

1/
Have you ever been confused by prostatitis?
When to suspect it? How to diagnose it? How to treat it? Is it acute or chronic?
Read on for more information!
@sargsyanz @EvaAmenta @RizwanSohailMD @MelanieGoebelMD
Have you ever been confused by prostatitis?
When to suspect it? How to diagnose it? How to treat it? Is it acute or chronic?
Read on for more information!
@sargsyanz @EvaAmenta @RizwanSohailMD @MelanieGoebelMD
2/
Our comprehensive review of prostatitis is available here! 👇👇👇
pubmed.ncbi.nlm.nih.gov
It was a pleasure to work with @BCMIDFellowship fellow Tyler Brehm and @bwtrautner on this review!
Our comprehensive review of prostatitis is available here! 👇👇👇
pubmed.ncbi.nlm.nih.gov
It was a pleasure to work with @BCMIDFellowship fellow Tyler Brehm and @bwtrautner on this review!

3/
Risk factors for prostatitis:
Anatomical abnormalities
Diabetes
Urogenital instrumentation
Immunosuppression
Acute and chronic bacterial prostatitis are different clinical entities!
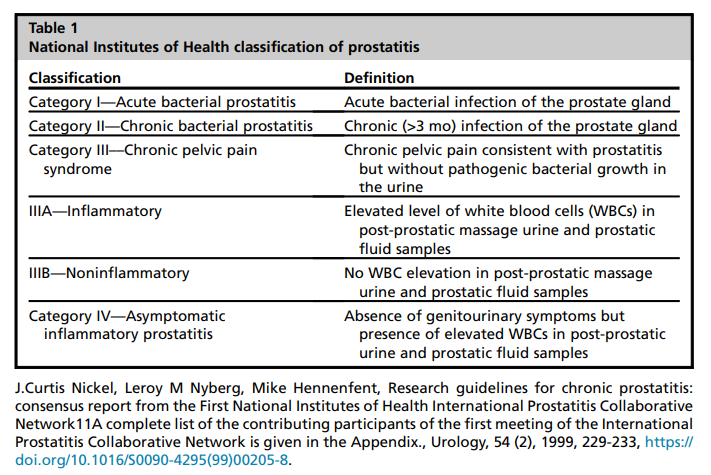
Classification of prostatitis:
Risk factors for prostatitis:
Anatomical abnormalities
Diabetes
Urogenital instrumentation
Immunosuppression
Acute and chronic bacterial prostatitis are different clinical entities!
Classification of prostatitis:
4/
When to suspect acute bacterial prostatitis (ABP)?
When to suspect acute bacterial prostatitis (ABP)?

5/ Symptoms of ABP:

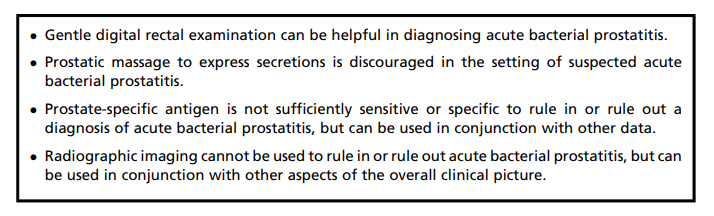
6/ Can DRE be performed??
👇👇👇
👇👇👇

7/ Summary of ABP diagnostic points:
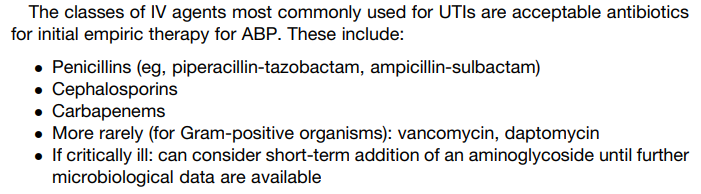
8/ Treatment of acute bacterial prostatitis:
9/ For step-down to oral antibiotics once the patient is clinically stabilized:

10/ How long should acute bacterial prostatitis be treated?? 👇👇👇

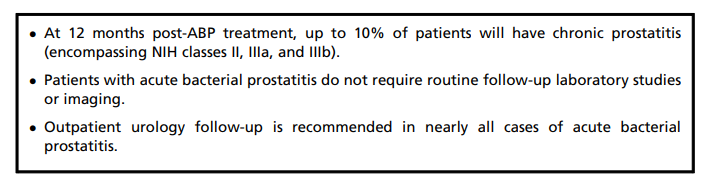
11/ What is the outcome of patients with acute bacterial prostatitis??
12/ Switching gears to chronic bacterial prostatitis (a different clinical entity)!!
When should chronic bacterial prostatitis (CBP) be suspected?
When should chronic bacterial prostatitis (CBP) be suspected?
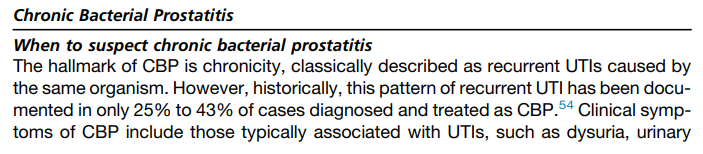
13/ Most importantly, chronic bacterial prostatitis has a different clinical presentation than acute bacterial prostatitis!

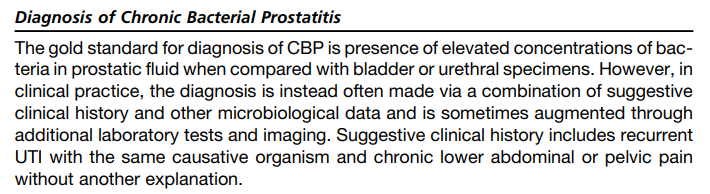
14/ How to diagnose chronic bacterial prostatitis??
15/ Best options for treatment of chronic bacterial prostatitis??
Fluoroquinolones for 4-6 weeks
Trimethoprim-sulfamethoxazole for 6 weeks
Could *consider*:
Tetracyclines (doxycycline or minocycline)
Fosfomycin
Fluoroquinolones for 4-6 weeks
Trimethoprim-sulfamethoxazole for 6 weeks
Could *consider*:
Tetracyclines (doxycycline or minocycline)
Fosfomycin
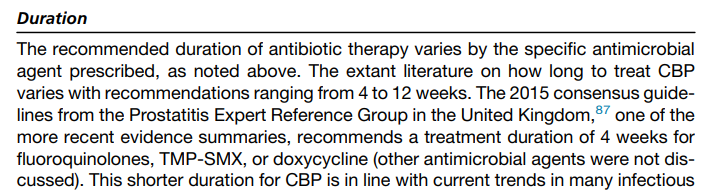
16/ How long should chronic bacterial prostatitis be treated?
17/ What is the natural history of chronic bacterial prostatitis??
18/ Are any other non-antibiotic medications useful in chronic bacterial prostatitis?
In general, no good supportive data.
In general, no good supportive data.
19/ Summary!
- Acute and chronic bacterial prostatitis are different entities.
- Suspect ABP with sepsis of suspected urinary source and no evidence of pyelo or another urinary focus.
- ABP can be Dx'ed by clinical presentation and gentle DRE. Elevated PSA can support the Dx.
- Acute and chronic bacterial prostatitis are different entities.
- Suspect ABP with sepsis of suspected urinary source and no evidence of pyelo or another urinary focus.
- ABP can be Dx'ed by clinical presentation and gentle DRE. Elevated PSA can support the Dx.
20/ Summary! (continued)
- ABP is treated with 2-4 weeks of Abx!
- CBP is indolent and should be suspected when a patient has recurrent UTIs due to the same organism.
- Fluoroquinolones and TMP/SMX are best options for susceptible organisms with Rx of 4-6 weeks!
/End
- ABP is treated with 2-4 weeks of Abx!
- CBP is indolent and should be suspected when a patient has recurrent UTIs due to the same organism.
- Fluoroquinolones and TMP/SMX are best options for susceptible organisms with Rx of 4-6 weeks!
/End
Loading suggestions...