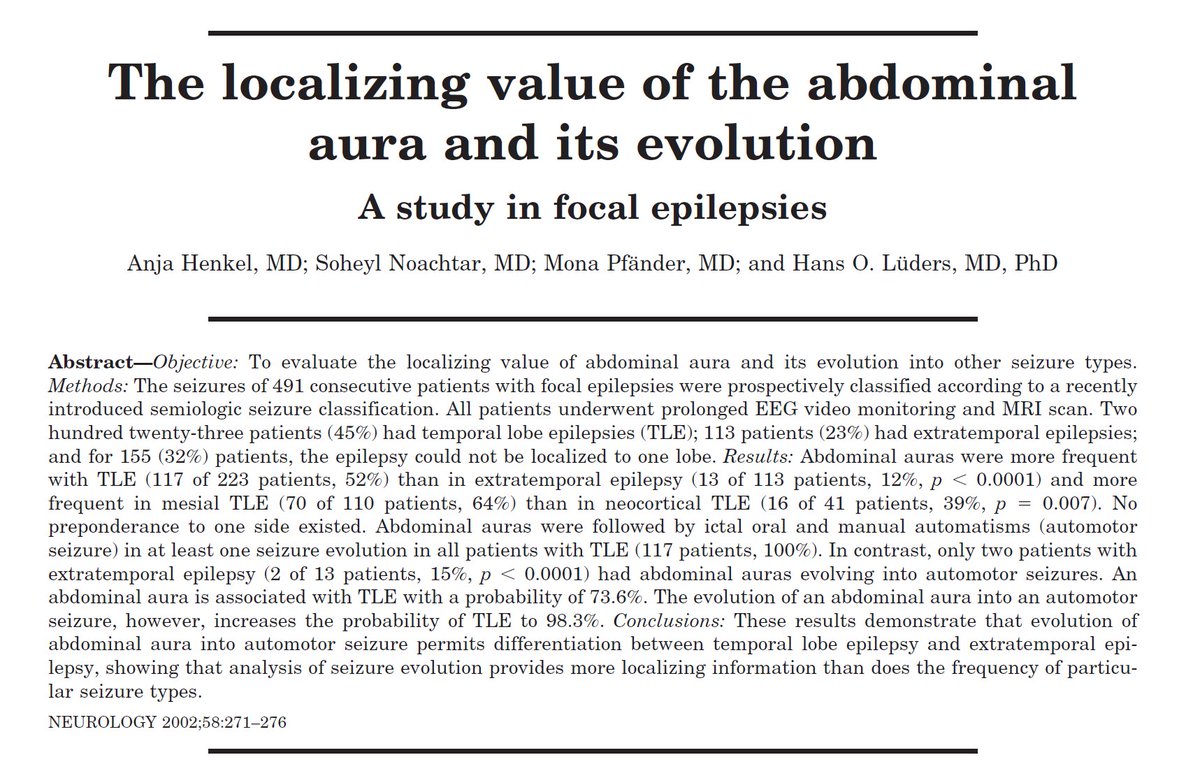
13/ The authors also noted that in patients with TLE, abdominal aura was followed by oroalimentary automatisms in 100% of cases as opposed to only 15% in extratemporal epilepsies (p<0.0001).
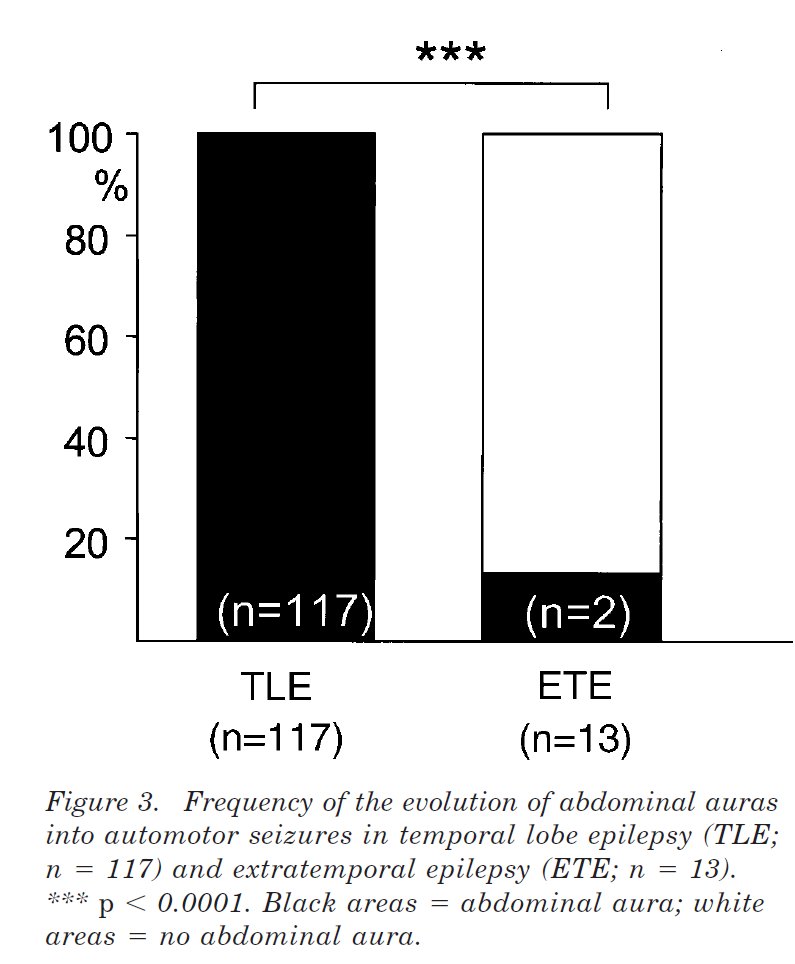
14/ Overall, abdominal auras in isolation increase the probability of TLE to 73.6%. However, the evolution of abdominal aura into oroalimentary automatisms increases the probability of TLE to 98.3%. This study, however, didn't find any lateralizing significance of abdominal aura.
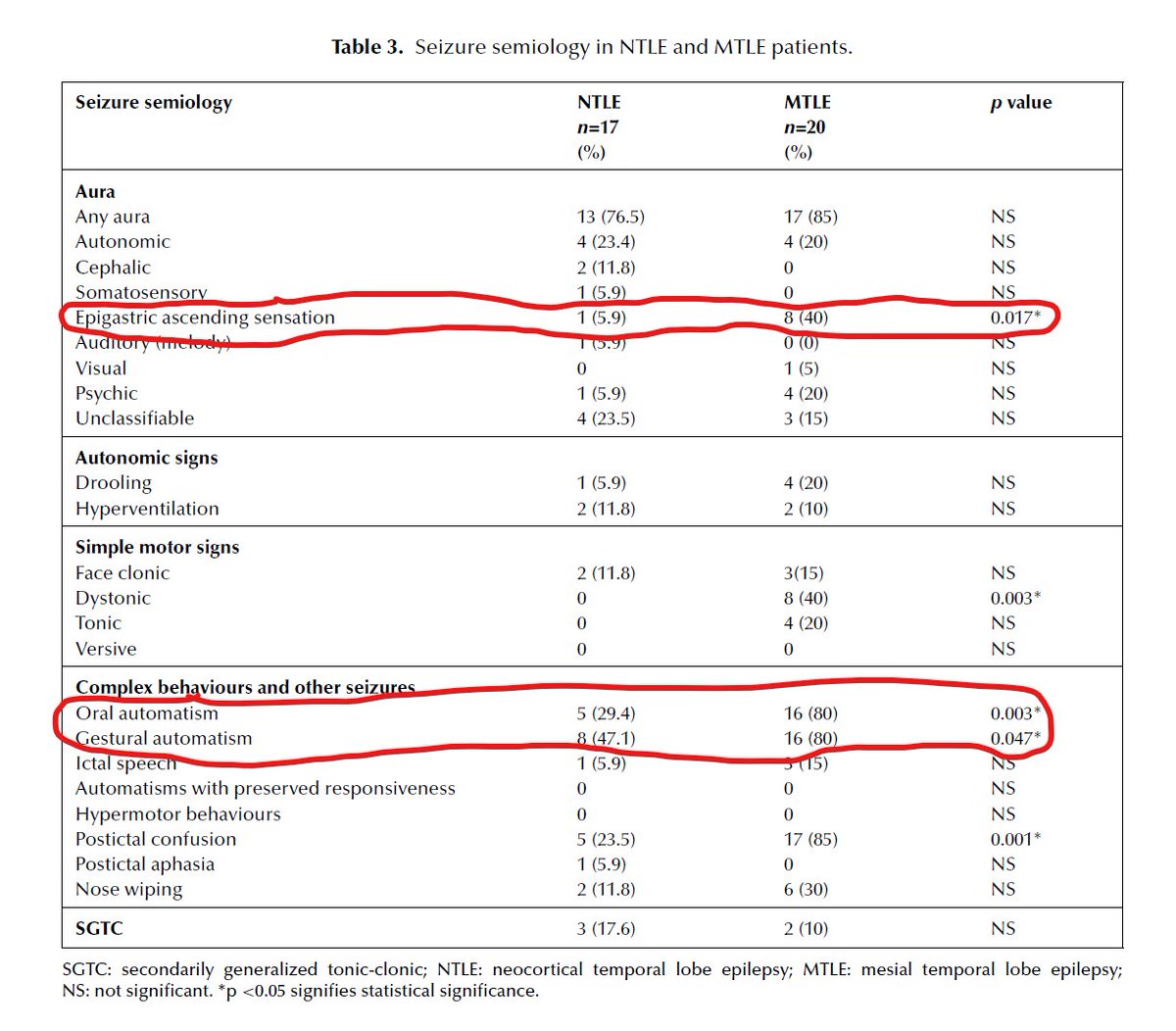
15/ In a different comparative study of pure mesial TLE v pure neocortical TLE, the epigastric ascending aura and oroalimentary automatisms were much more common in the mesial TLE cohort (40% v 6%, p=0.017 & 80% v 29%, p=0.003).
16/ Other less frequently associated epileptogenic zones reported with abdominal auras include mesial frontal, orbitofrontal and insula, varying between 19 to 30% of cases.
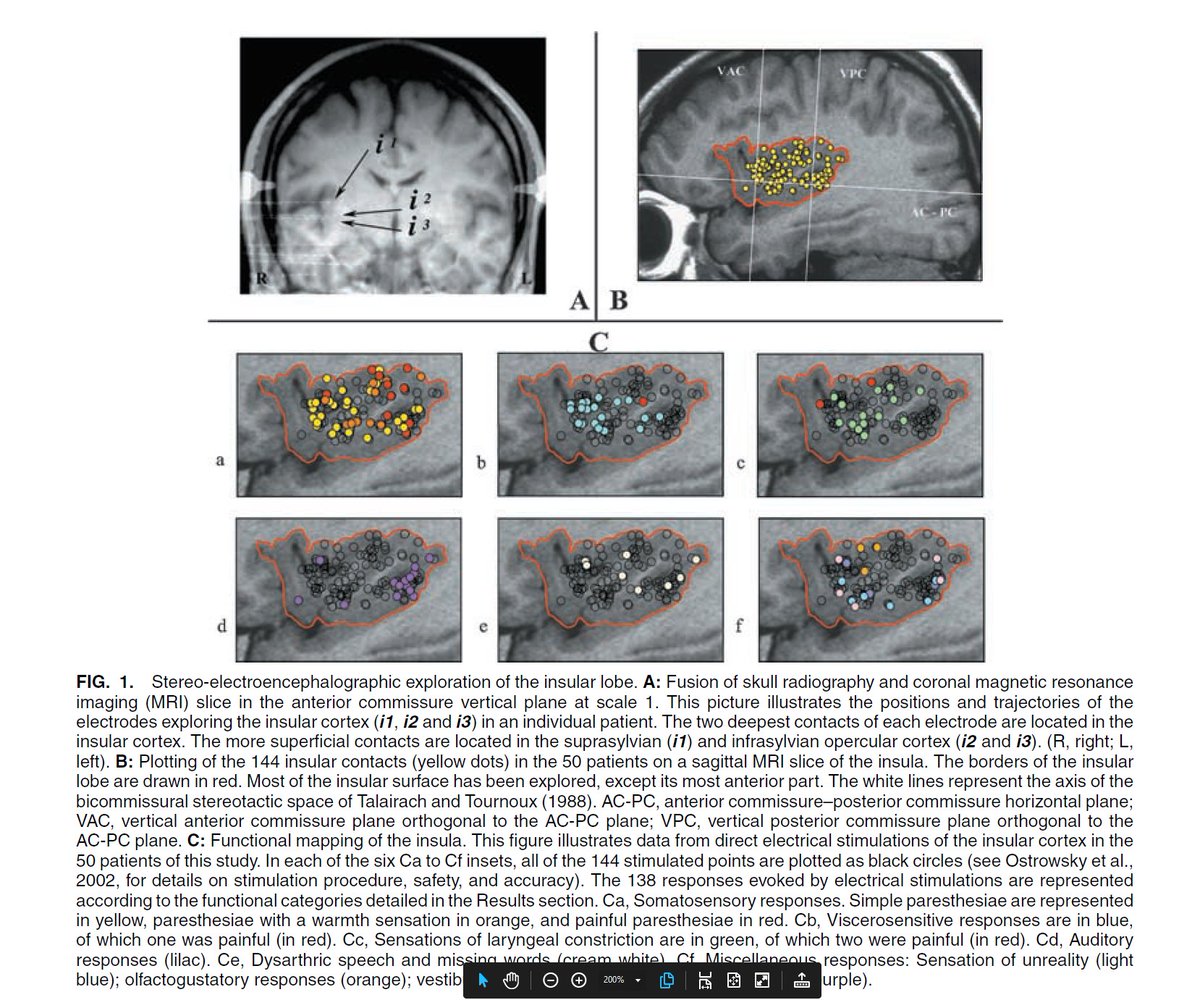
17/ Even though insula is the most likely symptomatogenic zone of abdominal aura, this is not the most frequent aura reported in most cases of insular epilepsy. The most frequently reported aura in these patients is the choking aura, produced by laryngeal constriction.
18/ Isnard, et al. were able to reproduce viscerosensitive responses in 22% of evoked responses with insular stimulation. About half of these were characterized by pharyngolaryngeal constriction and the other half were abdominal or thoracic sensations.
19/ Conclusion- Abdominal aura has a strong localizing value for the EZ being in the temporal lobe (mesial>>neocortical), especially when f/b oroalimentary automatisms. The most likely symptomatogenic zone is in the insula. It does not have any lateralizing significance.
جاري تحميل الاقتراحات...