

(1/6): 5 myths of IV fluids 🦄
A 🧵that makes my soul cringe.
Please help spread the word 🙏#stopinhospitaldrowning
A 🧵that makes my soul cringe.
Please help spread the word 🙏#stopinhospitaldrowning

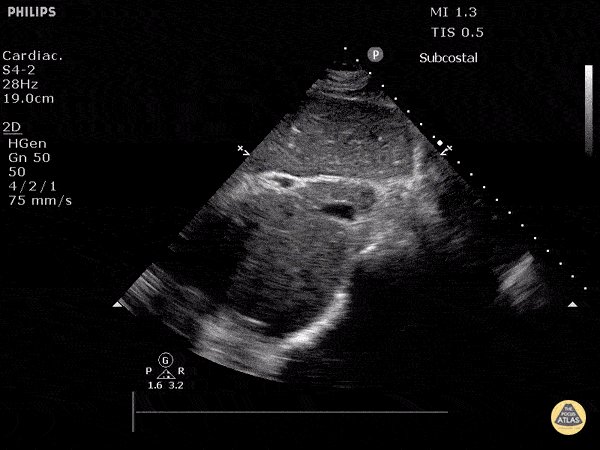
(2/6) Myth 1: You should resuscitate and "fill up" the IVC - "there is still room based on the IVC to give fluids..."
Response: We are not car mechanics filling up oil 🛢️
Response 2: IVC can be flat in hypovolemia OR distributive shock OR normal healthy state and does NOT predict fluid responsiveness 🚫
IVC needs to be decoupled entirely from fluid responsiveness. Yes it can tell us a little about tolerance, but NOT responsiveness. ❗️
Response: We are not car mechanics filling up oil 🛢️
Response 2: IVC can be flat in hypovolemia OR distributive shock OR normal healthy state and does NOT predict fluid responsiveness 🚫
IVC needs to be decoupled entirely from fluid responsiveness. Yes it can tell us a little about tolerance, but NOT responsiveness. ❗️
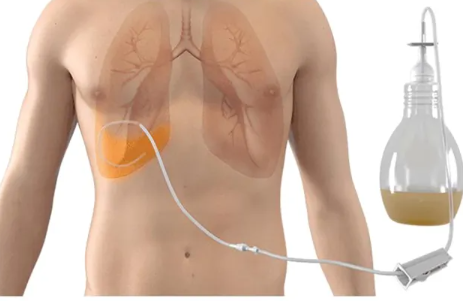
(3/6) Myth 2: Volume overload doesn’t matter early on in the ED or ICU – we can just diurese them later the ICU. 🌊🌊🌊
Response: Volume overload is associated with increased ICU, hospital length of stay ($$) AND death. Outcomes are better if we prevent volume overload than treat it.
Response: Volume overload is associated with increased ICU, hospital length of stay ($$) AND death. Outcomes are better if we prevent volume overload than treat it.
(4/6) Myth 3: My patient’s kidneys are "borderline" - if I don't give them enough fluid they will fail.
Response: IV fluids are not intrinsically beneficial to kidneys. They only help kidneys if the patient is fluid responsive and fluid tolerant. IV fluids can worsen venous congestion and kidney failure
Response: IV fluids are not intrinsically beneficial to kidneys. They only help kidneys if the patient is fluid responsive and fluid tolerant. IV fluids can worsen venous congestion and kidney failure

(5/6) Myth 4: IV fluids are the mainstay treatment of sepsis! 🦠
Response: Early antibiotics and treating any source of sepsis (source control are the most important aspects of managing sepsis. Fluid management is giving a bit more or less salt water.
Response: Early antibiotics and treating any source of sepsis (source control are the most important aspects of managing sepsis. Fluid management is giving a bit more or less salt water.
(6/6) Myth 5: I just use [x test] to tell if my patient is dry
Insert the following as [x test]: Swan, PPV, IVC, POCUS, VEXUS, etc.
Response: Fluid management requires integration of perfusion assessment (microcirculation), fluid responsiveness, and fluid tolerance assessments
Insert the following as [x test]: Swan, PPV, IVC, POCUS, VEXUS, etc.
Response: Fluid management requires integration of perfusion assessment (microcirculation), fluid responsiveness, and fluid tolerance assessments
![(6/6) Myth 5: I just use [x test] to tell if my patient is dry
Insert the following as [x test]: Sw...](https://pbs.twimg.com/media/GFH6HUwWwAELWd4.jpg)
Loading suggestions...