

1/8
A young man comes to our clinic for evaluation of rapid weight gain. He has heard "diet and exercise" several times before he sees us.
The driver license photo was taken ~9 months prior.
We make some observations, leading us to generate a hypothesis.
A young man comes to our clinic for evaluation of rapid weight gain. He has heard "diet and exercise" several times before he sees us.
The driver license photo was taken ~9 months prior.
We make some observations, leading us to generate a hypothesis.

2/8
Based on our hypothesis, we examine the patient further. And we make several more important observations, increasing the likelihood of our hypothesis.
Based on our hypothesis, we examine the patient further. And we make several more important observations, increasing the likelihood of our hypothesis.



3/8
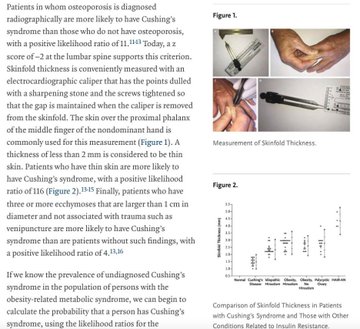
We remember that skin thickness can be an important sign in this condition, from Lynn Loriaux's 2017
@NEJM review.
(Examiner's hand is shown above, patient's below.)
We remember that skin thickness can be an important sign in this condition, from Lynn Loriaux's 2017
@NEJM review.
(Examiner's hand is shown above, patient's below.)

4/8
We now have a clinical syndrome that is consistent with Cushing's syndrome.
A confirmatory test is our next step.
Urine free cortisol (confirmatory test): 7,960 mcg/24H (!)
We now have a clinical syndrome that is consistent with Cushing's syndrome.
A confirmatory test is our next step.
Urine free cortisol (confirmatory test): 7,960 mcg/24H (!)
5/8
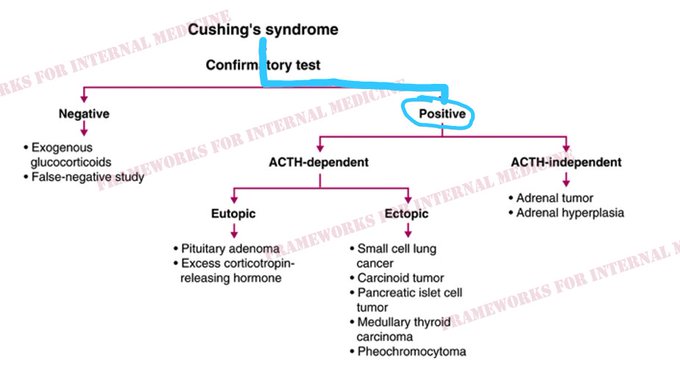
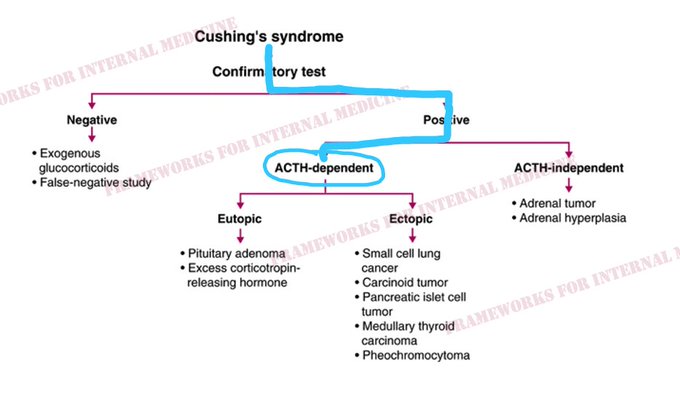
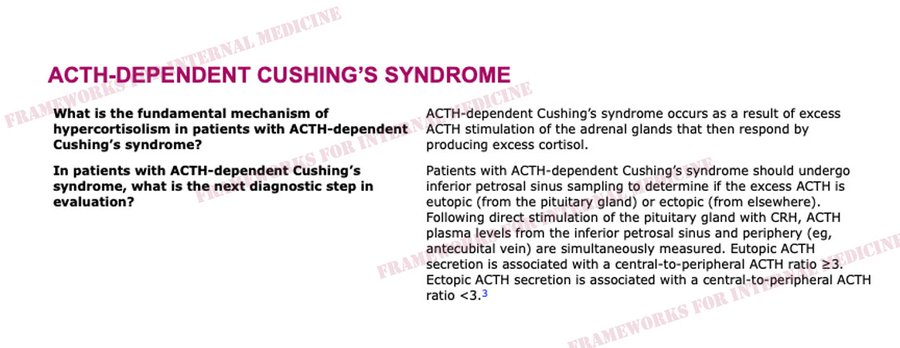
We have now confirmed the diagnosis of Cushing's syndrome. The next question is, is it ACTH-dependent or ACTH-independent?
A plasma ACTH level is necessary to make this determination.
Plasma ACTH level is 496 pg/mL (normal <50).
We have now confirmed the diagnosis of Cushing's syndrome. The next question is, is it ACTH-dependent or ACTH-independent?
A plasma ACTH level is necessary to make this determination.
Plasma ACTH level is 496 pg/mL (normal <50).
6/8
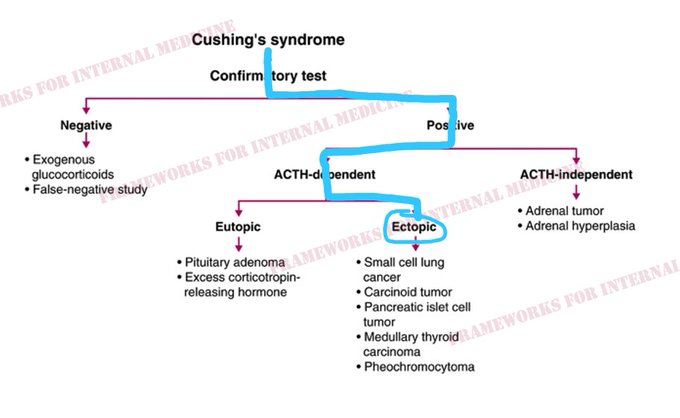
Where is that ACTH coming from? The pituitary gland (ectopic) or elsewhere (ectopic)?
To determine this, inferior petrosal sinus sampling is necessary.
IPSS shows a ratio <3, confirming an ectopic source of ACTH.
Where is that ACTH coming from? The pituitary gland (ectopic) or elsewhere (ectopic)?
To determine this, inferior petrosal sinus sampling is necessary.
IPSS shows a ratio <3, confirming an ectopic source of ACTH.
7/8
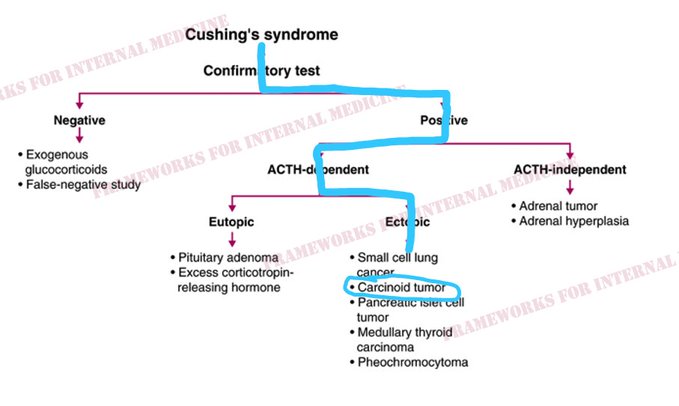
Chest imaging ultimately reveals the presence of a bronchial carcinoid tumor.
Chest imaging ultimately reveals the presence of a bronchial carcinoid tumor.
8/8
We have diagnosed ACTH-dependent Cushing's syndrome from an ectopic source using only our eyes and hypothesis-driven laboratory and imaging tests.
For more frameworks: amazon.com
We have diagnosed ACTH-dependent Cushing's syndrome from an ectopic source using only our eyes and hypothesis-driven laboratory and imaging tests.
For more frameworks: amazon.com

Loading suggestions...