

This generated some great discussion. Now let's do a deep dive
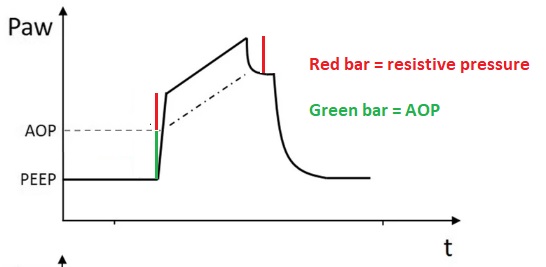
The first odd thing here is the Paw waveform. Traditional teaching is that in VC with continuous flow, the initial ⬆️in Paw corresponds to the pressure required to overcome resistance (as lung filling is minimal)
1/
The first odd thing here is the Paw waveform. Traditional teaching is that in VC with continuous flow, the initial ⬆️in Paw corresponds to the pressure required to overcome resistance (as lung filling is minimal)
1/
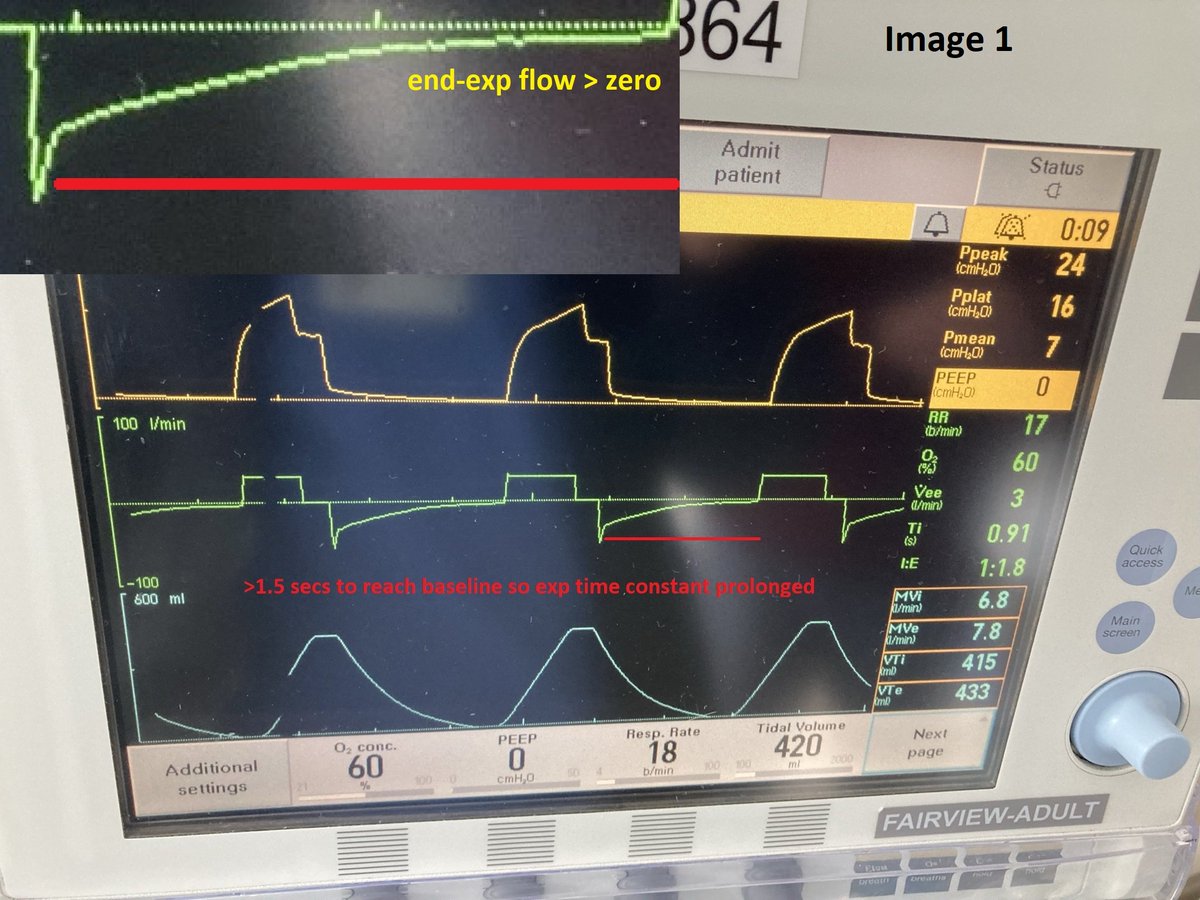
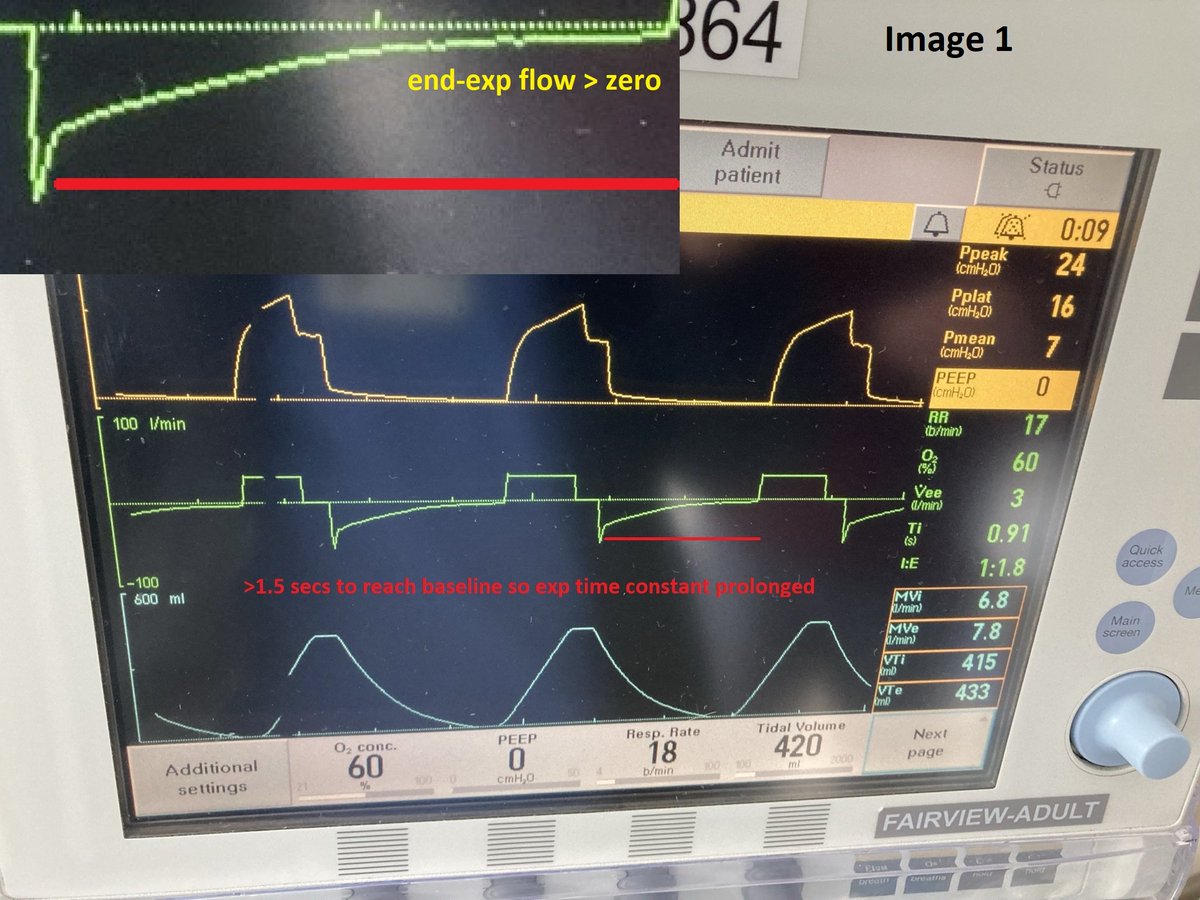
Since flow is constant, this 'resistive pressure' remains constant throughout the breath as revealed by the post-inspiratory pause (image 1)
Hence, the height of the initial Paw spike should equal the height of PIP - Pplat. This is not the case in our patient!
2/
Hence, the height of the initial Paw spike should equal the height of PIP - Pplat. This is not the case in our patient!
2/


In our patient, the initial ⬆️ in Paw is >> PIP - Pplat (let's call this pattern X). This implies that in the beginning of the breath, pressure is being spent not just to overcome the resistive load, but also on something else. But what?
Let's talk about 'airway closure'.
3/
Let's talk about 'airway closure'.
3/

Airway closure is a condition where at end-expiration, all alveoli are completely isolated form central airways.
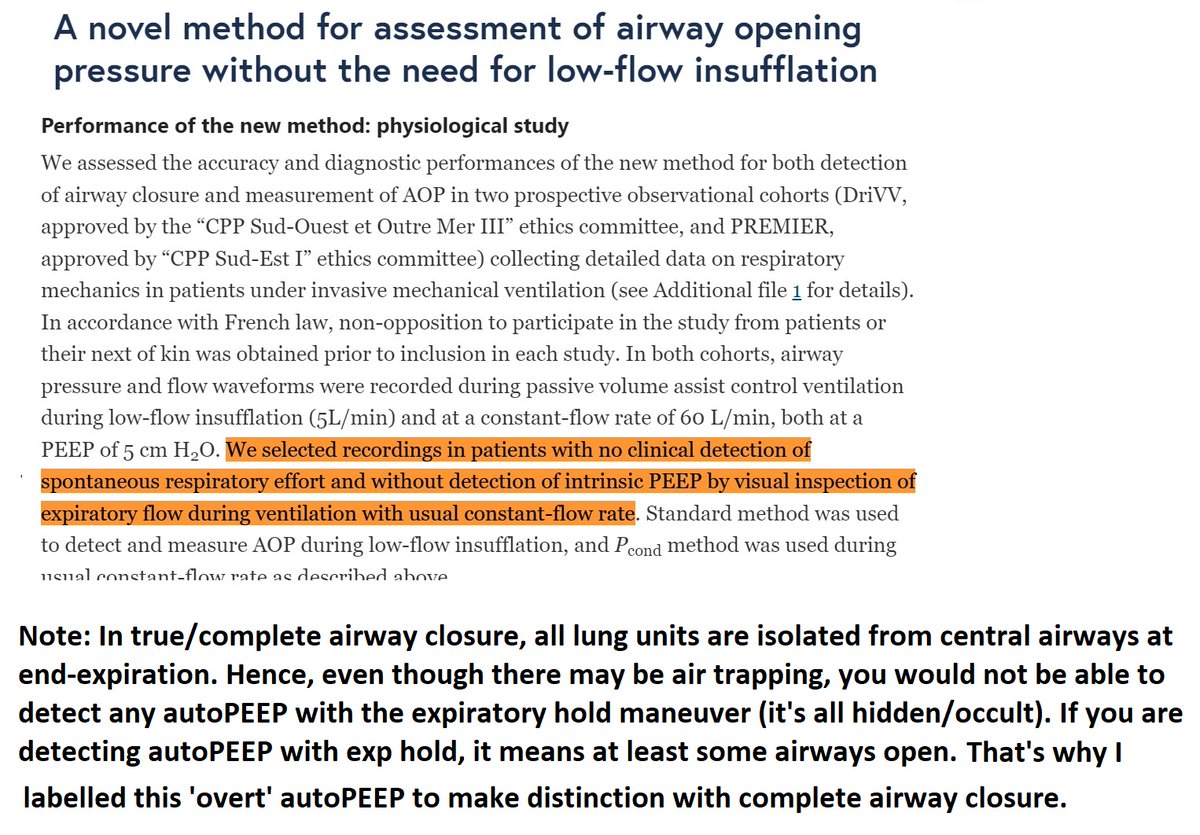
This was recently described in ARDS in this classic paper (see image 2).
The pressure required to overcome airway closure is airway opening pressure (AOP)
4/
This was recently described in ARDS in this classic paper (see image 2).
The pressure required to overcome airway closure is airway opening pressure (AOP)
4/
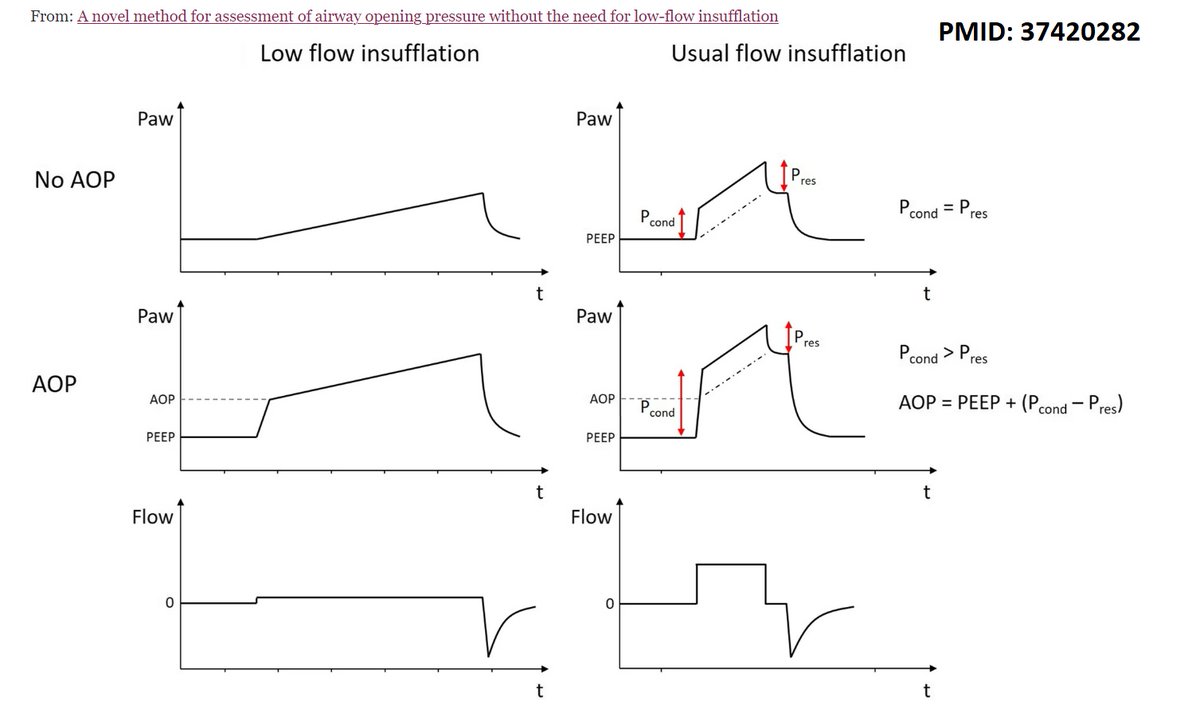
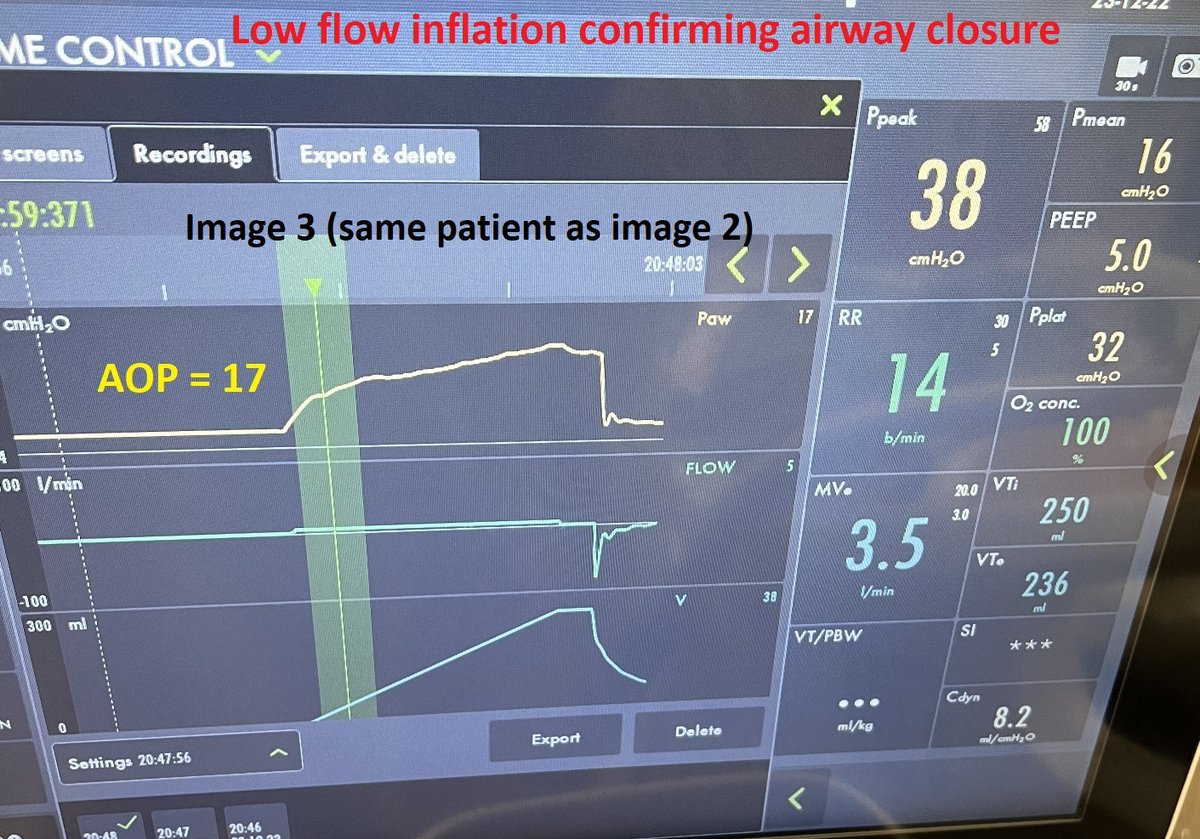
The traditional way of measuring AOP is by doing a low-flow inflation that (mostly) filters out resistive pressure
In airway closure, first few mLs will be discharged into the vent circuit that has very low compliance
Excellent demo by @respresource:
youtube.com
5/
In airway closure, first few mLs will be discharged into the vent circuit that has very low compliance
Excellent demo by @respresource:
youtube.com
5/
Now, back to VC with constant flow -
In patients with airway closure, AOP will be added to the resistive pressure during initial increase in Paw!
This has actually been studied by Haudebourg et al, who found that this method was highly accurate in detecting airway closure.
6/
In patients with airway closure, AOP will be added to the resistive pressure during initial increase in Paw!
This has actually been studied by Haudebourg et al, who found that this method was highly accurate in detecting airway closure.
6/
So did our patient have airway closure? Not quite! (at least not complete, at that instant).
Low-flow inflation done around the same time showed trivial, if any, AOP (👇)
So how do we make sense of this now? Is there another reason for this peculiar Paw pattern (pattern X)?
7/
Low-flow inflation done around the same time showed trivial, if any, AOP (👇)
So how do we make sense of this now? Is there another reason for this peculiar Paw pattern (pattern X)?
7/

Yes there is! 'Overt' auto-PEEP
Presence of auto-PEEP will similarly act as an impedance to passive inflation, thereby adding on to the resistive pressure (simulated scenario in img 1)
Of note, authors of the Haudebourg paper astutely excluded patients with autoPEEP (img 2)
8/
Presence of auto-PEEP will similarly act as an impedance to passive inflation, thereby adding on to the resistive pressure (simulated scenario in img 1)
Of note, authors of the Haudebourg paper astutely excluded patients with autoPEEP (img 2)
8/

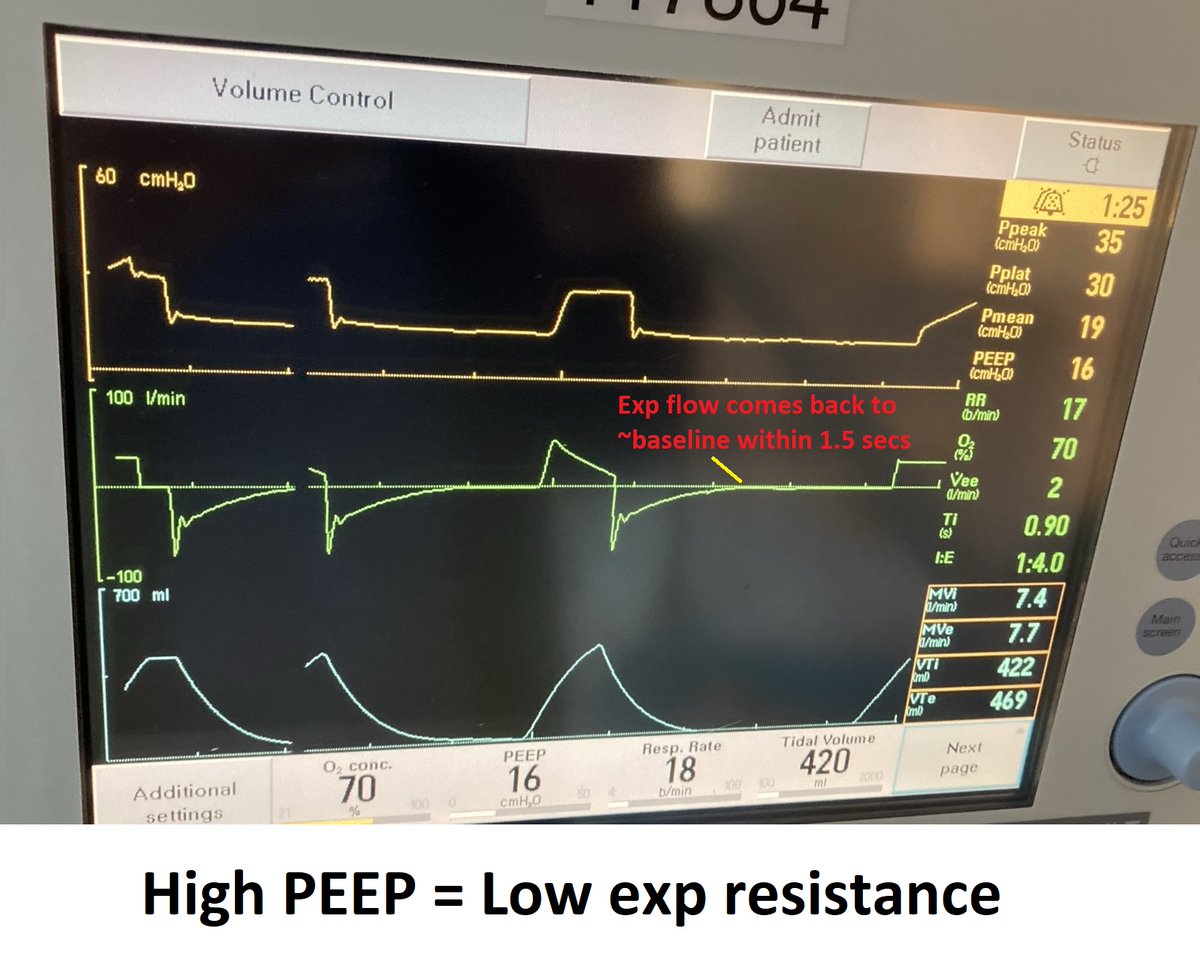
Is there concern for autoPEEP in our patient?
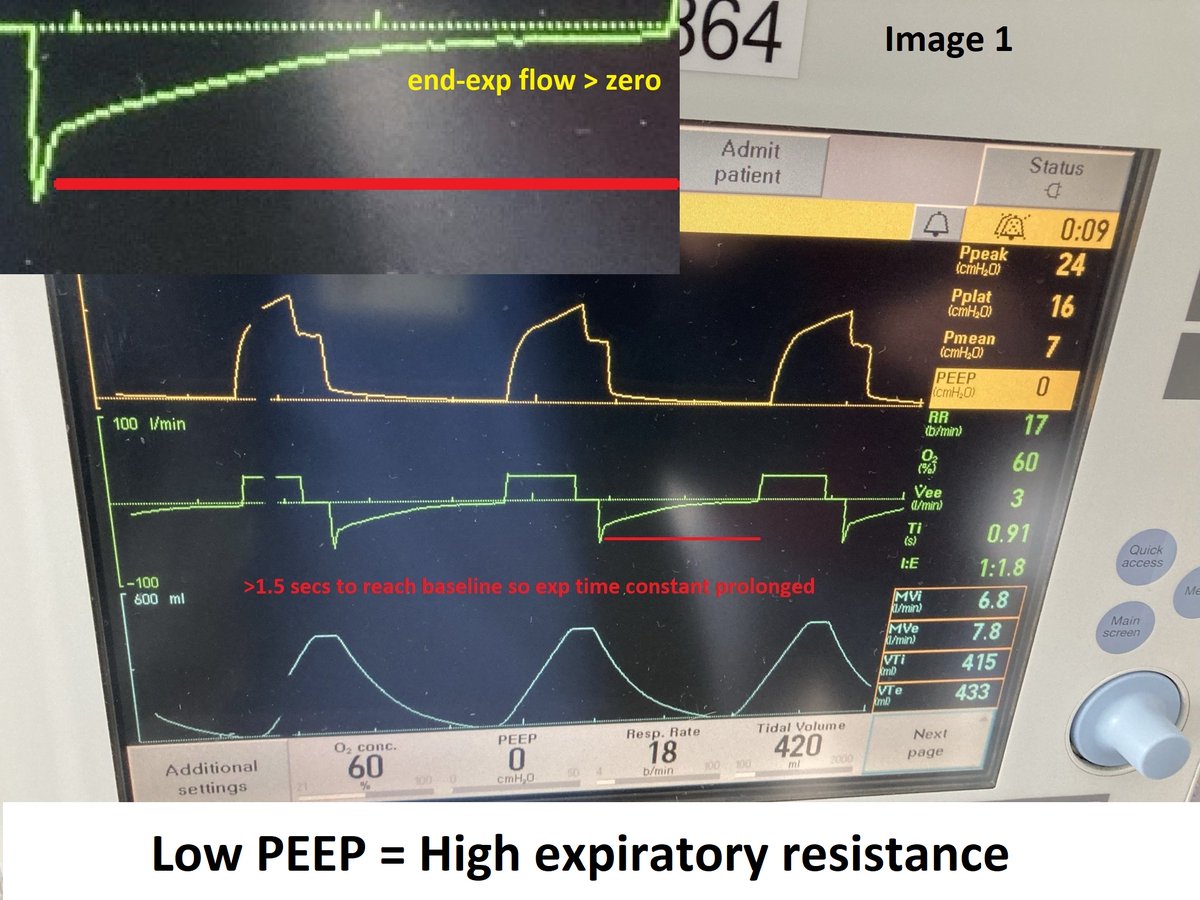
It may be tough to appreciate due to the scale but the flow does not come back to baseline (also note end-exp flow is 3).
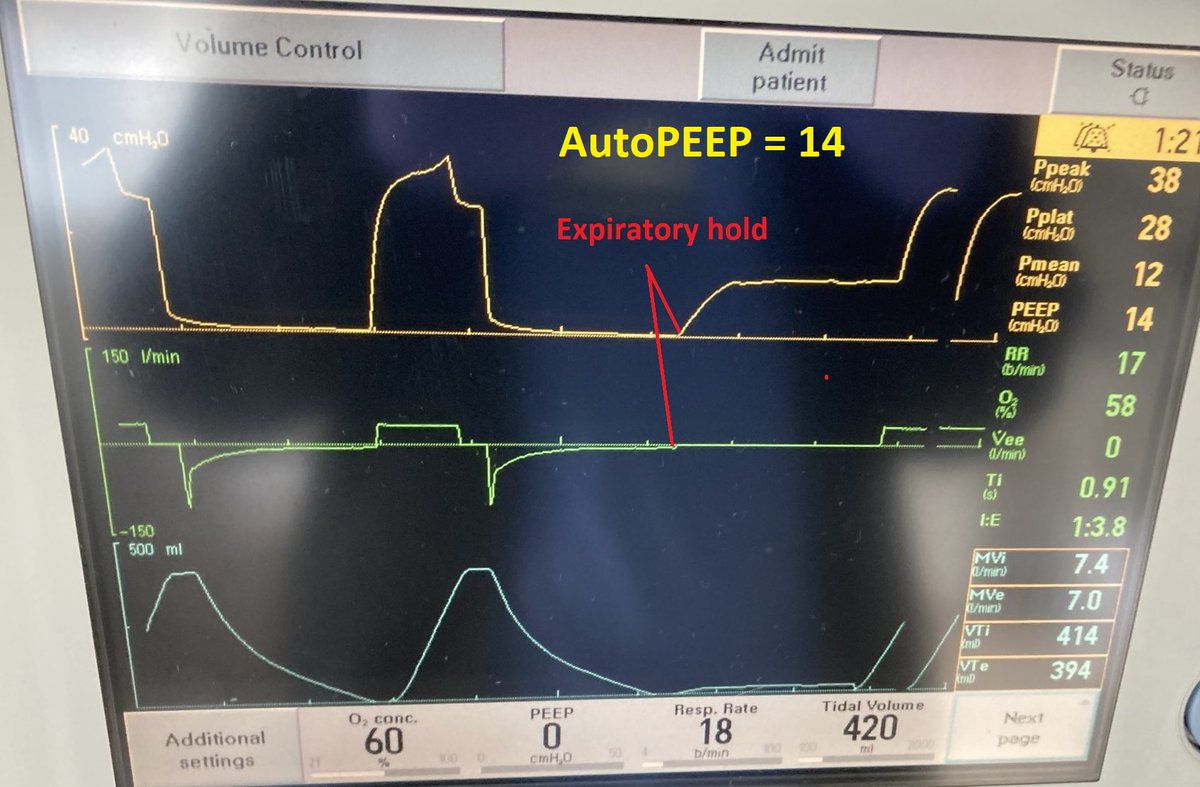
Here's a better example from a few hours later (image 1), followed by revelation of autoPEEP (image 2).
9/
It may be tough to appreciate due to the scale but the flow does not come back to baseline (also note end-exp flow is 3).
Here's a better example from a few hours later (image 1), followed by revelation of autoPEEP (image 2).
9/
Now let's characterize the loads in detail.
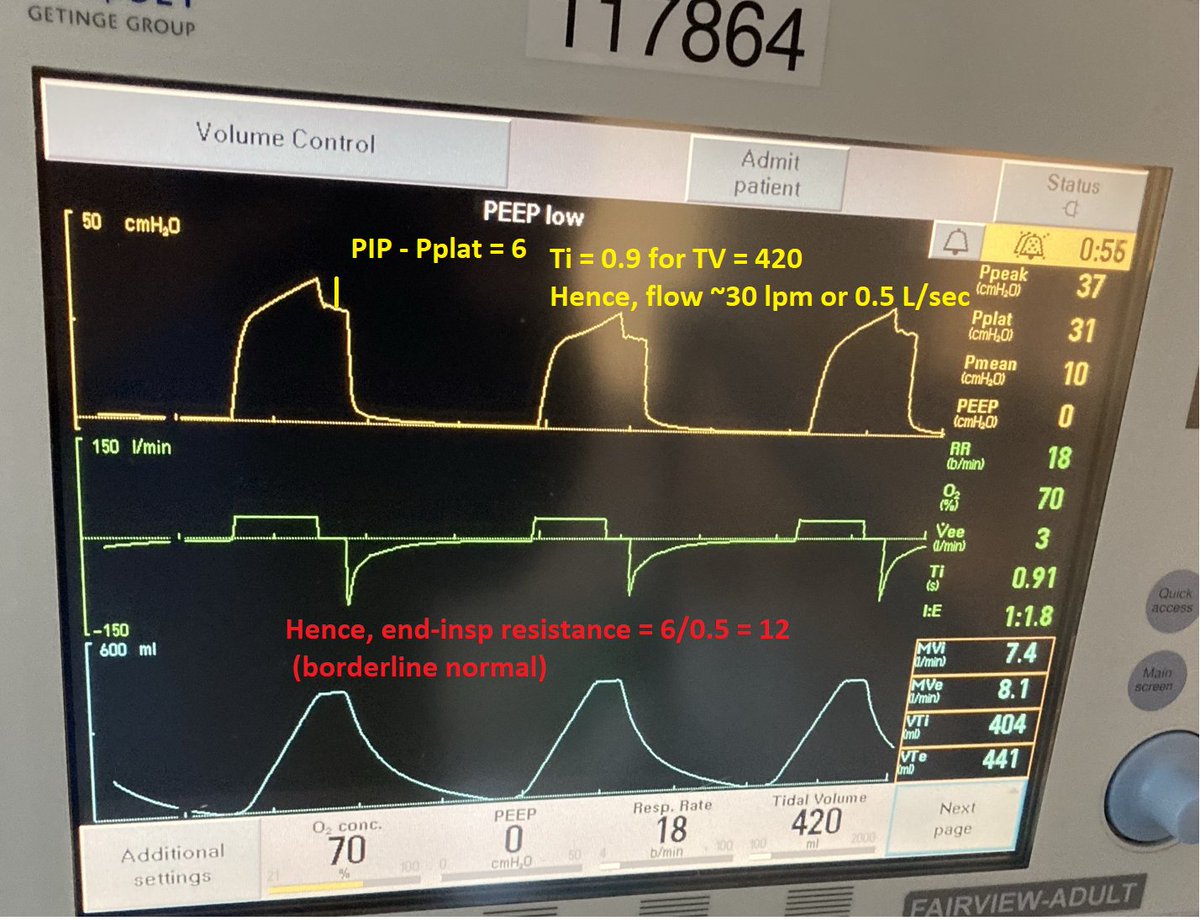
As already mentioned, the initial ⬆️ in Paw cannot be used to assess inspiratory load in patients with 'pattern X'. However PIP - Plat is only 6. Flow ~30 so end-insp resistance is ~12 cmH2O/L/sec (~normal)
What about expiration?
10/
As already mentioned, the initial ⬆️ in Paw cannot be used to assess inspiratory load in patients with 'pattern X'. However PIP - Plat is only 6. Flow ~30 so end-insp resistance is ~12 cmH2O/L/sec (~normal)
What about expiration?
10/
Expiratory time constant appears long and there is autoPEEP --> suggestive of resistive load during expiration (img 1)
This descrepancy between insp and exp loads is NOT typical of pattern X. A typical example in a patient with ARDS & airway closure can be found in imgs 2/3
11/
This descrepancy between insp and exp loads is NOT typical of pattern X. A typical example in a patient with ARDS & airway closure can be found in imgs 2/3
11/
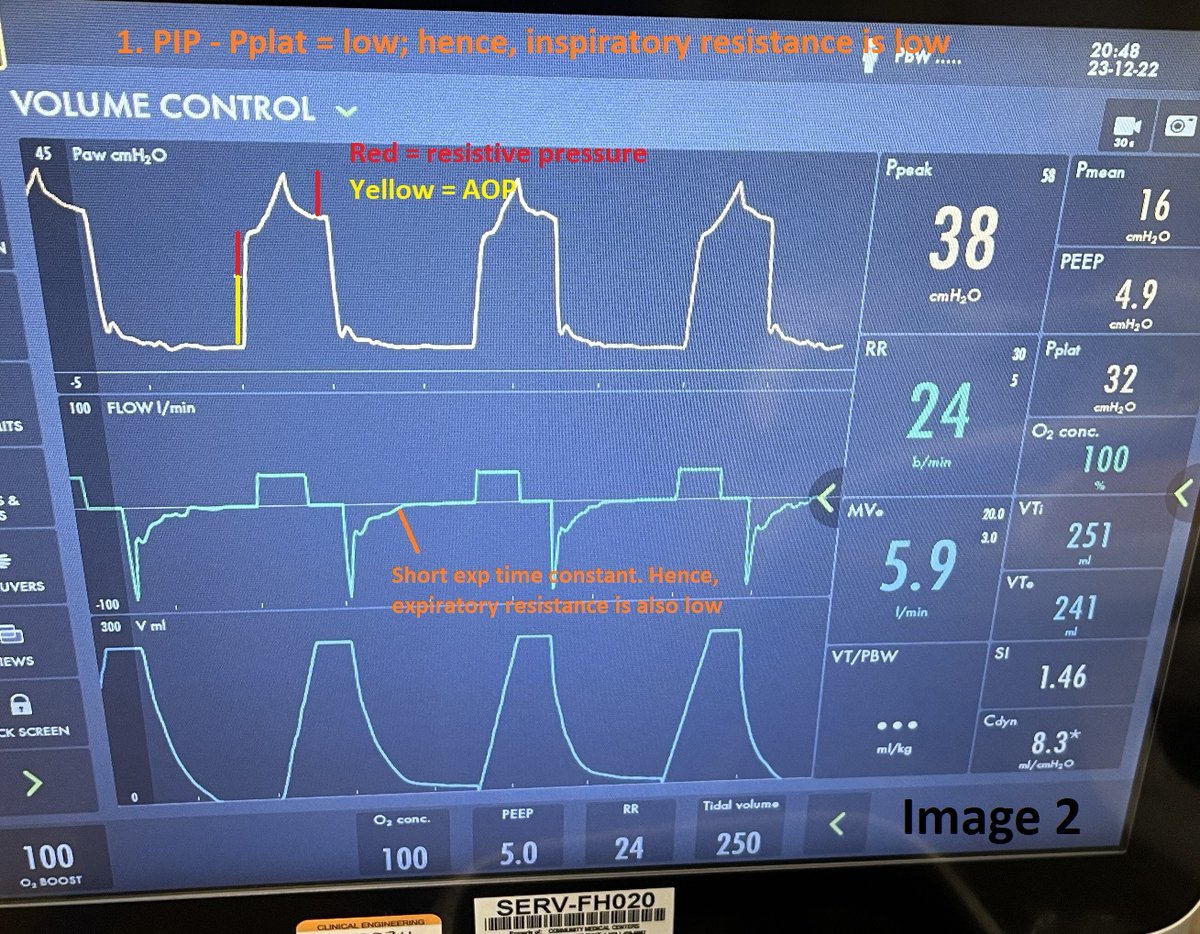
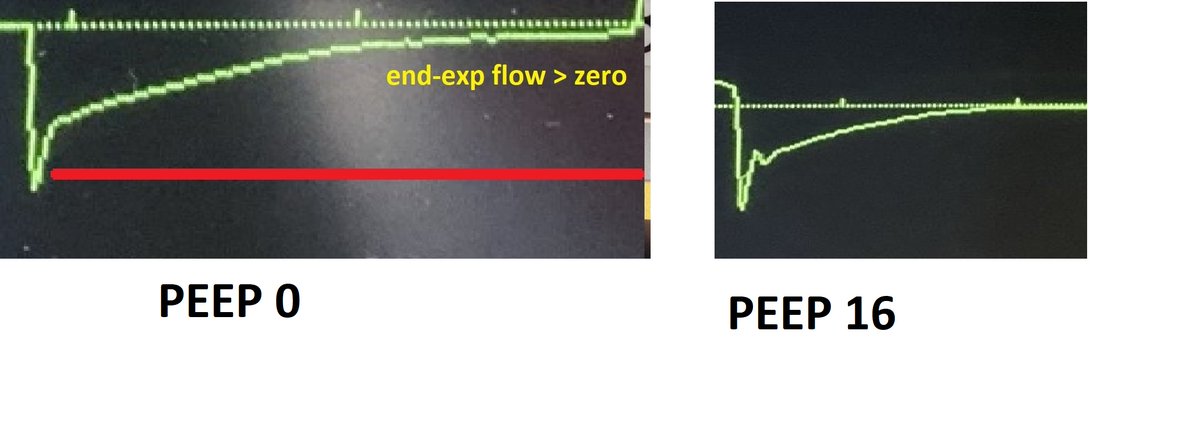
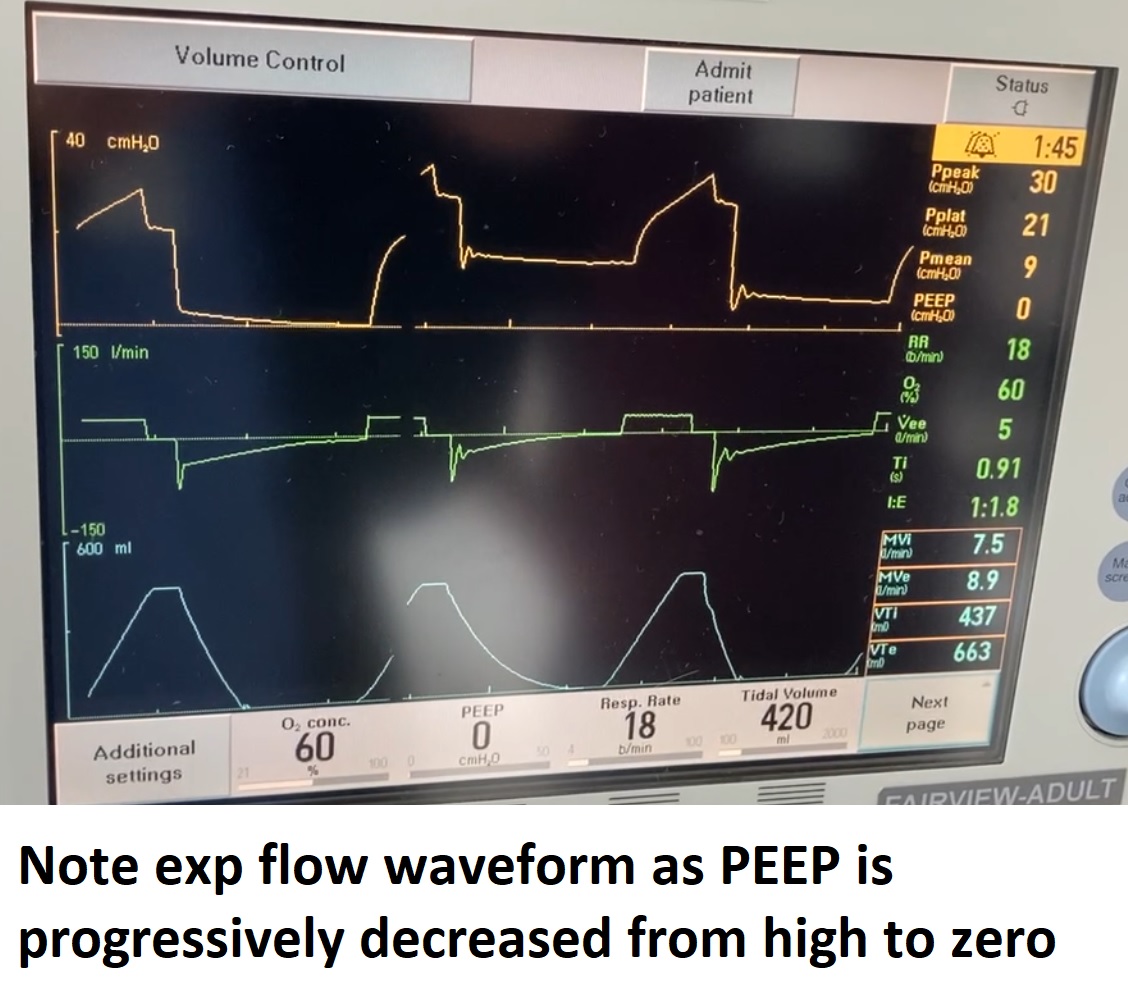
Furthermore, expiratory resistance seemed to vary significantly with PEEP setting! (see images)
This feature, along with the load descrapancy during insp & exp, is characteristic of a **dynamic airway obstruction**.
Here, positive pressure is mitigating the obstruction.
12/
This feature, along with the load descrapancy during insp & exp, is characteristic of a **dynamic airway obstruction**.
Here, positive pressure is mitigating the obstruction.
12/
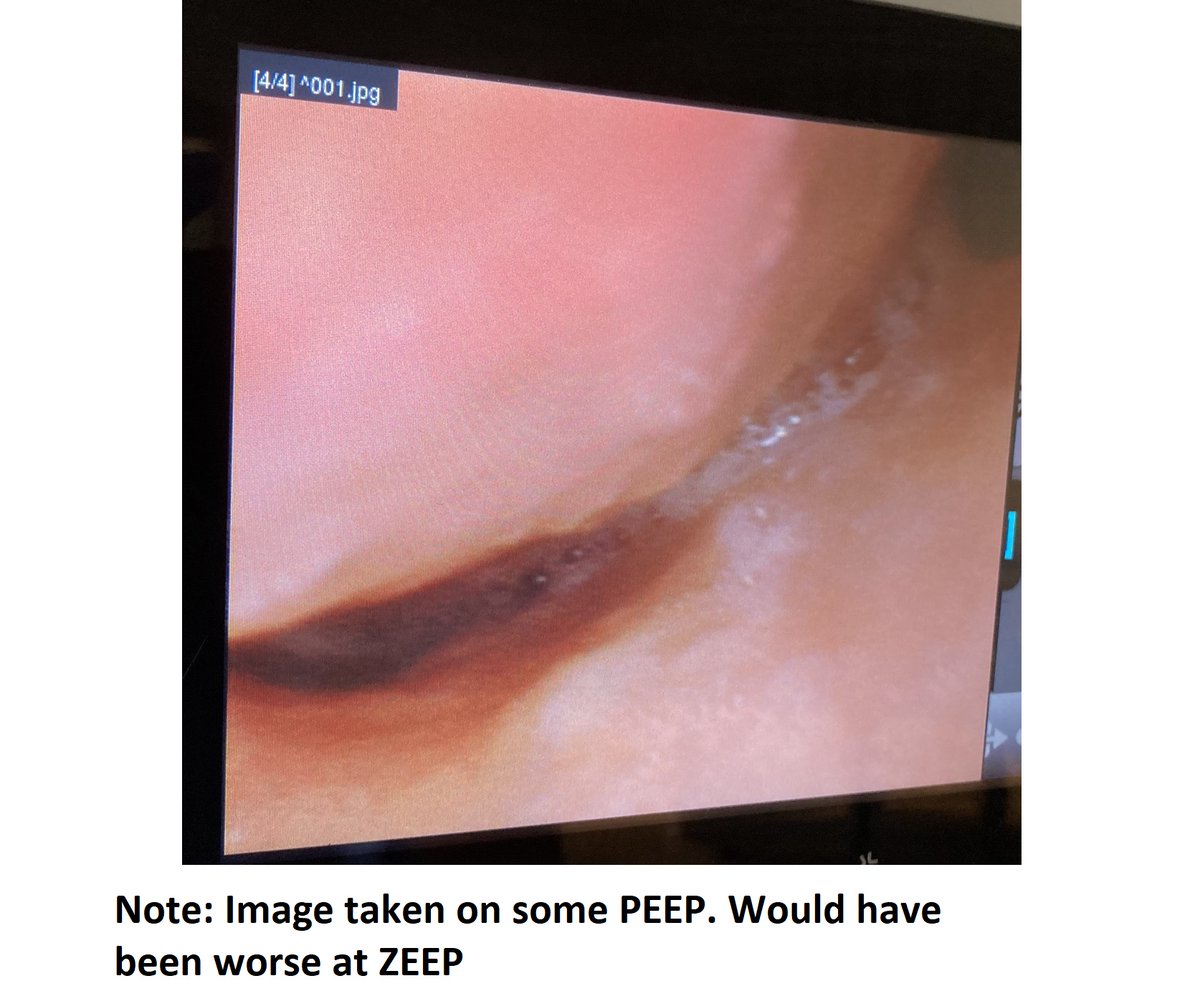
This patient had severe tracheobronchomalacia (TBM). There was some evidence of this on an old CT & the diagnosis was confirmed on bronchoscopy (img).
Unfortunately, the patient was not a candidate for stenting or surgical therapies & were eventually transitioned to comfort
13/
Unfortunately, the patient was not a candidate for stenting or surgical therapies & were eventually transitioned to comfort
13/
It has to be emphasized that the obstruction in this patient was extremely dynamic, with varying degrees of severity even at a particular PEEP.
Also, at least at one instant, the TBM did cause true/complete airway closure! (video)
14/
Also, at least at one instant, the TBM did cause true/complete airway closure! (video)
14/

In summary
-In VC+constant flow, Paw provides a lot of information about mechanics
-'Pattern X' can be seen in airway closure OR with presence of 'overt' autoPEEP
-Discrepant loads during insp & exp is NOT a typical feature of pattern X & suggests dynamic airway obstruction
15/
-In VC+constant flow, Paw provides a lot of information about mechanics
-'Pattern X' can be seen in airway closure OR with presence of 'overt' autoPEEP
-Discrepant loads during insp & exp is NOT a typical feature of pattern X & suggests dynamic airway obstruction
15/
- TBM can cause 'pattern X' by either mechanism - it's probably just a matter of whether the proximal airways are extremely narrow or completely closed!
- Severe TBM can cause critical autoPEEP and dynamic hyperinflation. Pertinent case reports - PMID: 30838137, 25972973.
16/
- Severe TBM can cause critical autoPEEP and dynamic hyperinflation. Pertinent case reports - PMID: 30838137, 25972973.
16/
Like I said, this was a fun one. Feel free to share your thoughts!
/Fin
cc @emireles_c @msiuba @DrMiguelIbarra1 @MegriMohammed @IM_Crit_ @OfVentilation @efan75 @MayoVentilation @DrivingPressure @RespiratorySCCM @ParijatSen11 @ventilacionmeca @roeckler @ThePlugWG @ArielG_RRT
/Fin
cc @emireles_c @msiuba @DrMiguelIbarra1 @MegriMohammed @IM_Crit_ @OfVentilation @efan75 @MayoVentilation @DrivingPressure @RespiratorySCCM @ParijatSen11 @ventilacionmeca @roeckler @ThePlugWG @ArielG_RRT
Loading suggestions...