

Getting my own talk from yesterday up late.
Also presented at the Big Beasts session on Community-Acquired Pneumonia.
Focused at stewardship folks but something in here for everyone 👇
#SHEASpring2024
#IDTwitter
#MedTwitter
1/
Also presented at the Big Beasts session on Community-Acquired Pneumonia.
Focused at stewardship folks but something in here for everyone 👇
#SHEASpring2024
#IDTwitter
#MedTwitter
1/

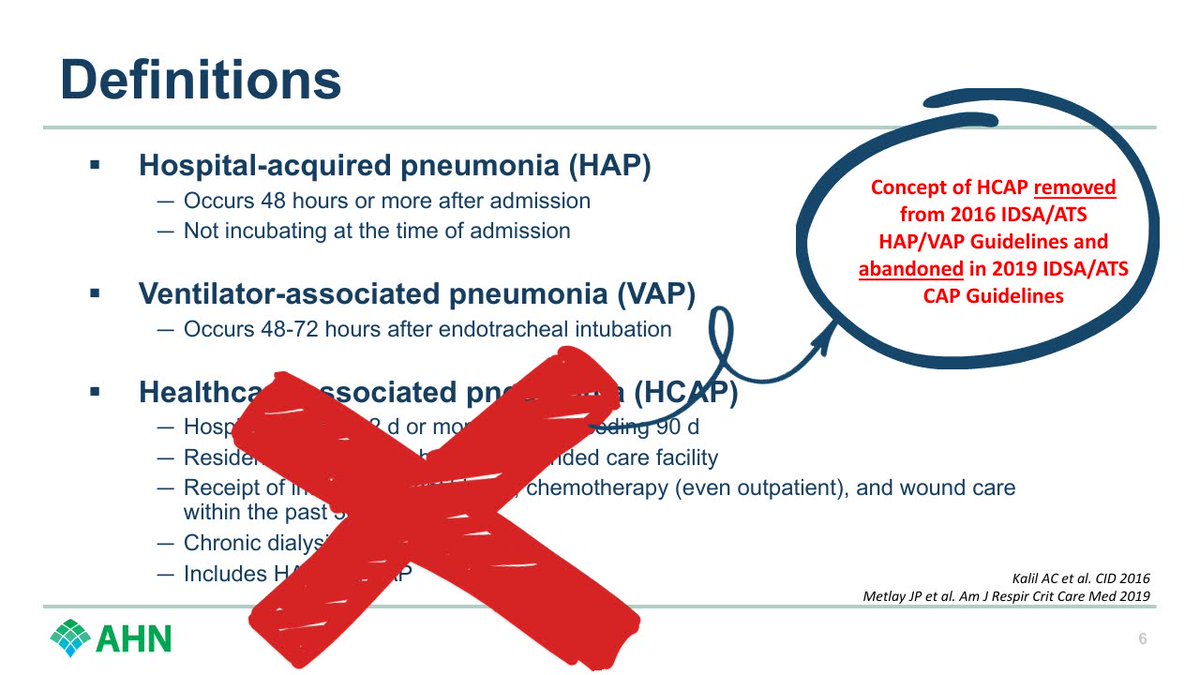
First up, quick definition:
➡️ Since HCAP is now dead, CAP is basically all pneumonia acquired outside of a hospital.
Lots of stuff can cause CAP, but viruses cause a LOT. Any virus that can cause an upper respiratory infection can also cause pneumonia.
#SHEASpring2024
2/
➡️ Since HCAP is now dead, CAP is basically all pneumonia acquired outside of a hospital.
Lots of stuff can cause CAP, but viruses cause a LOT. Any virus that can cause an upper respiratory infection can also cause pneumonia.
#SHEASpring2024
2/


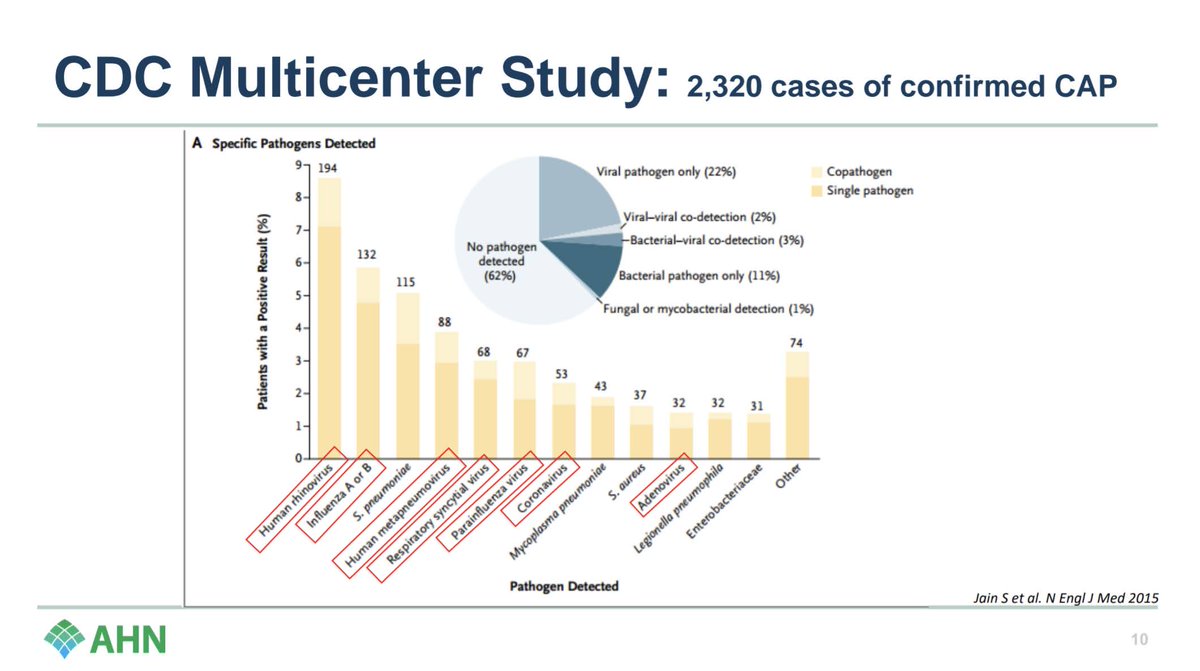
Check out this CDC study: when a pathogen was found, #1 cause?
Rhinovirus.
Flu was #2.
Strep pneumo is #3, then 4 more viruses before you hit another bacteria.
(This study is well pre-COVID, but rest assured it would be well represented now).
#SHEASpring2024
3/
Rhinovirus.
Flu was #2.
Strep pneumo is #3, then 4 more viruses before you hit another bacteria.
(This study is well pre-COVID, but rest assured it would be well represented now).
#SHEASpring2024
3/
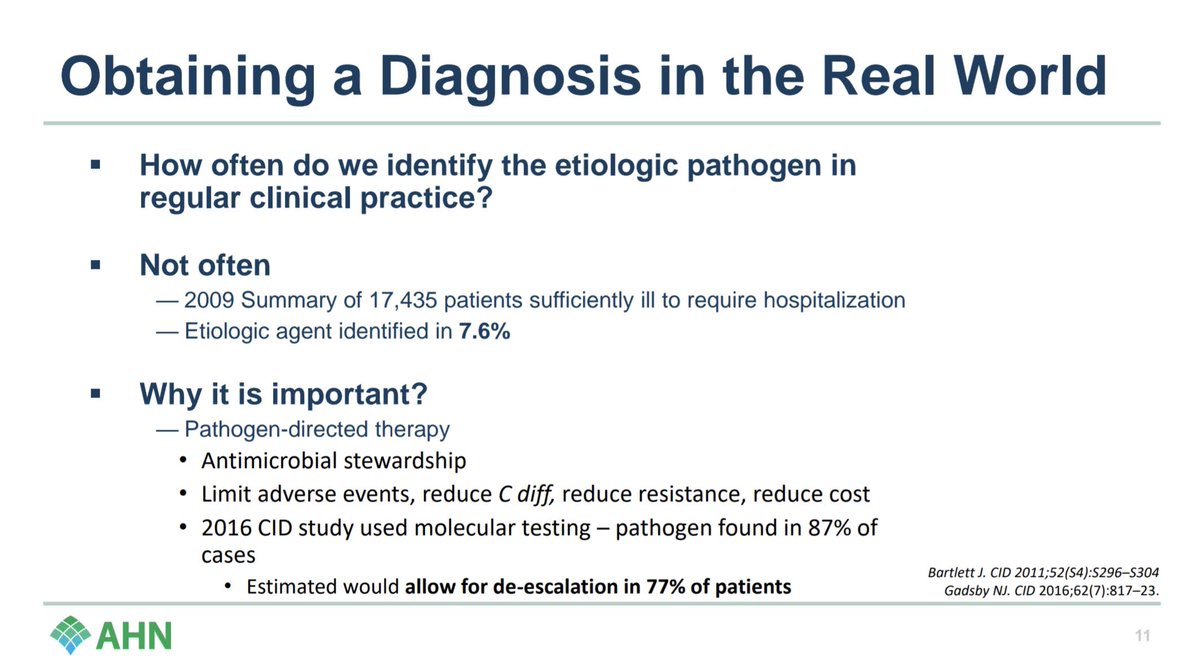
How do we do at getting a dx in the real world?
Not well at all. Can make de-escalation harder.
#SHEASpring2024
4/
Not well at all. Can make de-escalation harder.
#SHEASpring2024
4/
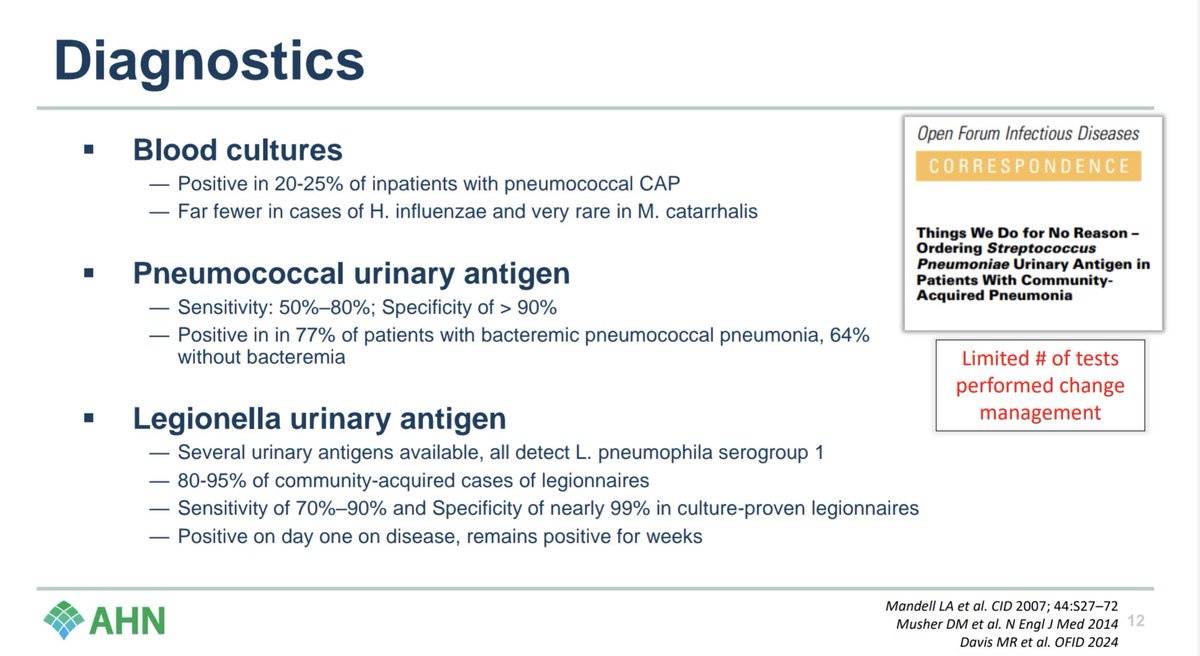
Let's look at the diagnostics we have: Blood cultures - overdone for pneumonia, not positive much.
Strep pneumo Ur Ag - can be helpful if +, but recent paper from @ErinMcCreary @MattDavis138 suggests doesn't change practice much in the real world.
#SHEASpring2024
5/
Strep pneumo Ur Ag - can be helpful if +, but recent paper from @ErinMcCreary @MattDavis138 suggests doesn't change practice much in the real world.
#SHEASpring2024
5/
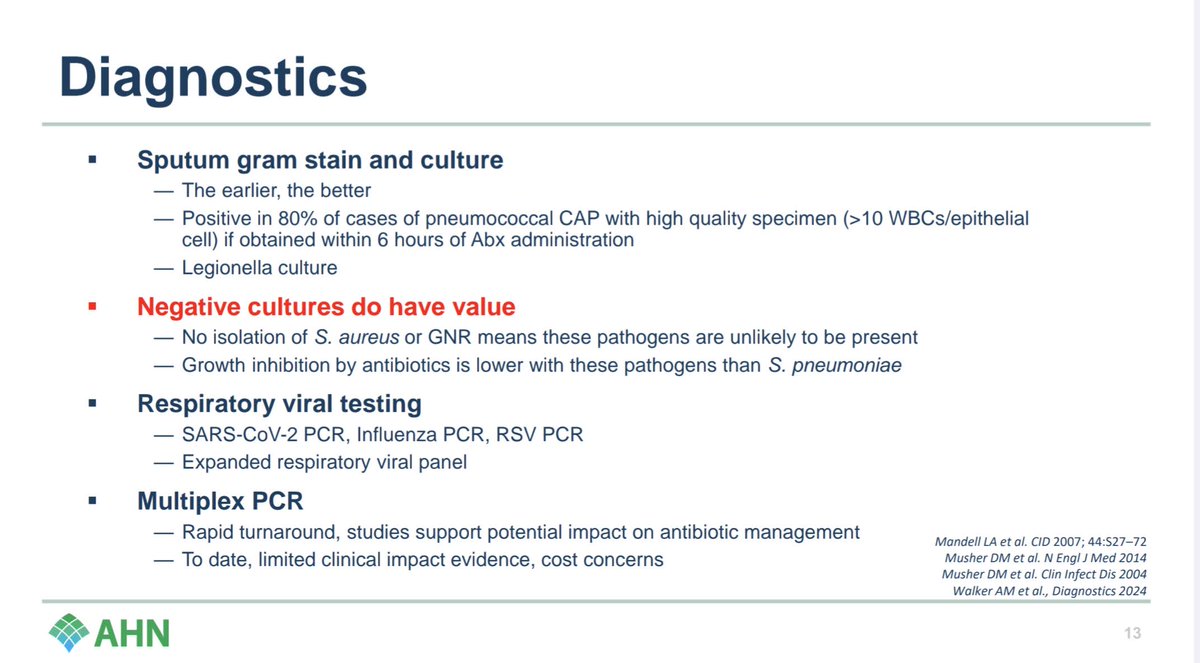
Sputum cultures - underdone. Make efforts to get them and get them early. Think induced sputum in the ED with 7% hypertonic saline.
Neg cultures have value. If no MRSA/PsA grow, they're not there.
Viral options and multiplex PCR ($$$) highlighted below.
#SHEASpring2024
6/
Neg cultures have value. If no MRSA/PsA grow, they're not there.
Viral options and multiplex PCR ($$$) highlighted below.
#SHEASpring2024
6/
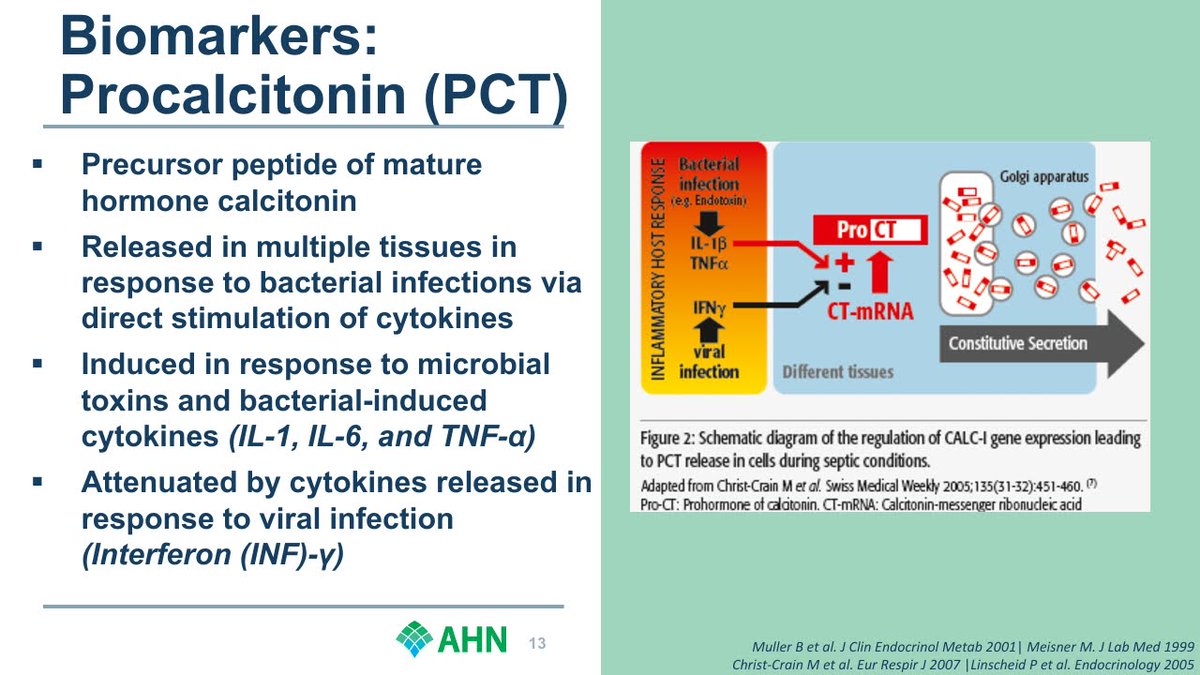
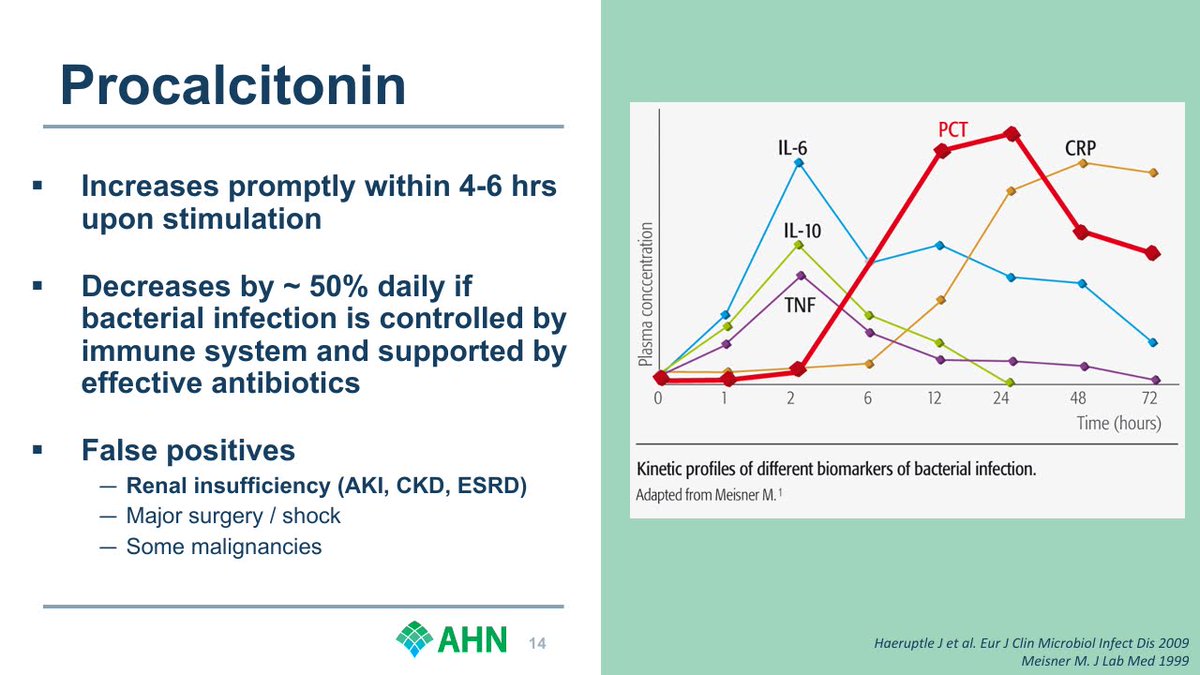
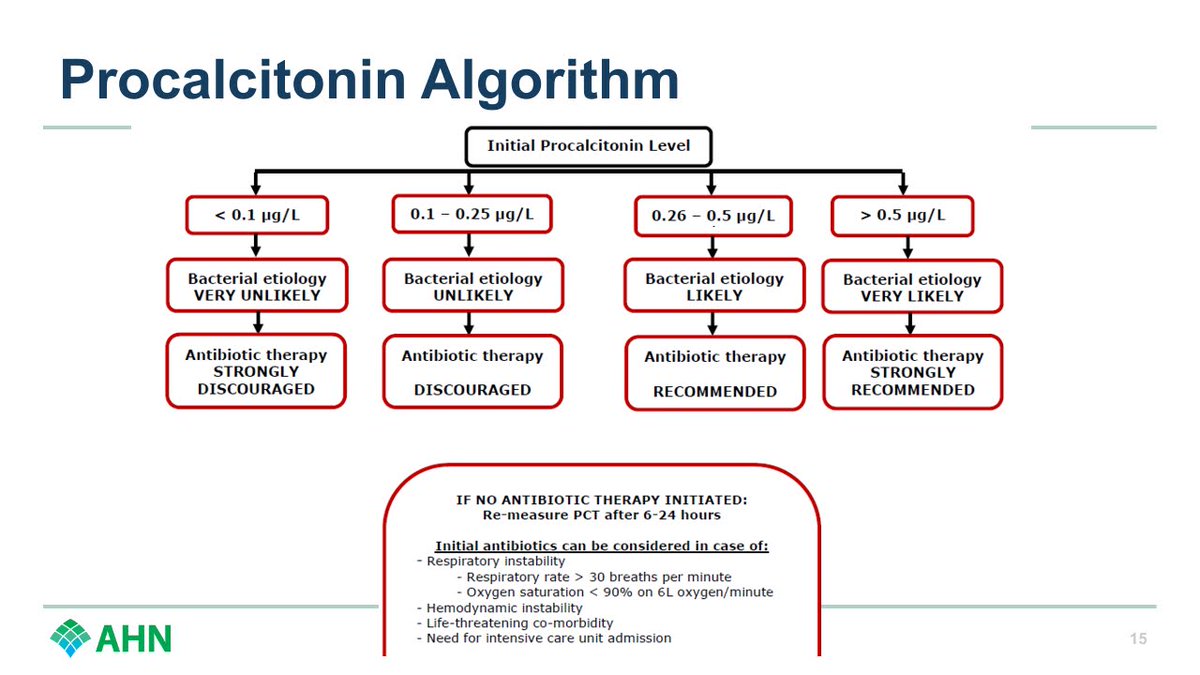
Let's talk about procalcitonin.
It's a biomarker that, when negative, suggests safe to stop/not give abx.
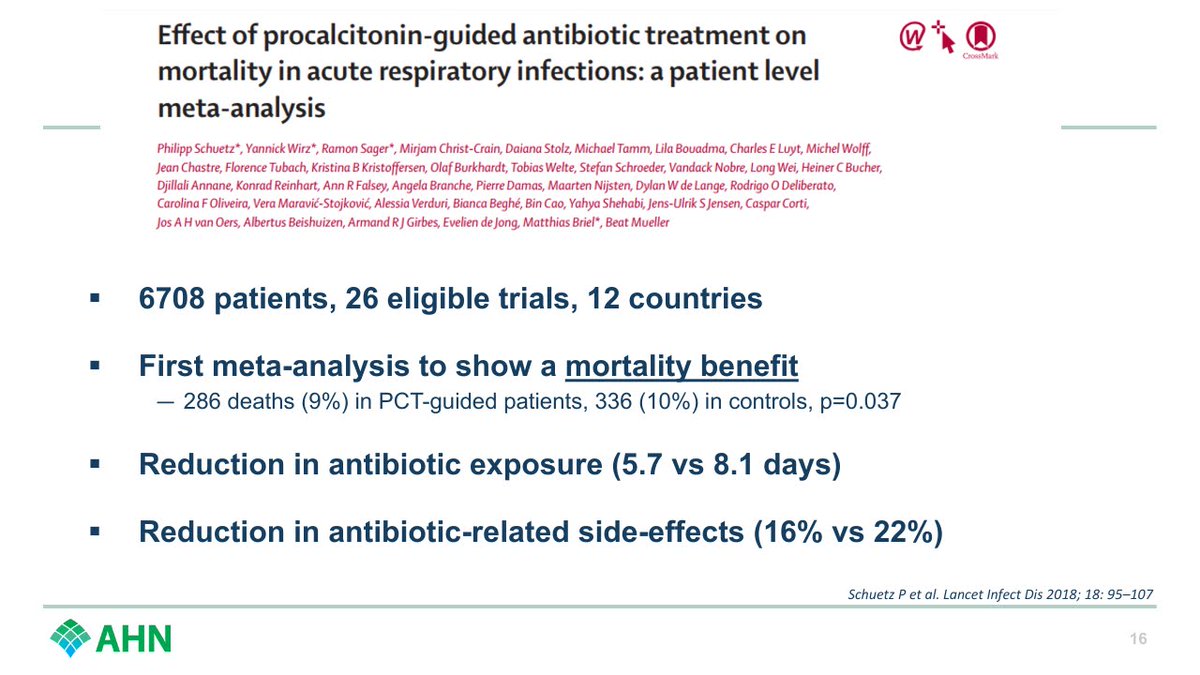
Meta-analysis below of 26 RCTs: PCT-guided = less abx, less adverse effects, less mortality.
Guess how many RCTs the CAP guidelines cite?
0 🤔
#SHEASpring2024
7/
It's a biomarker that, when negative, suggests safe to stop/not give abx.
Meta-analysis below of 26 RCTs: PCT-guided = less abx, less adverse effects, less mortality.
Guess how many RCTs the CAP guidelines cite?
0 🤔
#SHEASpring2024
7/
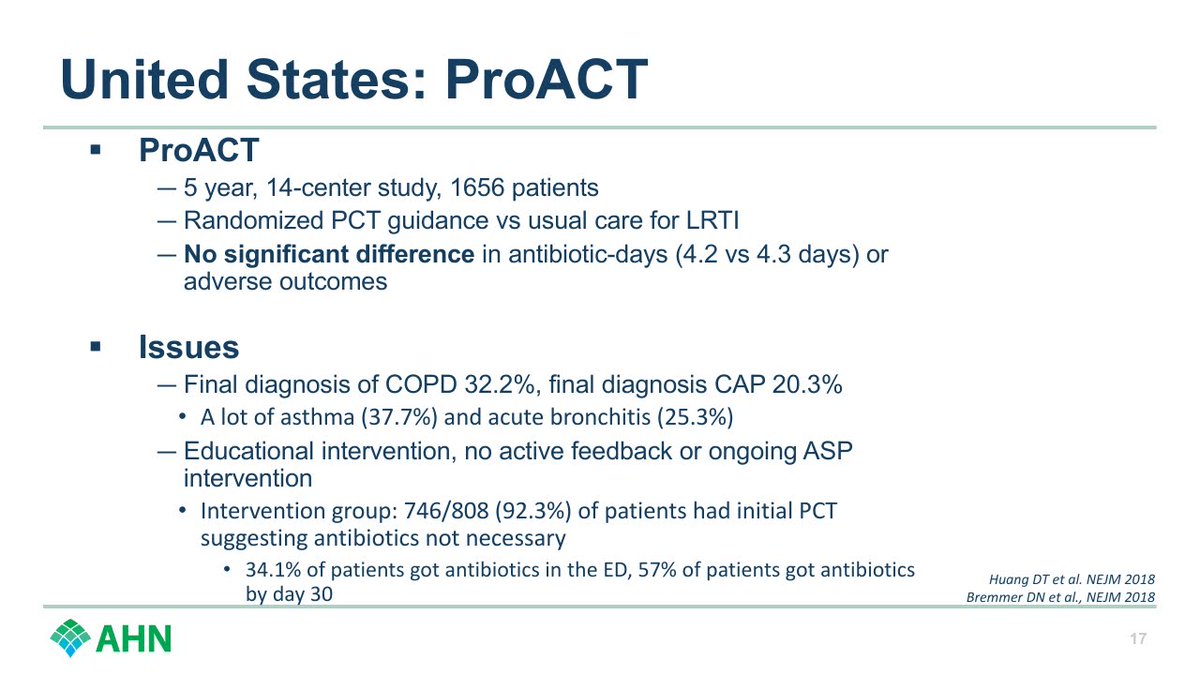
Negative trial in the US worth highlighting.
Some issues outlined here, but biggest is just educational intervention, no active ASP feedback in real time.
If you're going to use PCT, you need an ASP team reaching out to teams.
#SHEASpring2024
8/
Some issues outlined here, but biggest is just educational intervention, no active ASP feedback in real time.
If you're going to use PCT, you need an ASP team reaching out to teams.
#SHEASpring2024
8/
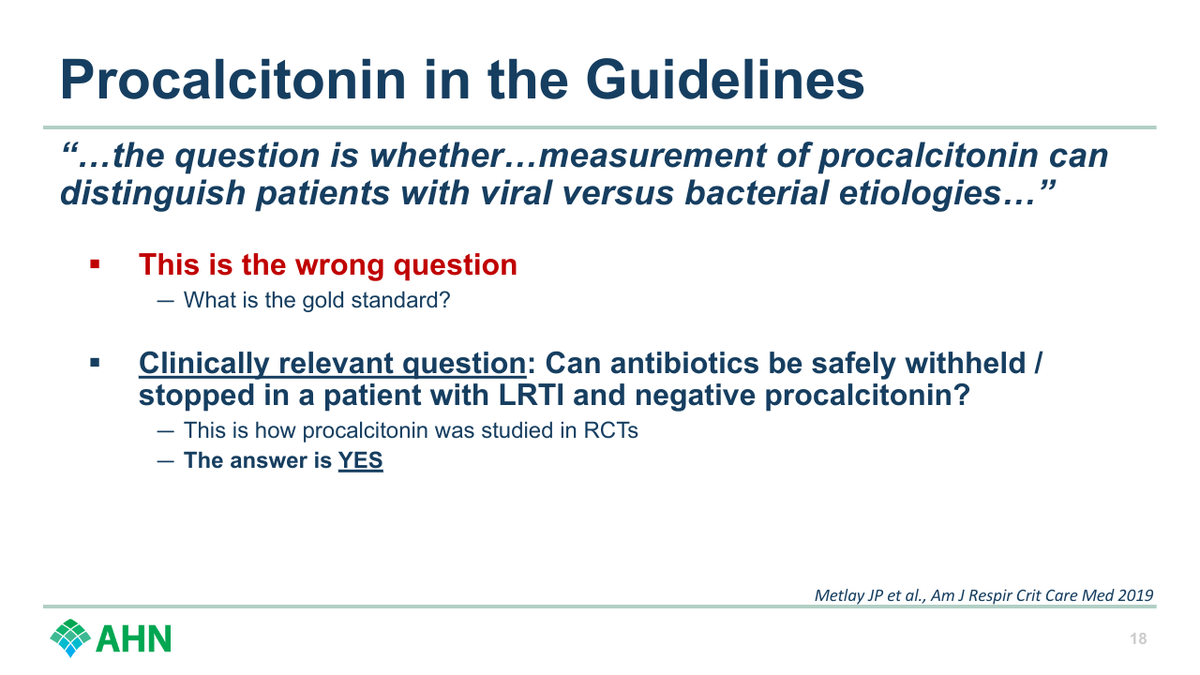
Why do guidelines get PCT wrong?
They ask the wrong question. And cite sensitivity/specificity studies - can't get that with no gold standard.
Not really about bacterial vs viral. It's "is it safe to hold abx if negative PCT?" RCTs say yes.
#SHEASpring2024
9/
They ask the wrong question. And cite sensitivity/specificity studies - can't get that with no gold standard.
Not really about bacterial vs viral. It's "is it safe to hold abx if negative PCT?" RCTs say yes.
#SHEASpring2024
9/
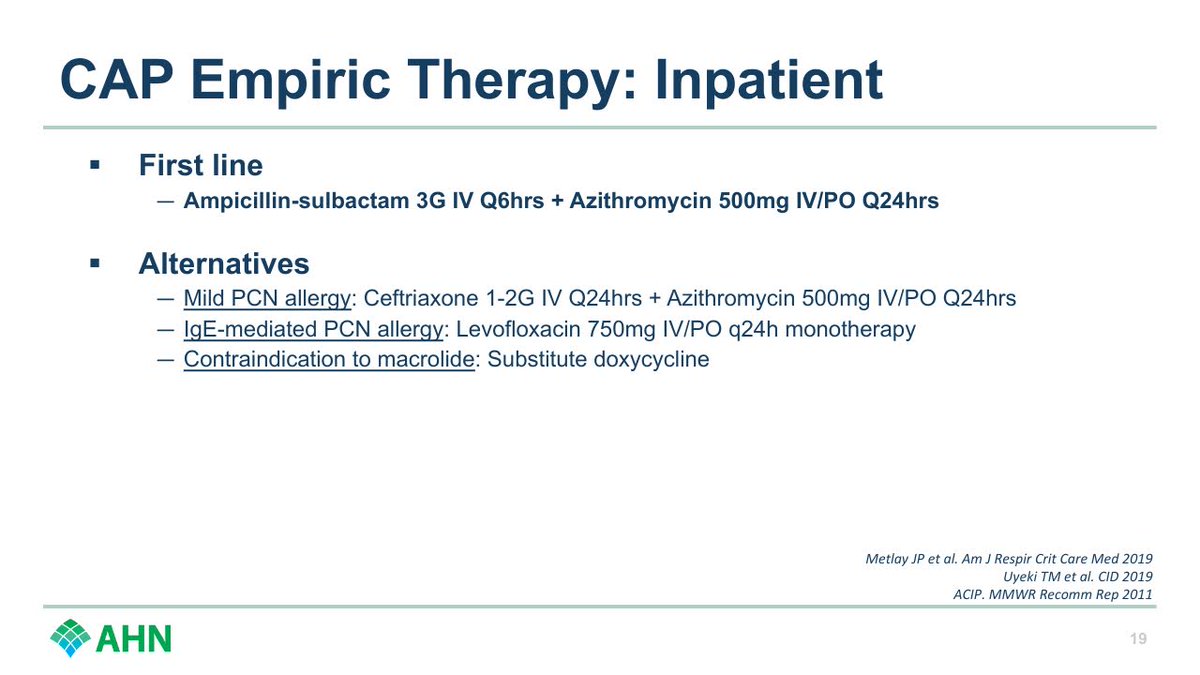
Alright, how about treatment?
Amp-sulbactam first line for us.
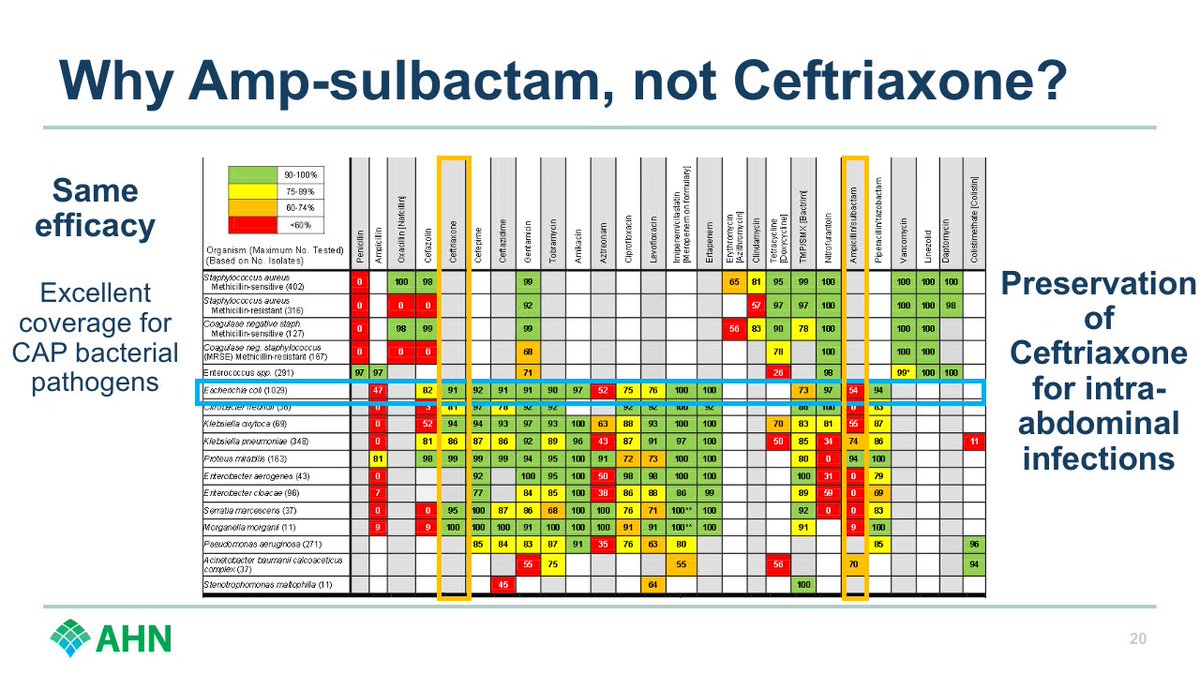
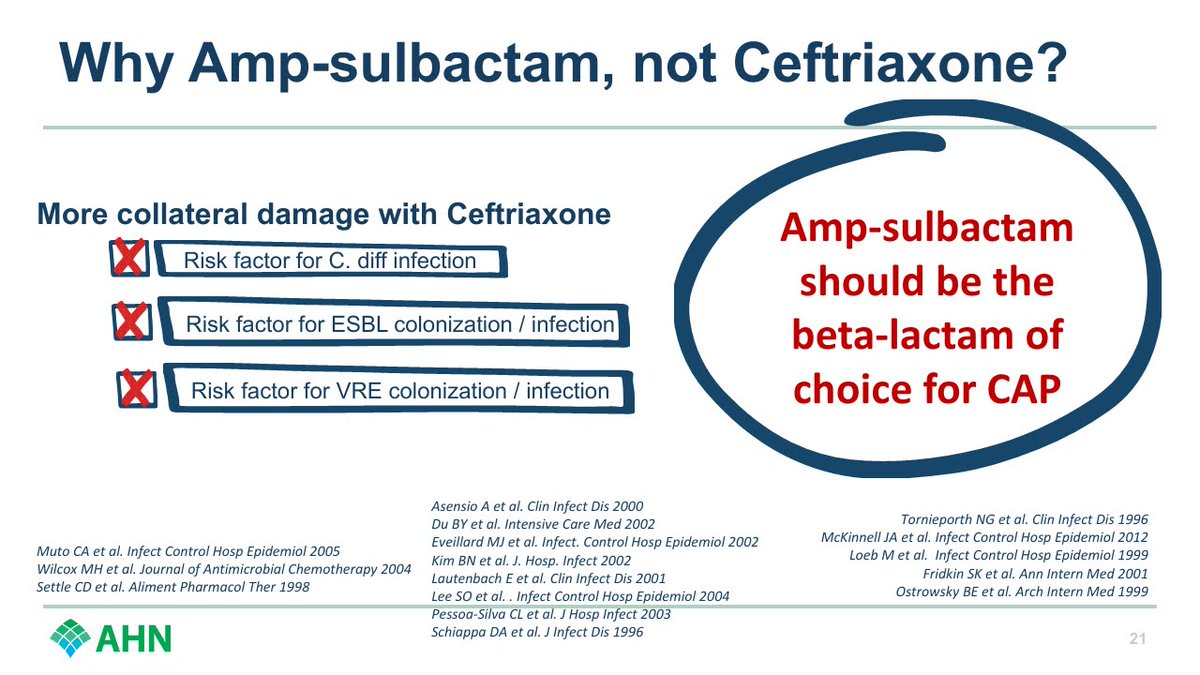
Why not Ceftriaxone?
Need Ceftriaxone for intra-ab infxns - when narrower spectrum, less ESBL/VRE selecting, and less C diff causing Amp-sulbactam works just as well for PNA bugs, use that.
#SHEASpring2024
10/
Amp-sulbactam first line for us.
Why not Ceftriaxone?
Need Ceftriaxone for intra-ab infxns - when narrower spectrum, less ESBL/VRE selecting, and less C diff causing Amp-sulbactam works just as well for PNA bugs, use that.
#SHEASpring2024
10/
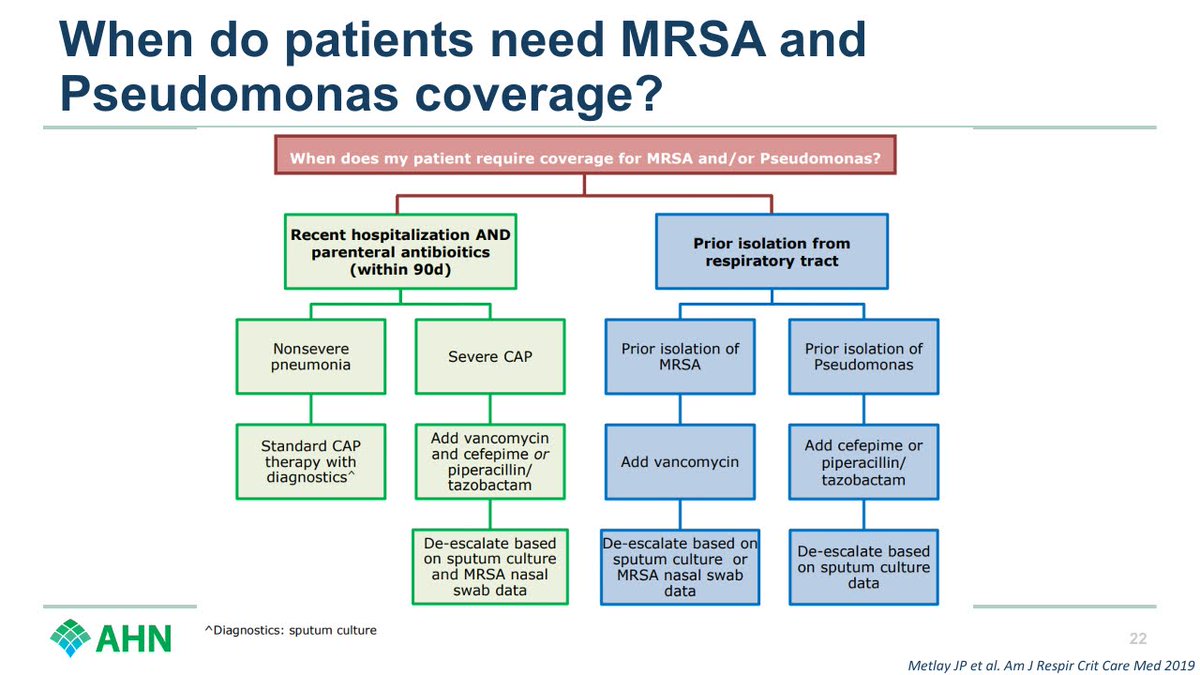
When do we need to cover MRSA / Pseudomonas?
✅If isolated previously.
✅If recent admission and IV antibiotics AND severe PNA.
That's the list.
If you trained before 2019, forget the HCAP stuff you used to know.
#SHEASpring2024
11/
✅If isolated previously.
✅If recent admission and IV antibiotics AND severe PNA.
That's the list.
If you trained before 2019, forget the HCAP stuff you used to know.
#SHEASpring2024
11/
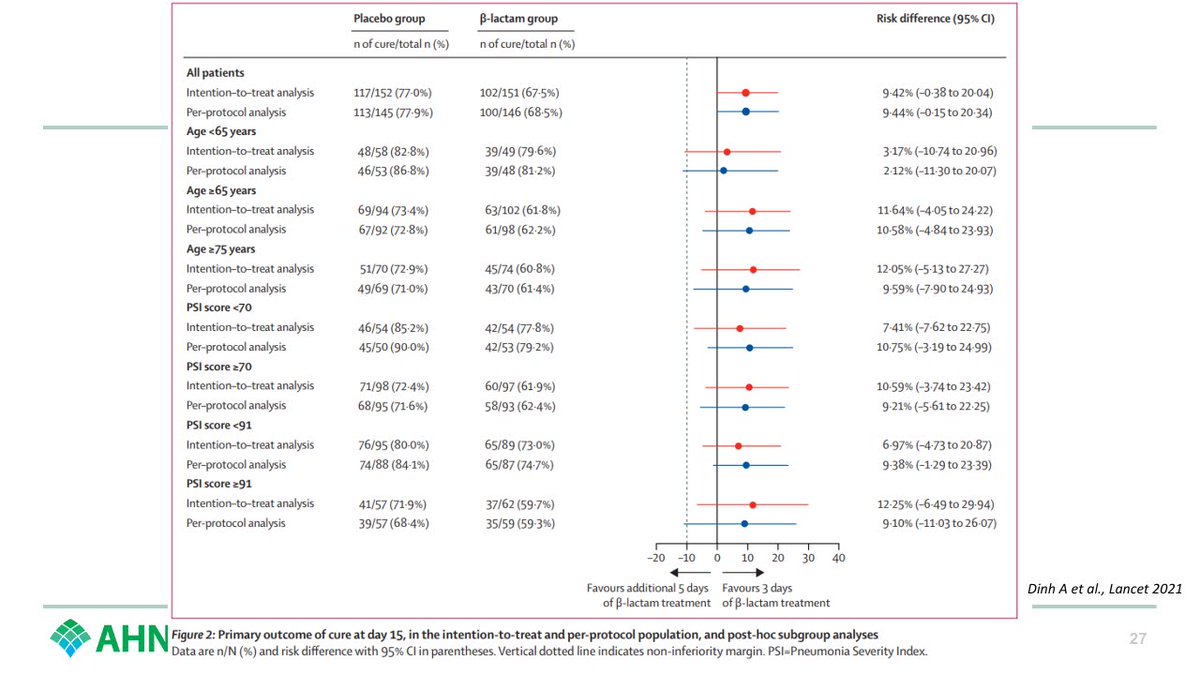
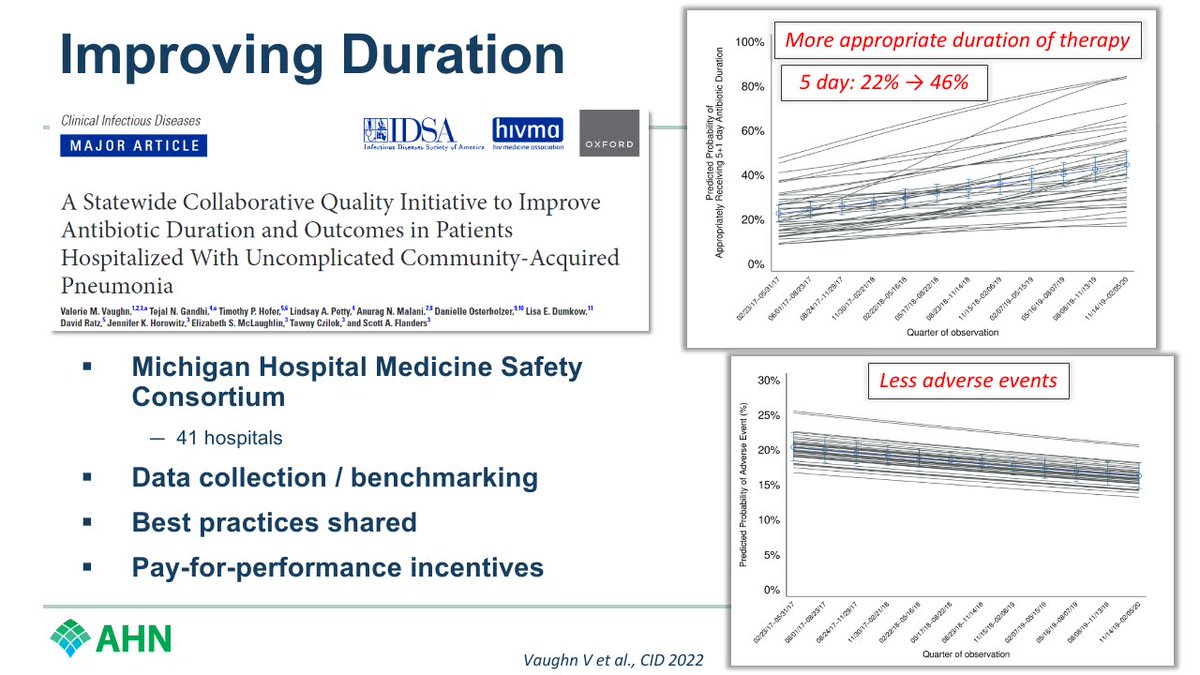
Duration of therapy?
5 days.
(As long as clinically stable by 48-72 hours).
RCT proving the guideline rec highlighted below.
#SHEASpring2024
12/
5 days.
(As long as clinically stable by 48-72 hours).
RCT proving the guideline rec highlighted below.
#SHEASpring2024
12/


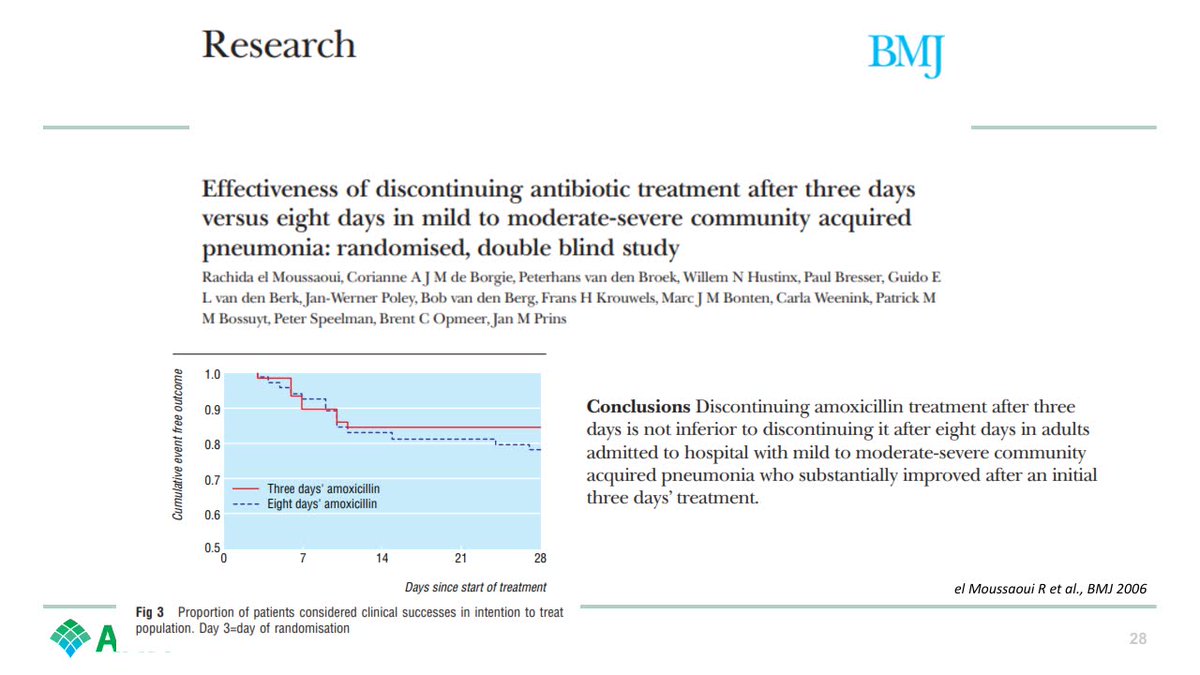
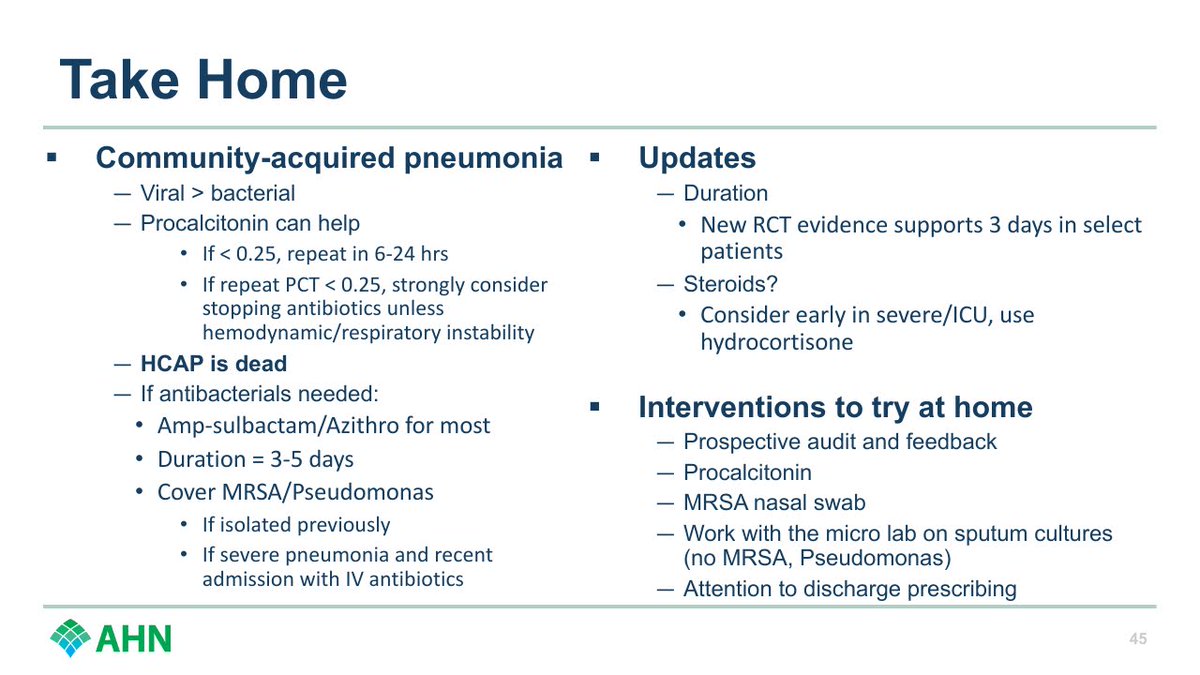
But can we go even shorter?
We probably can. New 2022 RCT suggests 3 days is fine for admitted, non-ICU patients that meet the clinical stability criteria.
A prior smaller RCT showed the same thing.
#ShorterIsBetter @BradSpellberg
#SHEASpring2024
13/
We probably can. New 2022 RCT suggests 3 days is fine for admitted, non-ICU patients that meet the clinical stability criteria.
A prior smaller RCT showed the same thing.
#ShorterIsBetter @BradSpellberg
#SHEASpring2024
13/

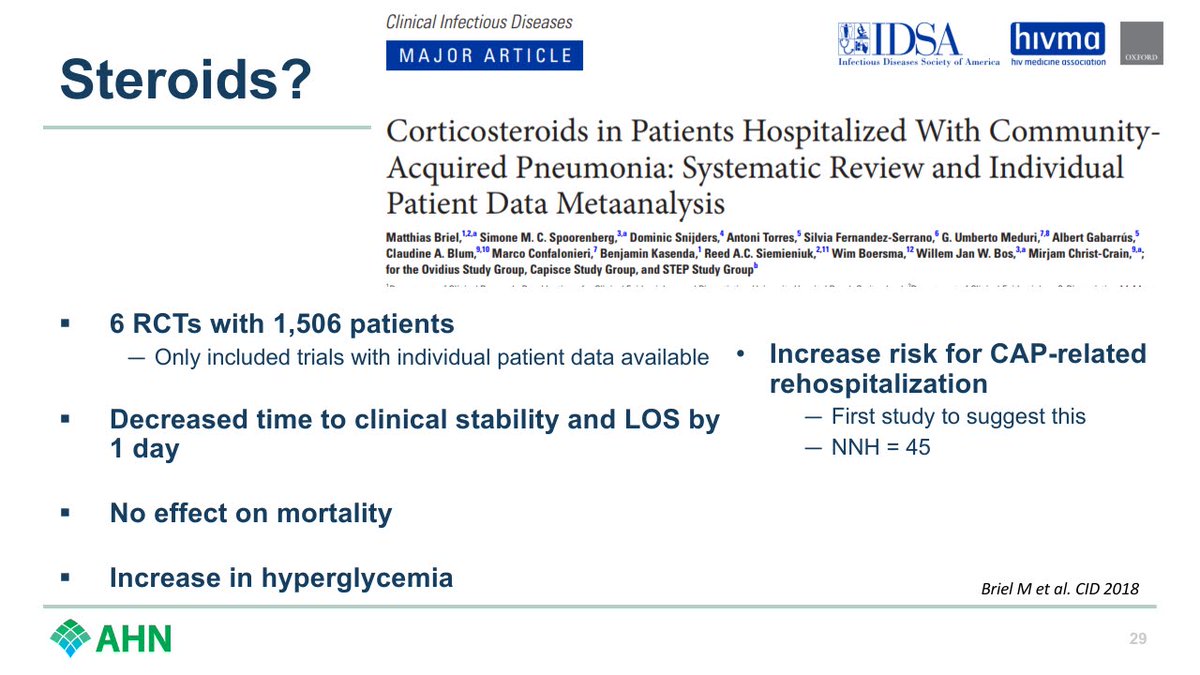
How about steroids?
Literature interesting to follow here.
Recent meta-analysis:
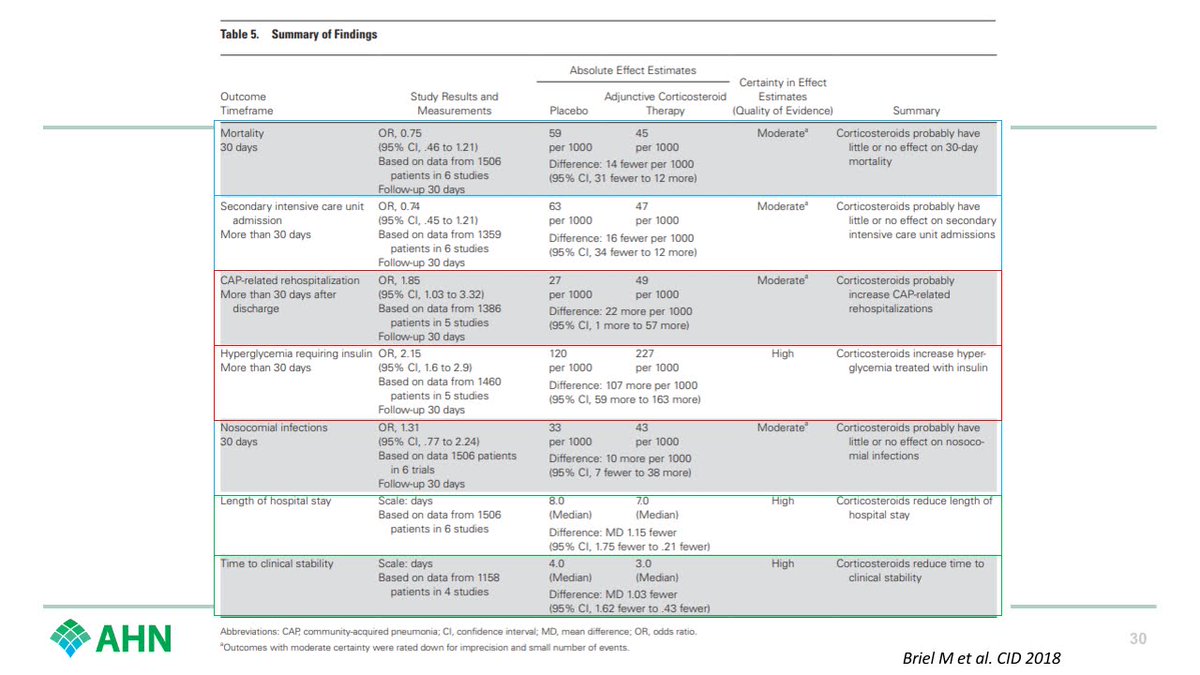
Good:
➡️Shorter LOS, faster time to stability
Bad:
➡️More hyperglycemia, more CAP-related rehosp.
Neutral:
➡️No diff in mortality, ICU admission, nosocomial infection
#SHEASpring2024
14/
Literature interesting to follow here.
Recent meta-analysis:
Good:
➡️Shorter LOS, faster time to stability
Bad:
➡️More hyperglycemia, more CAP-related rehosp.
Neutral:
➡️No diff in mortality, ICU admission, nosocomial infection
#SHEASpring2024
14/
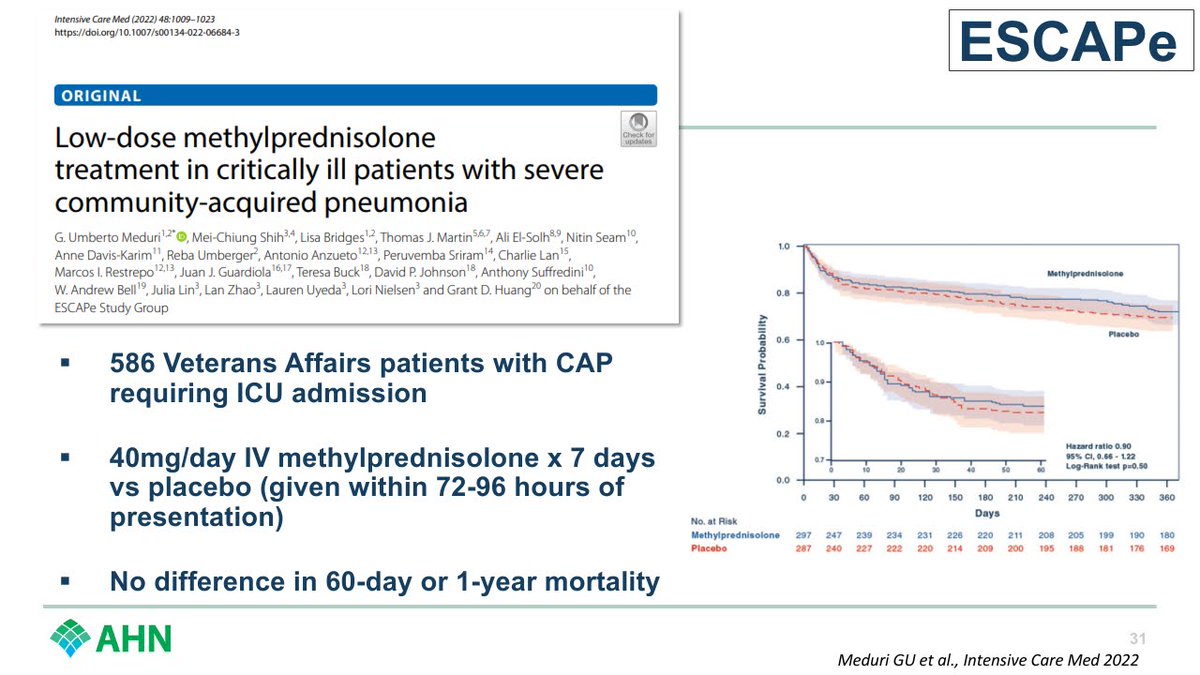
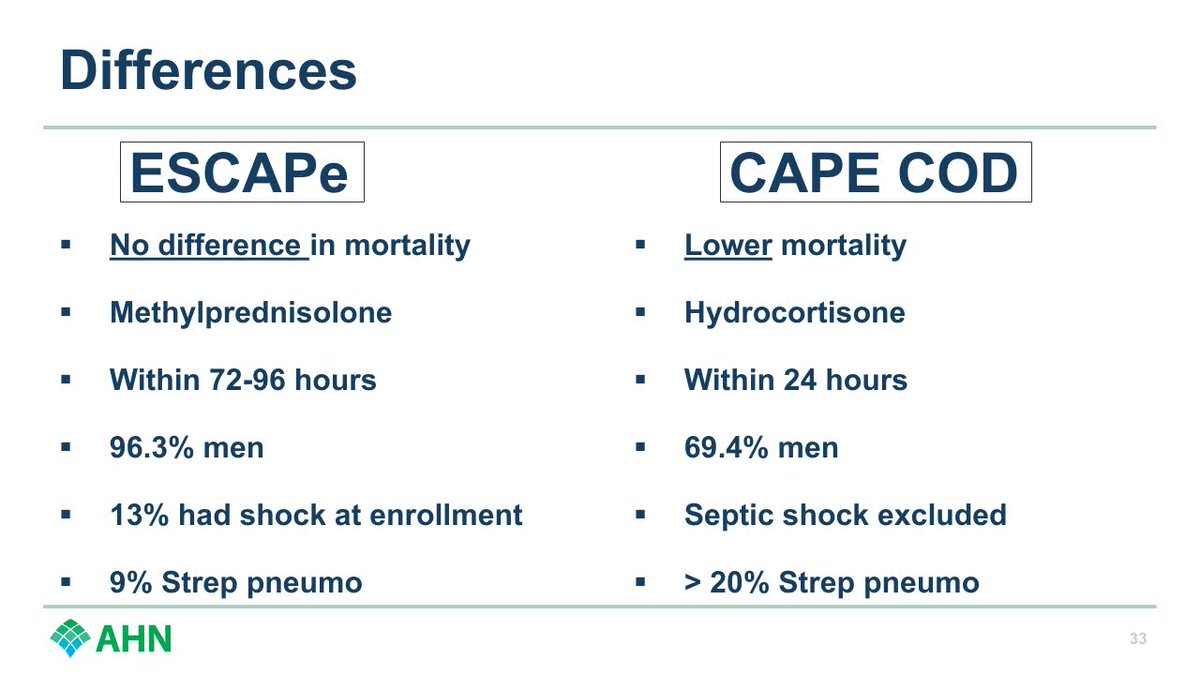
Very recently, a couple trials in severe CAP requiring ICU with conflicting results.
ESCAPe = no benefit
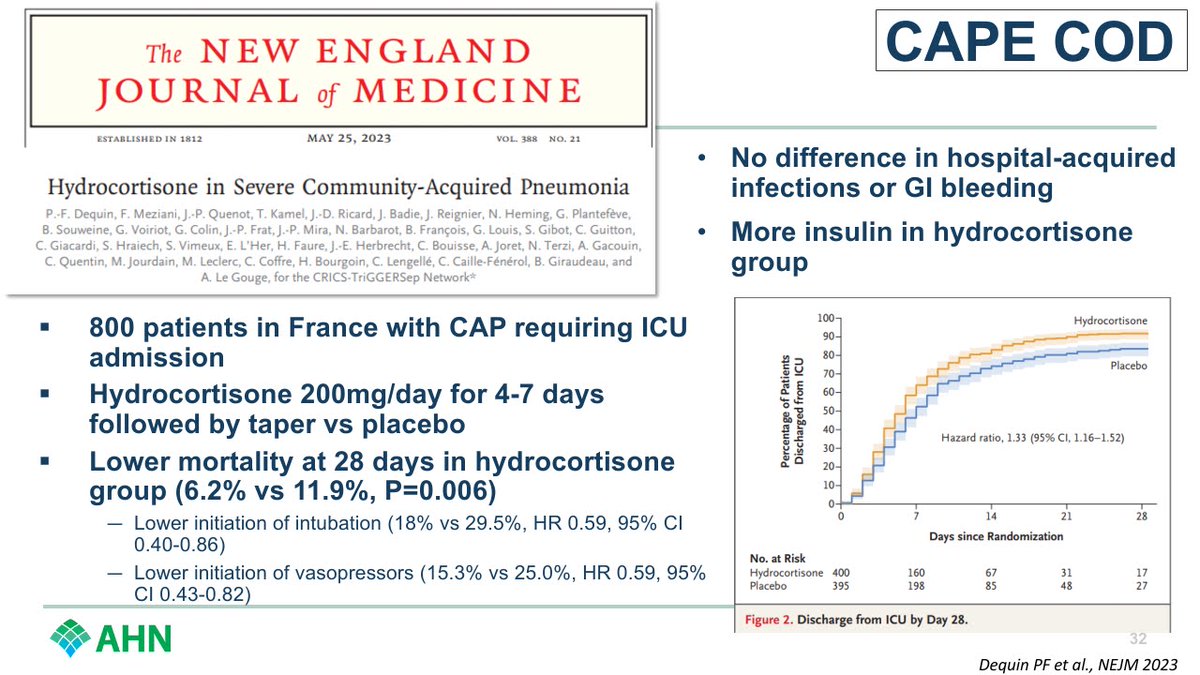
CAPE COD = Mortality benefit with NNT < 20
Why conflicting?
Choice of steroid might matter. Early might matter. Pathogen might matter.
#SHEASpring2024
15/
ESCAPe = no benefit
CAPE COD = Mortality benefit with NNT < 20
Why conflicting?
Choice of steroid might matter. Early might matter. Pathogen might matter.
#SHEASpring2024
15/
So where do I come down on steroids in 2024?
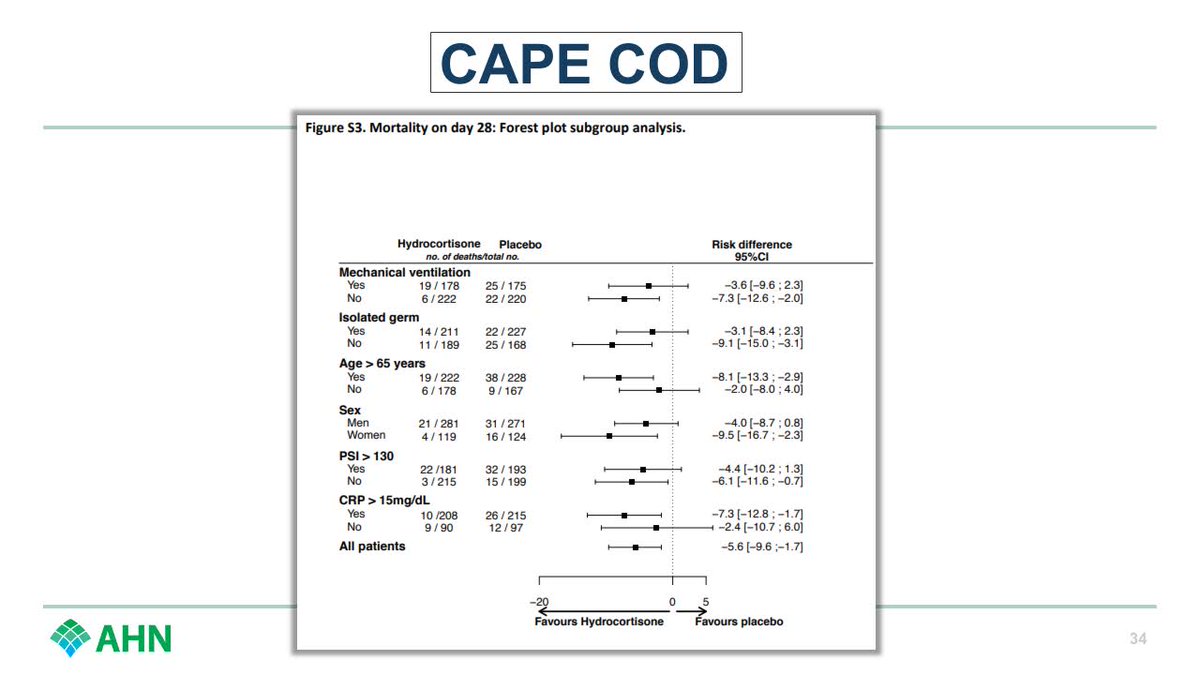
More likely to come in the literature, but for now, I'd consider it early in patients who need ICU who are not in shock, and I'd use hydrocortisone.
High CRP/older/female might push you a bit more.
#SHEASpring2024
16/
More likely to come in the literature, but for now, I'd consider it early in patients who need ICU who are not in shock, and I'd use hydrocortisone.
High CRP/older/female might push you a bit more.
#SHEASpring2024
16/
Let's close out with some things your stewardship program can do to improve care in pneumonia.
#SHEASpring2024
17/
#SHEASpring2024
17/
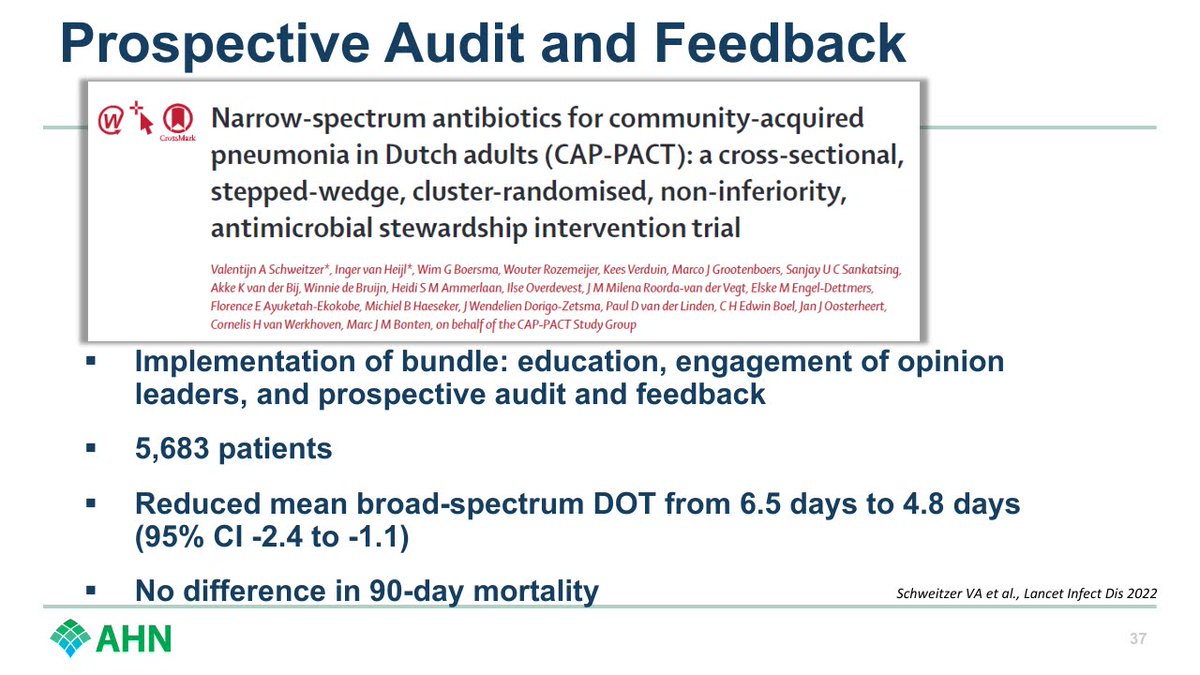
Prospective audit and feedback.
Most of us do this every day, but it works!
Consider disease-state focused reviews to catch all of the CAP patients, even if already on narrower therapy.
#SHEASpring2024
18/
Most of us do this every day, but it works!
Consider disease-state focused reviews to catch all of the CAP patients, even if already on narrower therapy.
#SHEASpring2024
18/
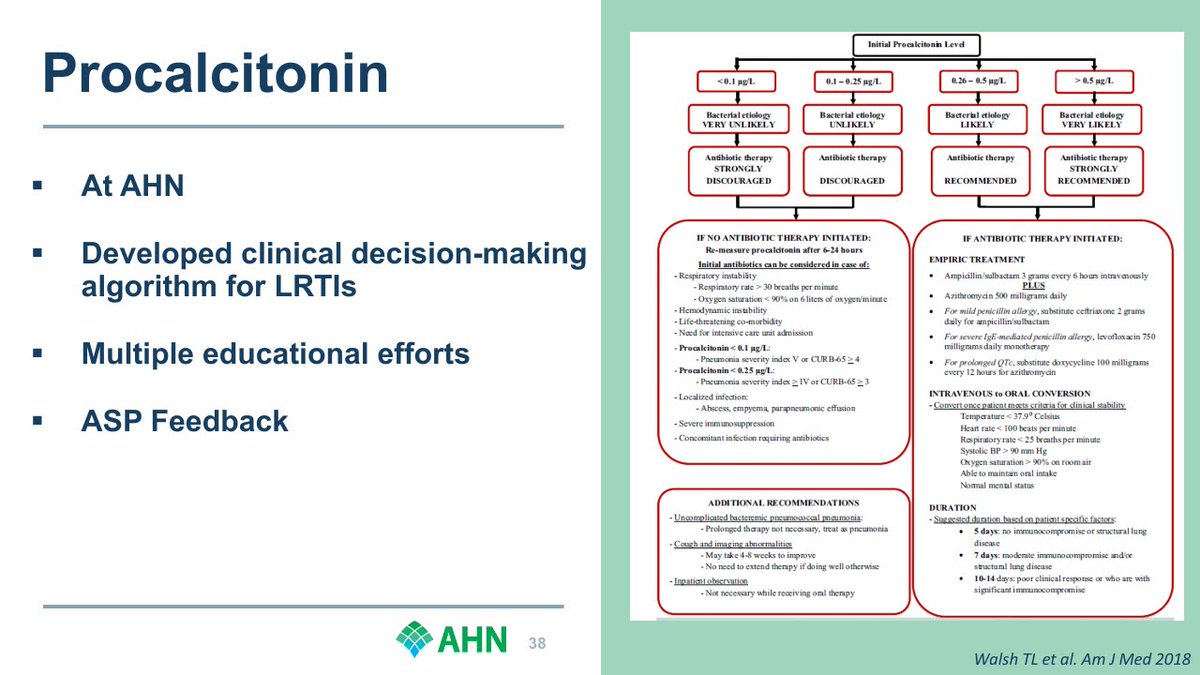
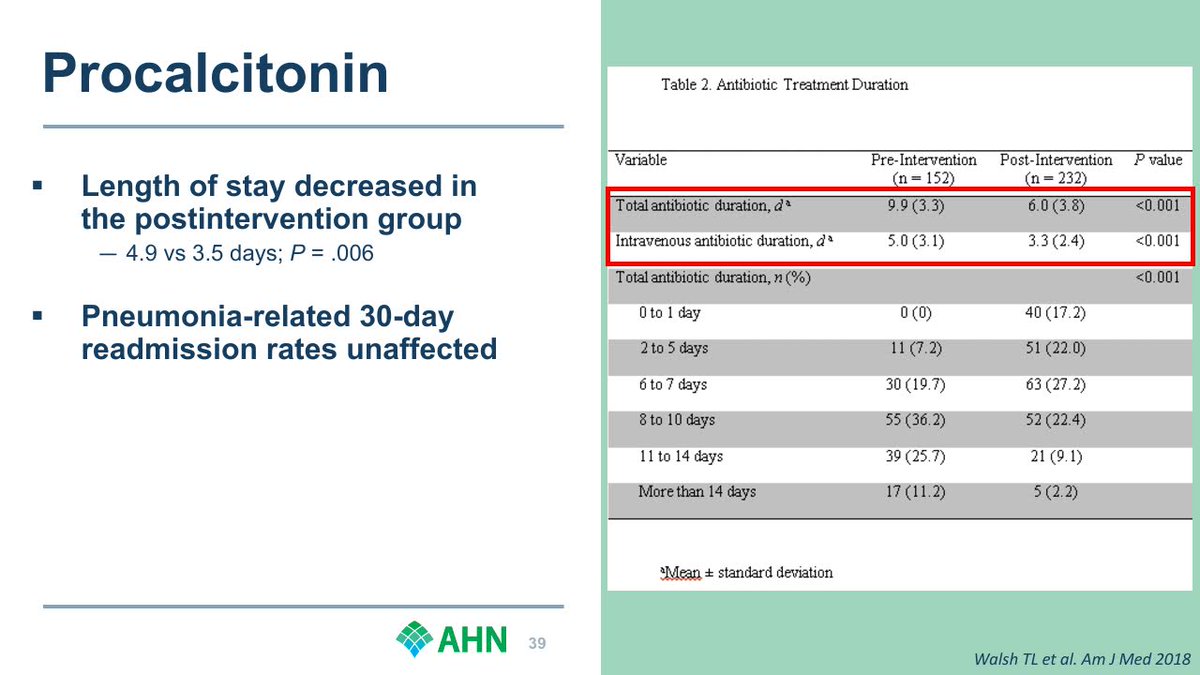
Procalcitonin.
Here is some real world data from our group at AHN. Less antibiotics, shorter LOS, no change in readmissions.
@TomWalshMD13 @matthewmof31 @dnbrems @DustinRCarr @cbuchananpharm @CessnaPharmD
#SHEASpring2024
19/
Here is some real world data from our group at AHN. Less antibiotics, shorter LOS, no change in readmissions.
@TomWalshMD13 @matthewmof31 @dnbrems @DustinRCarr @cbuchananpharm @CessnaPharmD
#SHEASpring2024
19/
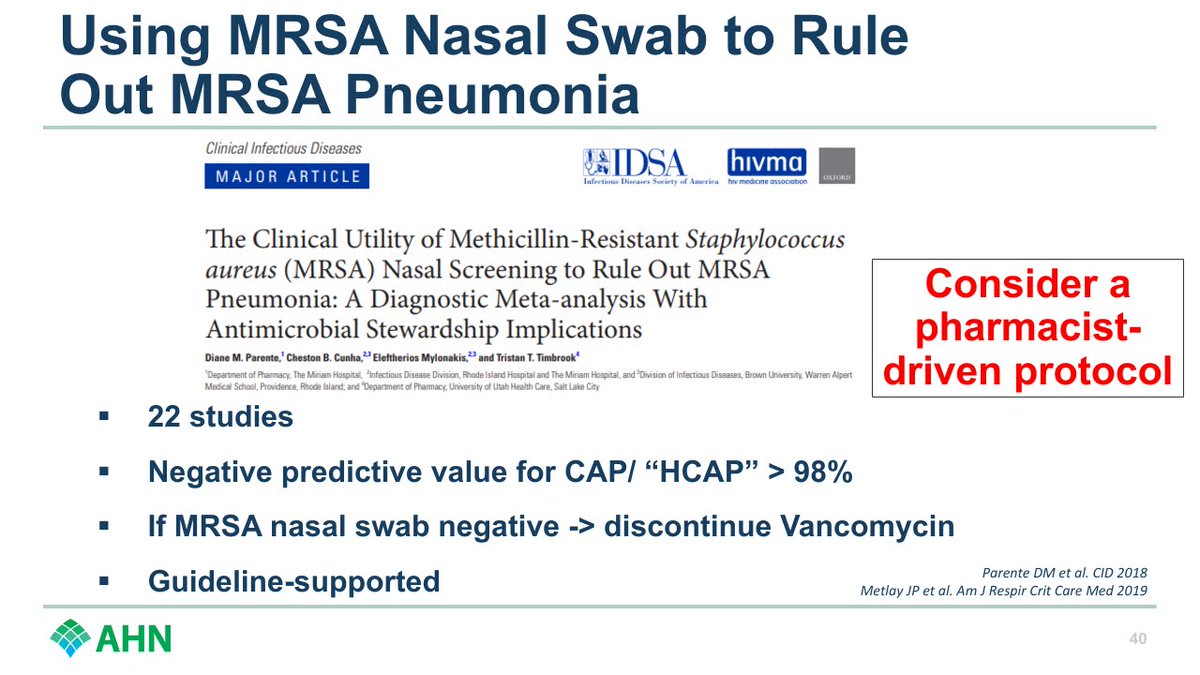
MRSA nasal swab.
Excellent NPV to exclude MRSA pneumonia.
We have a pharmacy-driven protocol - if Vanc ordered for PNA, our pharmacists can order the swab. When comes back negative, our ASP team reaches out with rec to stop.
#SHEASpring2024
20/
Excellent NPV to exclude MRSA pneumonia.
We have a pharmacy-driven protocol - if Vanc ordered for PNA, our pharmacists can order the swab. When comes back negative, our ASP team reaches out with rec to stop.
#SHEASpring2024
20/
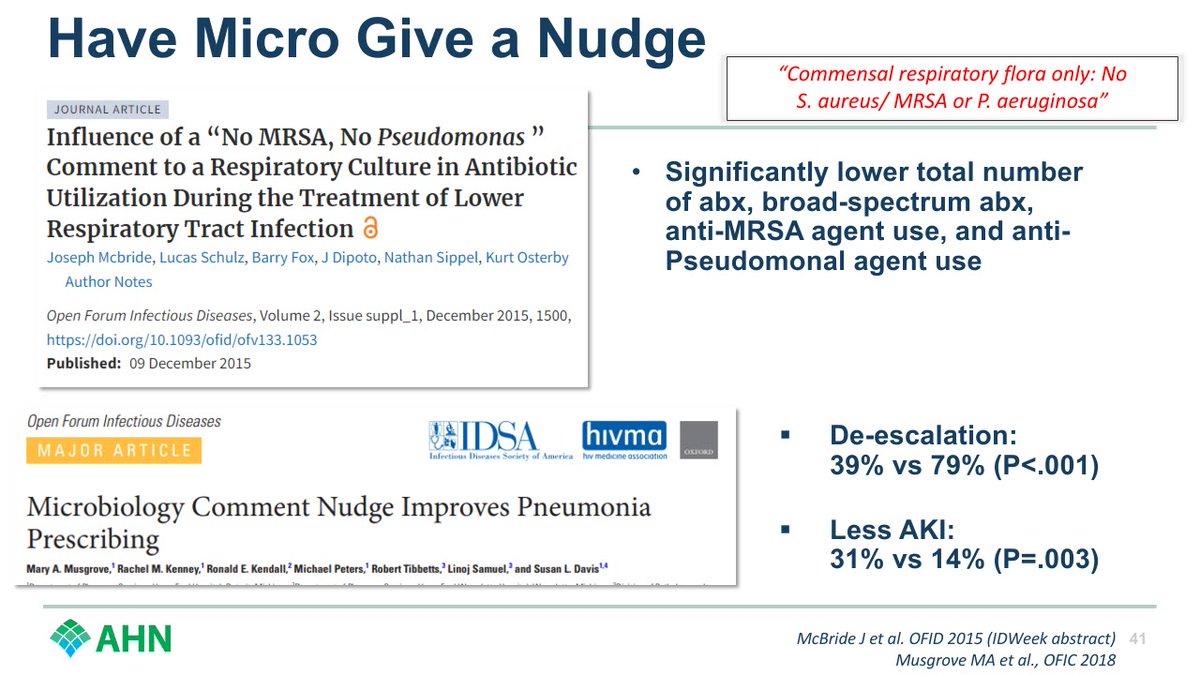
Have micro give a nudge.
Instead of just saying "normal respiratory flora" on sputum cultures, add "No MRSA, No Pseudomonas"
Small change with a big impact.
#SHEASpring2024
21/
Instead of just saying "normal respiratory flora" on sputum cultures, add "No MRSA, No Pseudomonas"
Small change with a big impact.
#SHEASpring2024
21/
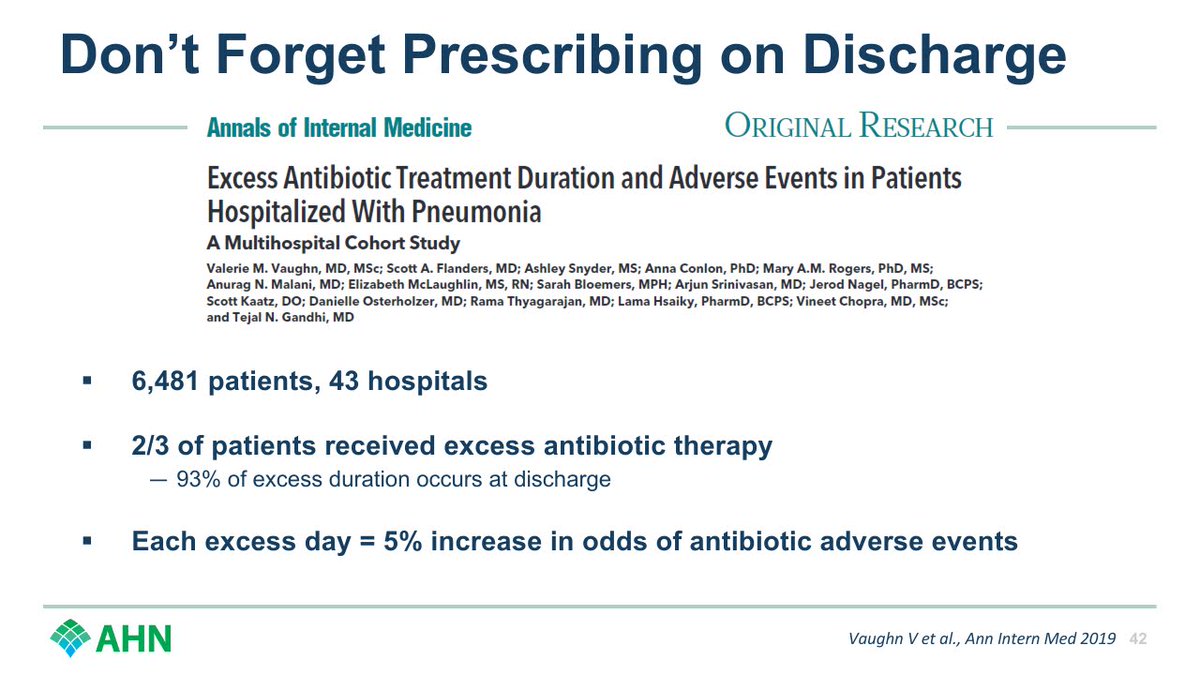
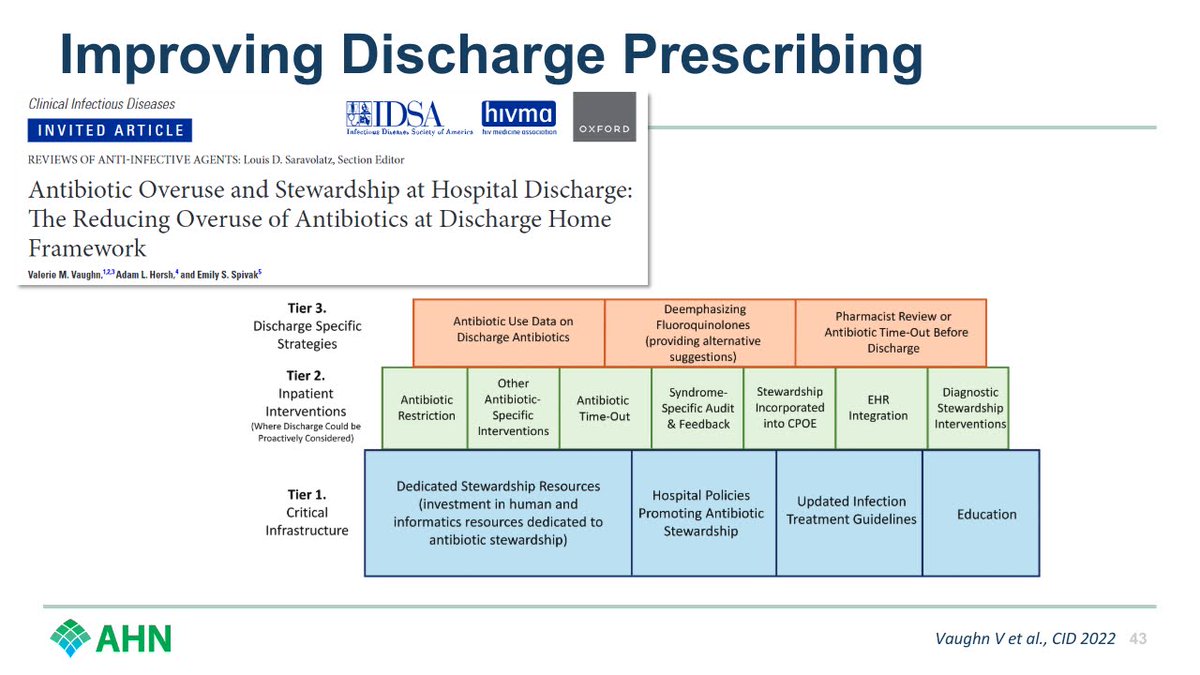
And don't forget discharge prescribing.
Most excess duration happens at discharge, and each excess day matters.
Try to impact it however you can.
Great work on this here from @ValerieVaughnMD.
#SHEASpring2024
22/
Most excess duration happens at discharge, and each excess day matters.
Try to impact it however you can.
Great work on this here from @ValerieVaughnMD.
#SHEASpring2024
22/
Loading suggestions...