


✅Pre-operative RT reduces the risk of pelvic recurrence for patients with rectal cancer.
But some patients will suffer from acute and long term toxicity (bladder, bowel, sexual, endocrine dysfunction)
❓How can we tailor therapy to balance QoL & cancer control?
2/
But some patients will suffer from acute and long term toxicity (bladder, bowel, sexual, endocrine dysfunction)
❓How can we tailor therapy to balance QoL & cancer control?
2/

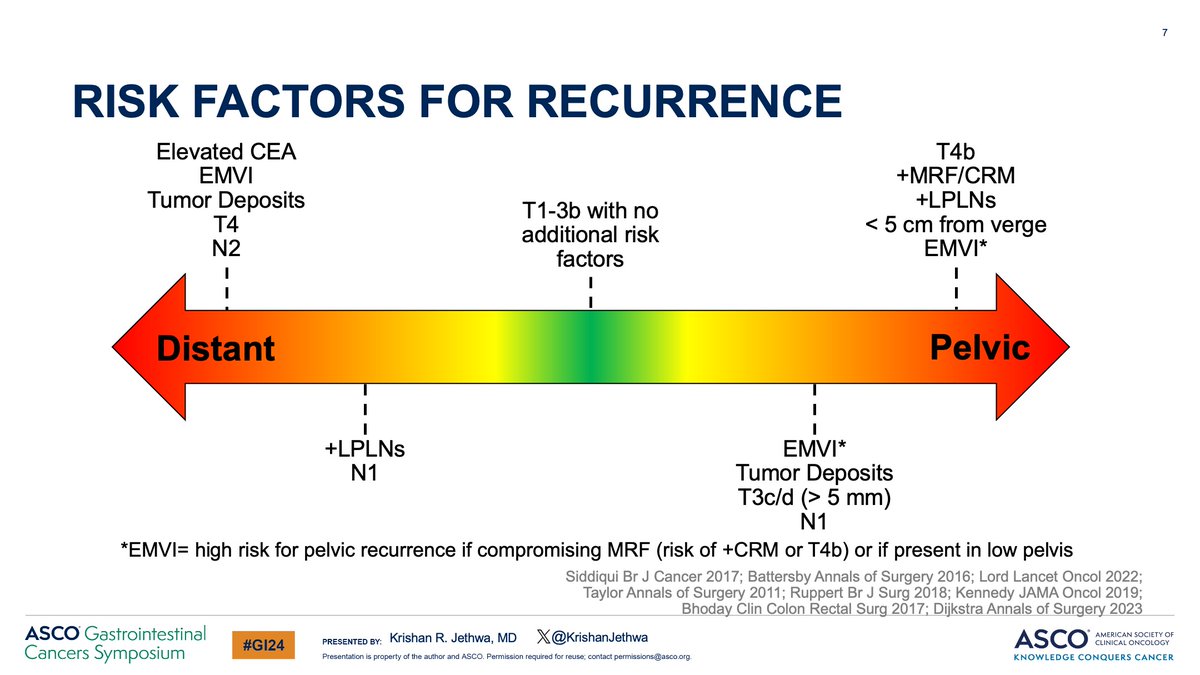
Rectal cancer is highly heterogeneous with a broad spectrum of risk for both pelvic and distant recurrence.
🔥🔥🔥 Understanding risk of recurrence is critical in clinical decision making!
3/
🔥🔥🔥 Understanding risk of recurrence is critical in clinical decision making!
3/

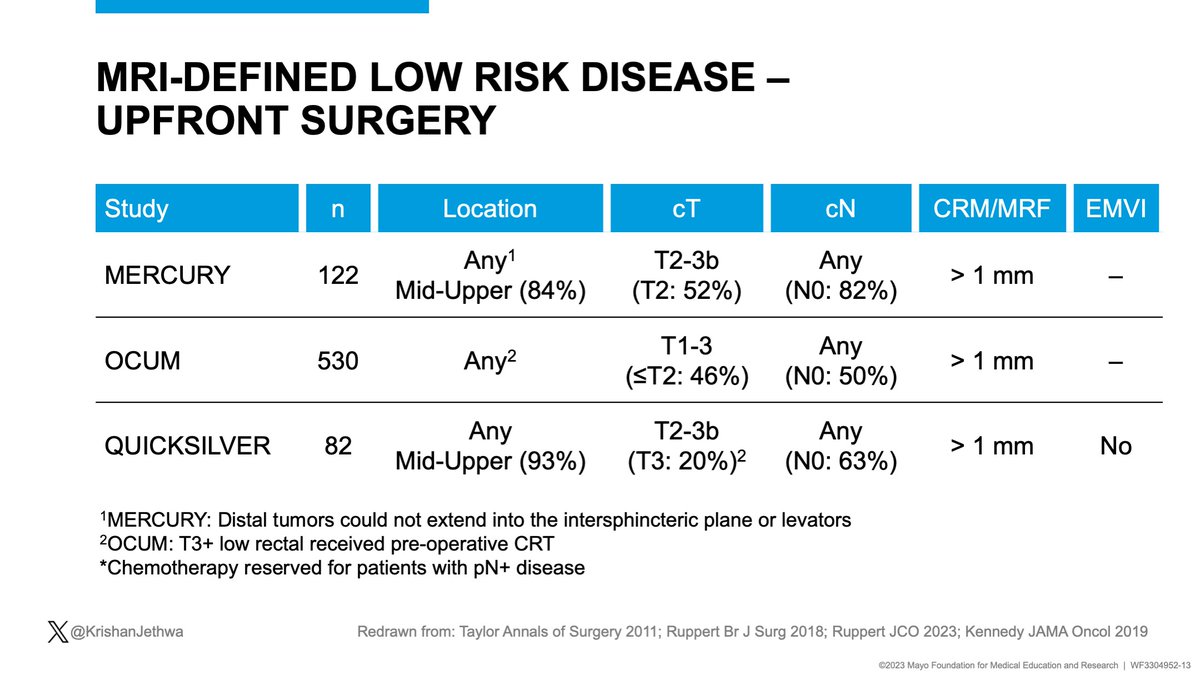
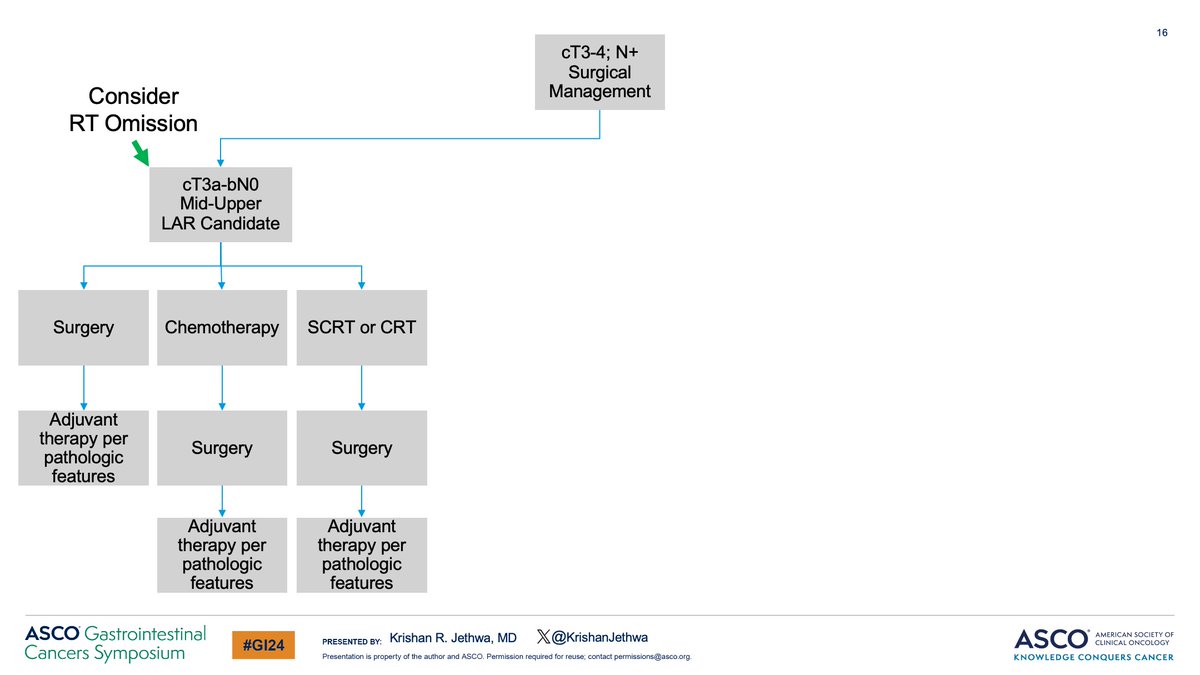
Which pts may omit RT?
Mercury, OCUM, and Quicksilver included pts with predominately mid-upper rectal cancers, T2-3bN0, clear MRF, and no EMVI
Patients treated with up-front surgery
Chemotherapy only for pN+ patients
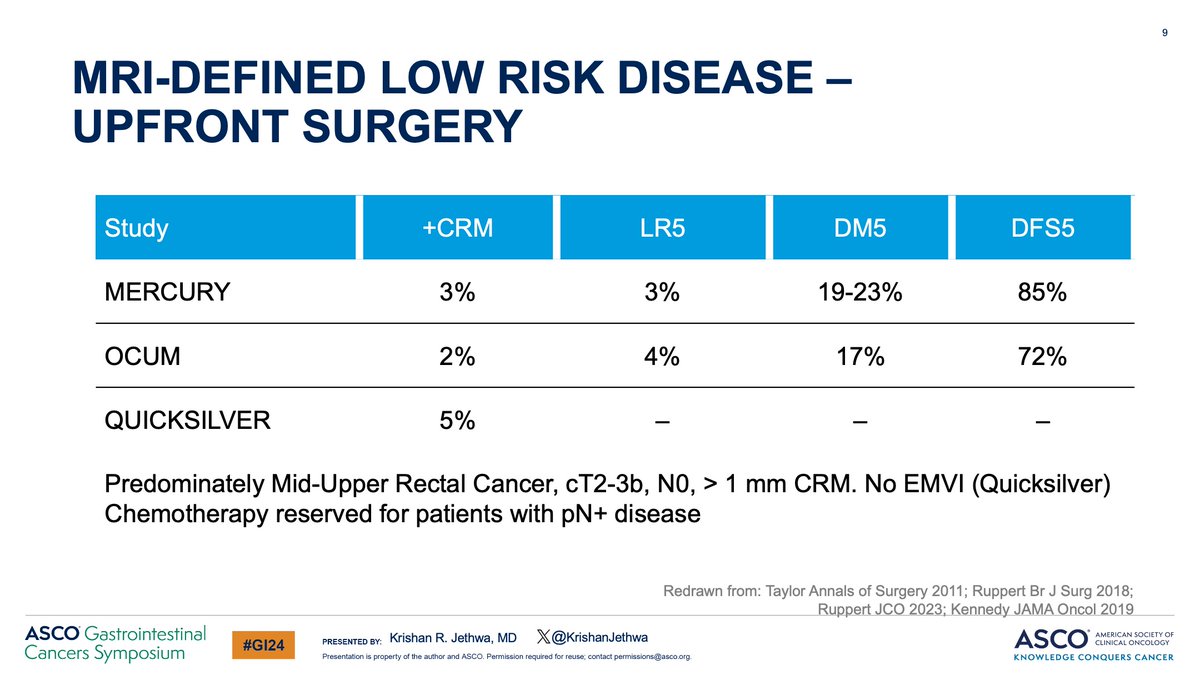
✅ < 5% + margins
✅< 5% 5-year pelvic recurrence
4/
Mercury, OCUM, and Quicksilver included pts with predominately mid-upper rectal cancers, T2-3bN0, clear MRF, and no EMVI
Patients treated with up-front surgery
Chemotherapy only for pN+ patients
✅ < 5% + margins
✅< 5% 5-year pelvic recurrence
4/
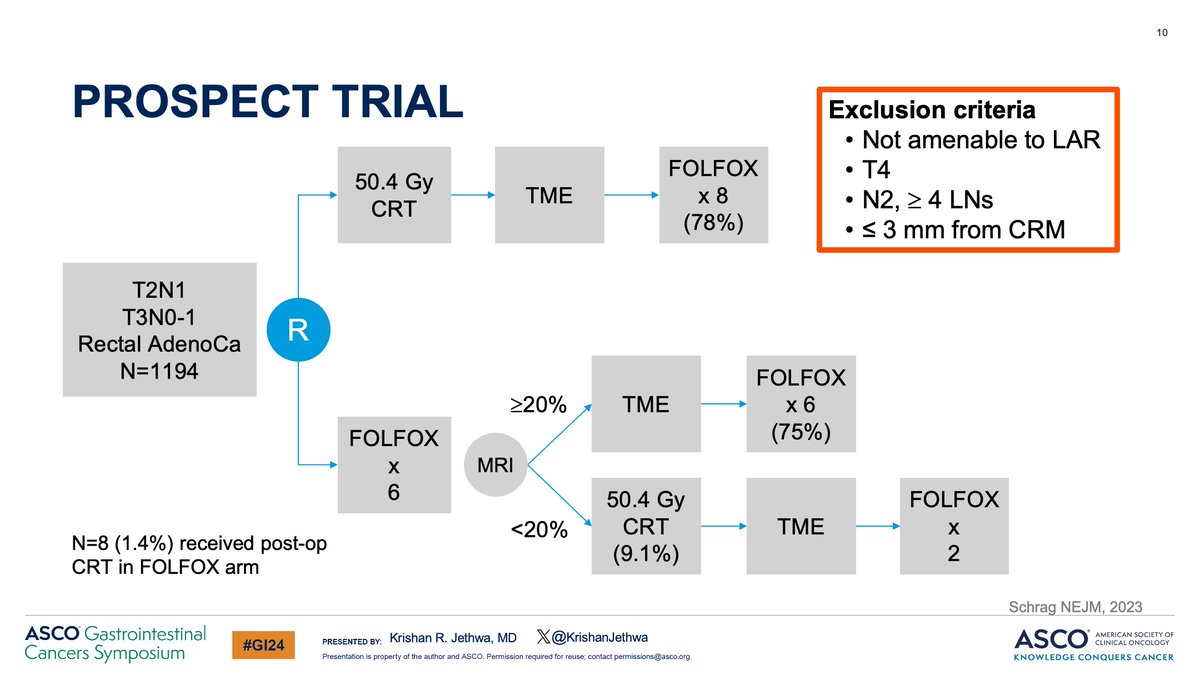
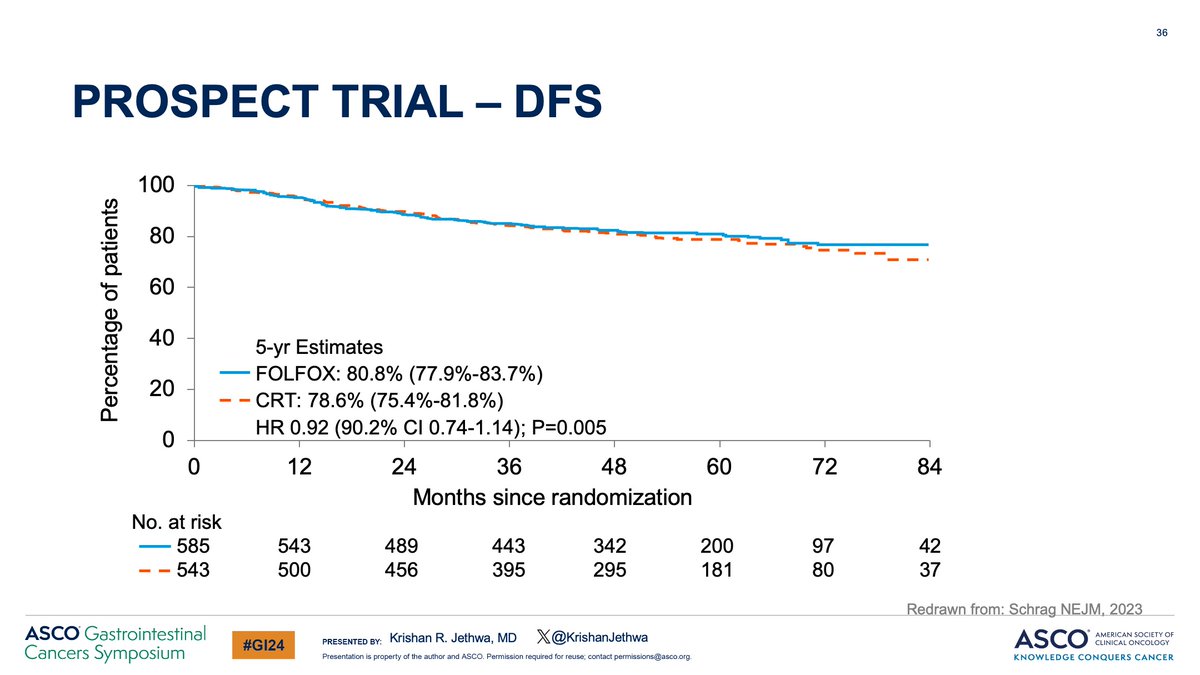
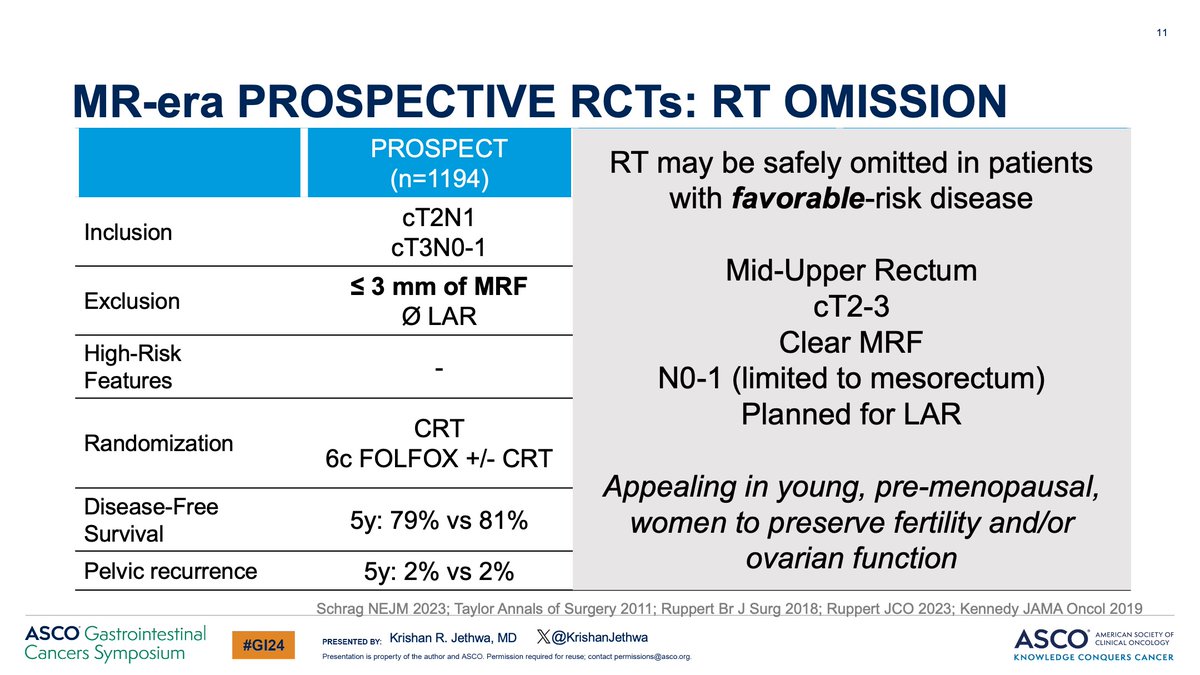
For pts with favorable risk cT3N0-1/cT2N1 rectal cancer amenable to LAR, PROSPECT compared:
LC-CRT
vs
Pre-op chemo +/- selective CRT
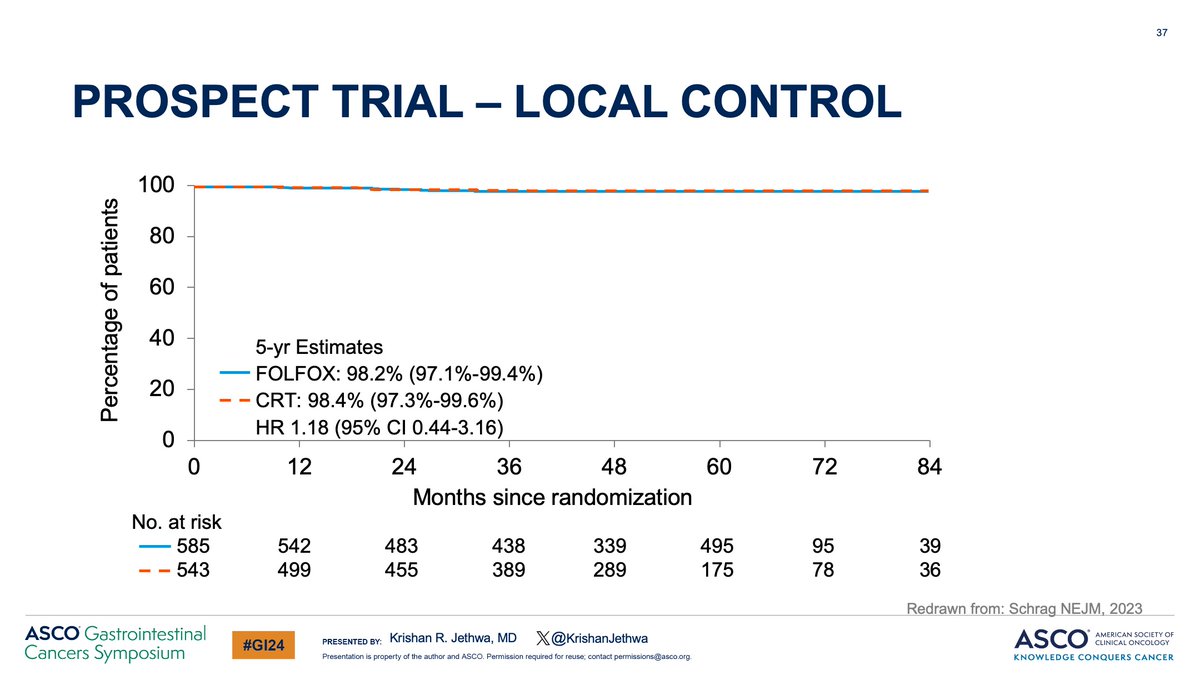
Study found no detriment in:
✅Local control
✅Disease free survival
✅Overall survival
BUT
🔺 pre-op toxicity with FOLFOX
5/
LC-CRT
vs
Pre-op chemo +/- selective CRT
Study found no detriment in:
✅Local control
✅Disease free survival
✅Overall survival
BUT
🔺 pre-op toxicity with FOLFOX
5/
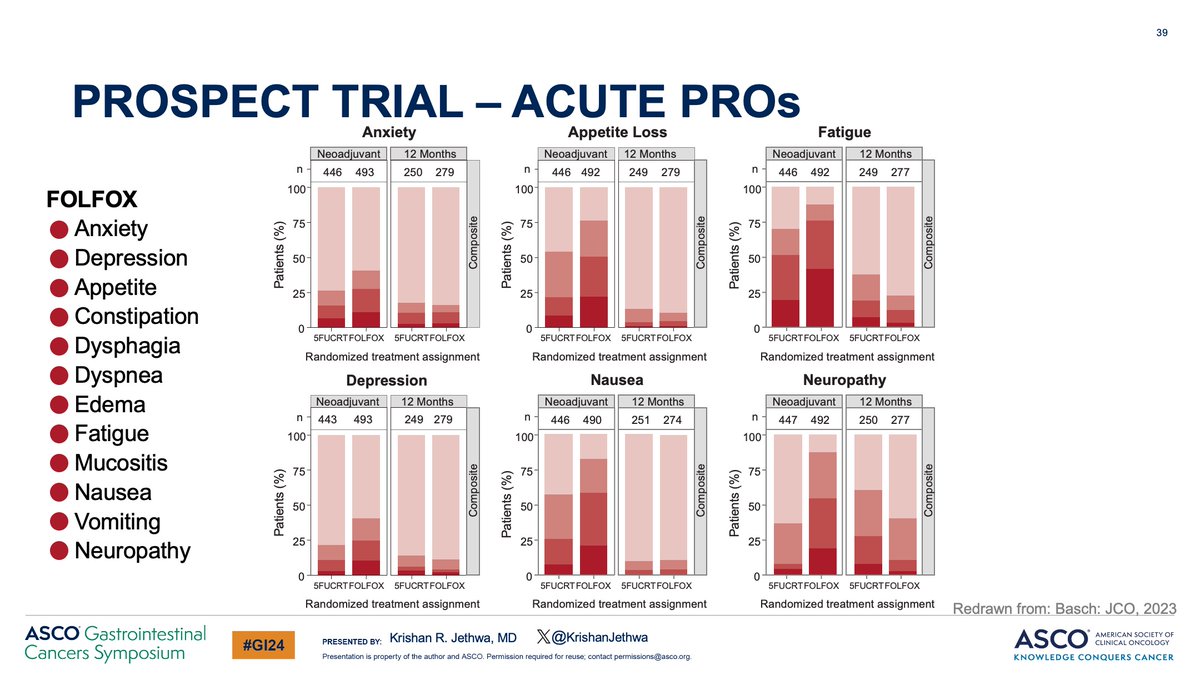
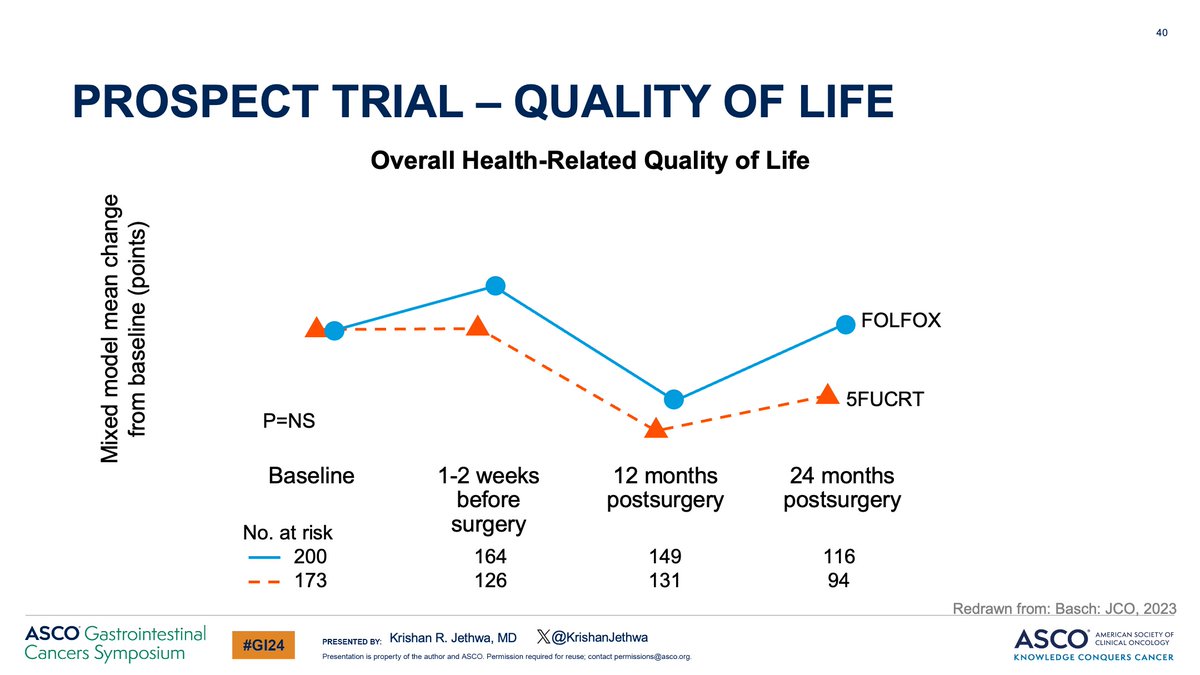
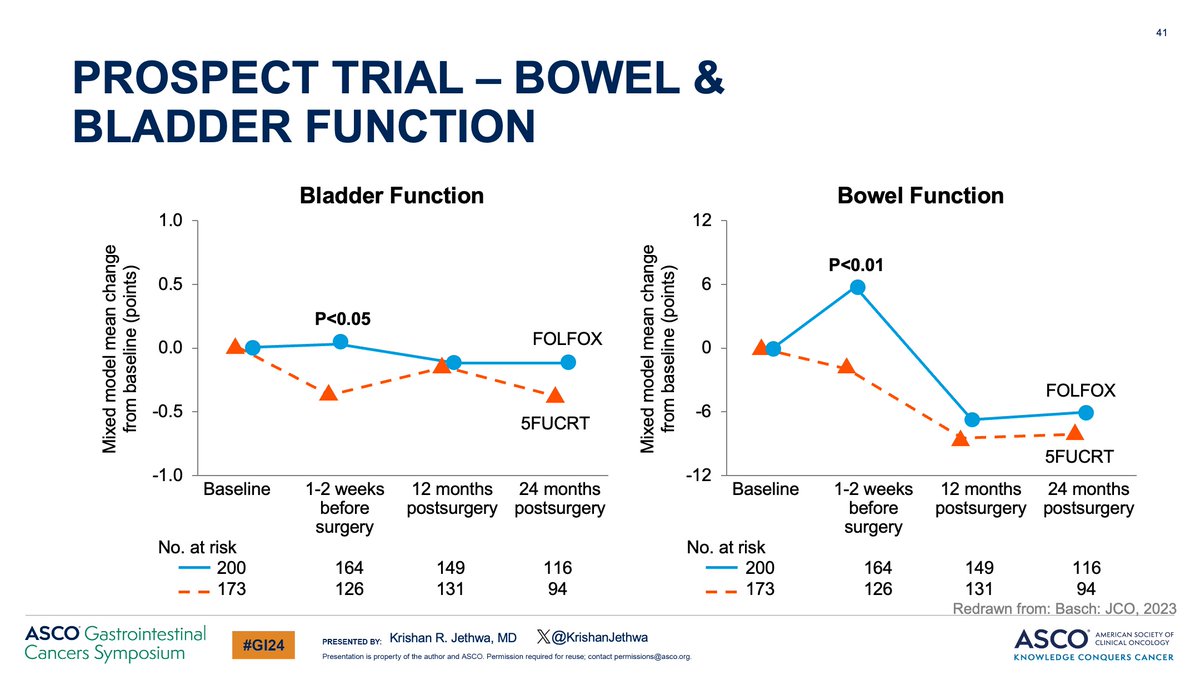
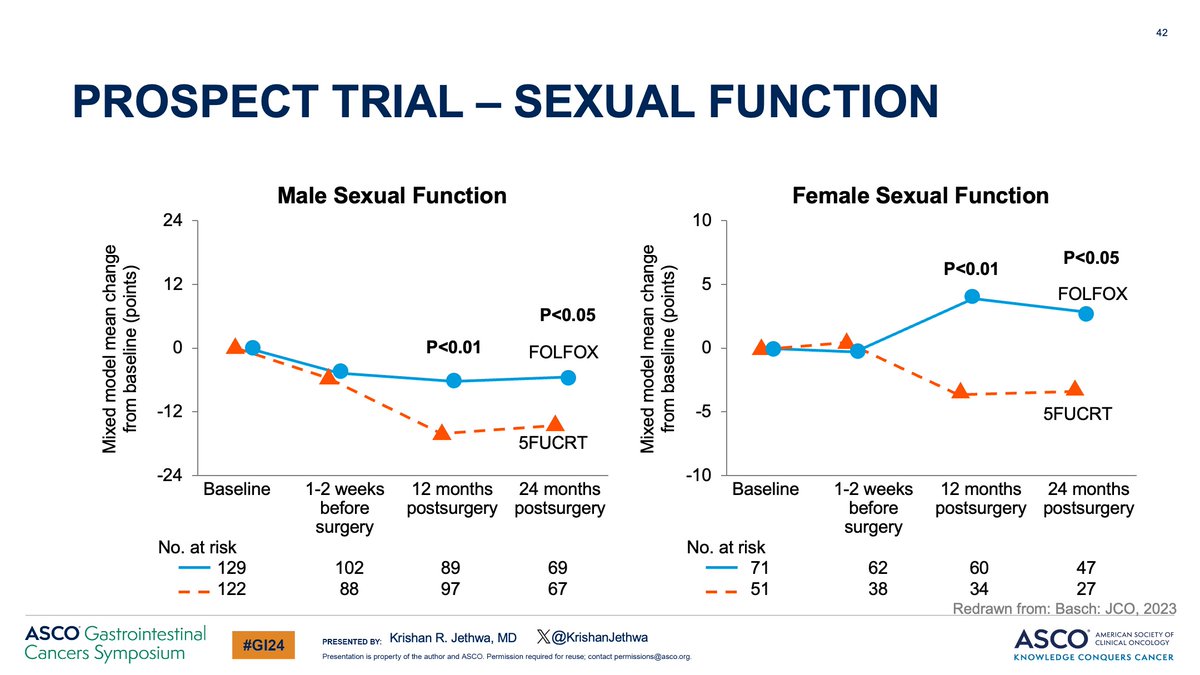
The study included robust collection of PROs which demonstrated:
There were substantial differences in acute PROs favoring CRT but
✅ No difference in overall QoL
✅ RT omission did better preserve sexual function
6/
There were substantial differences in acute PROs favoring CRT but
✅ No difference in overall QoL
✅ RT omission did better preserve sexual function
6/
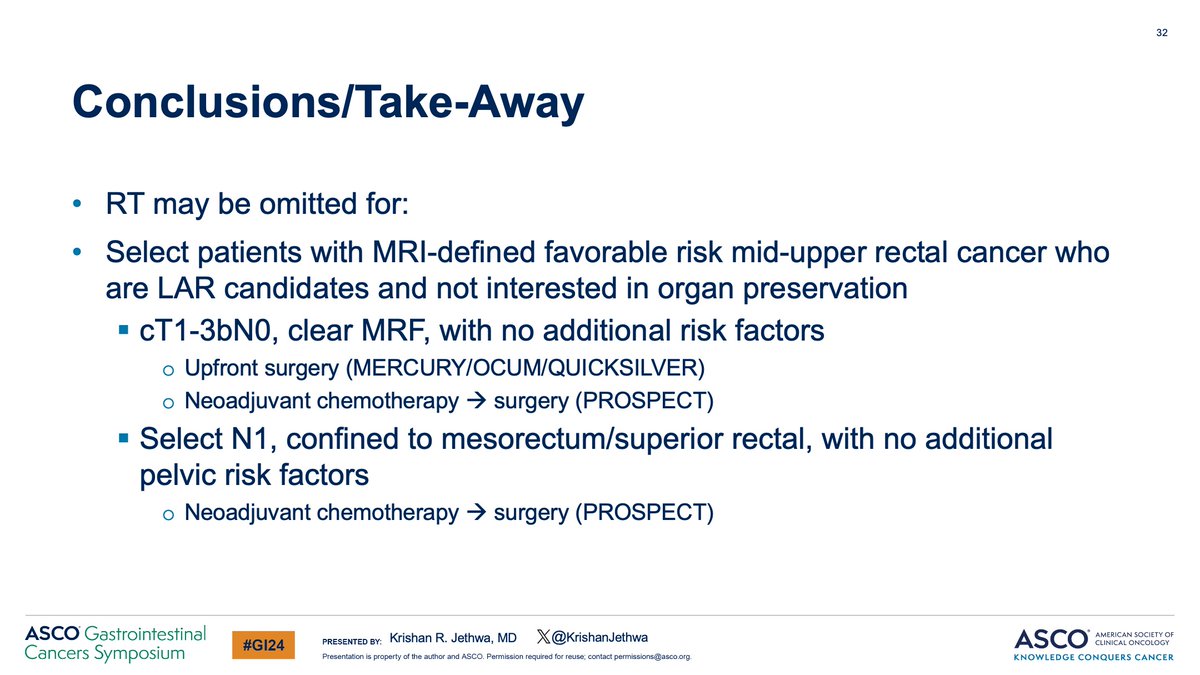
Based upon these data, RT may be safely omitted in patients with favorable risk LARC, including those with:
✅Tumors in the mid-upper rectum
✅cT2-3
✅Clear MRF
✅N0-1, limited to the mesorectum
✅Planned for surgery with a LAR
7/
✅Tumors in the mid-upper rectum
✅cT2-3
✅Clear MRF
✅N0-1, limited to the mesorectum
✅Planned for surgery with a LAR
7/
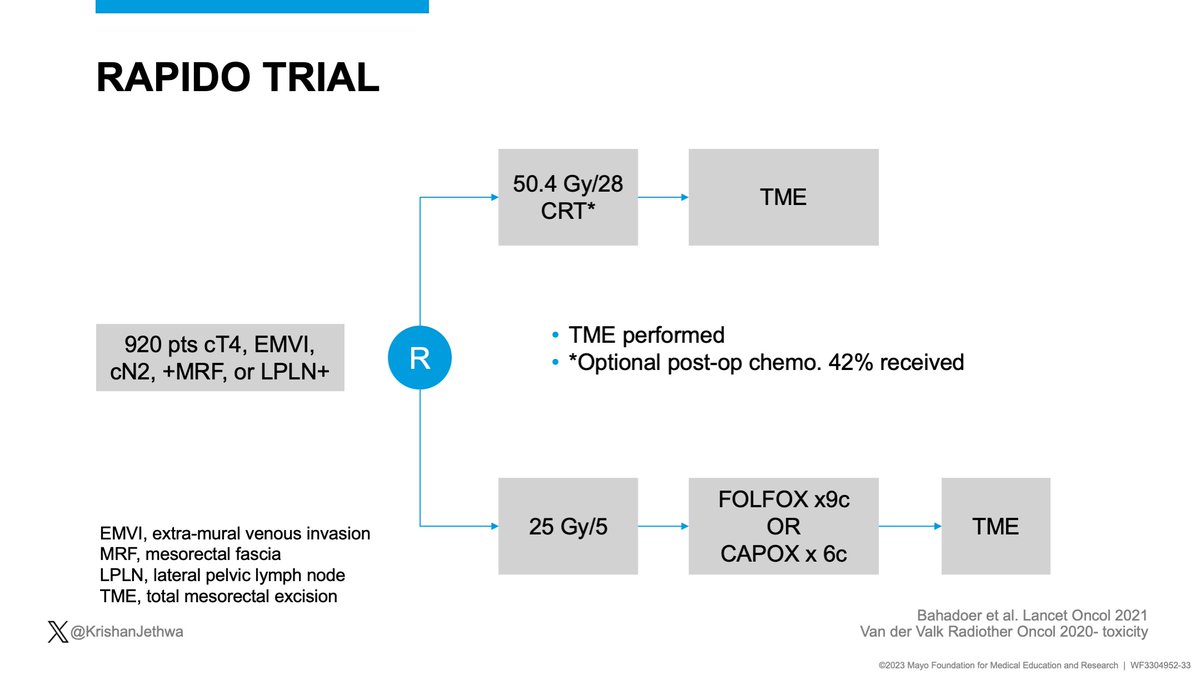
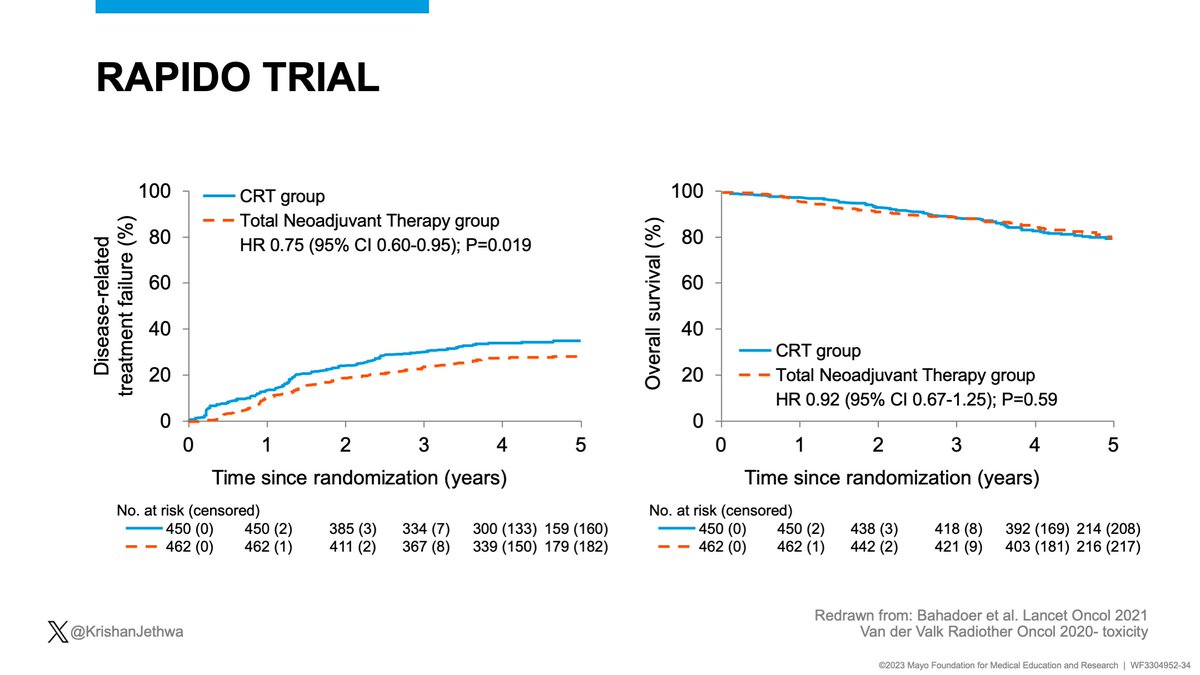
What about high-risk rectal cancer?
RAPIDO included pts with T4, cN2, +EMVI, +MRF, or +LPNs.
Randomized:
CRT (Adj chemo optional: 42% received)
vs.
Intensified TNT regimen of SC-RT➡️FOLFOX.
Key results improved with TNT:
✅⬇️Disease related treatment failure
✅Decreased DM
8/
RAPIDO included pts with T4, cN2, +EMVI, +MRF, or +LPNs.
Randomized:
CRT (Adj chemo optional: 42% received)
vs.
Intensified TNT regimen of SC-RT➡️FOLFOX.
Key results improved with TNT:
✅⬇️Disease related treatment failure
✅Decreased DM
8/
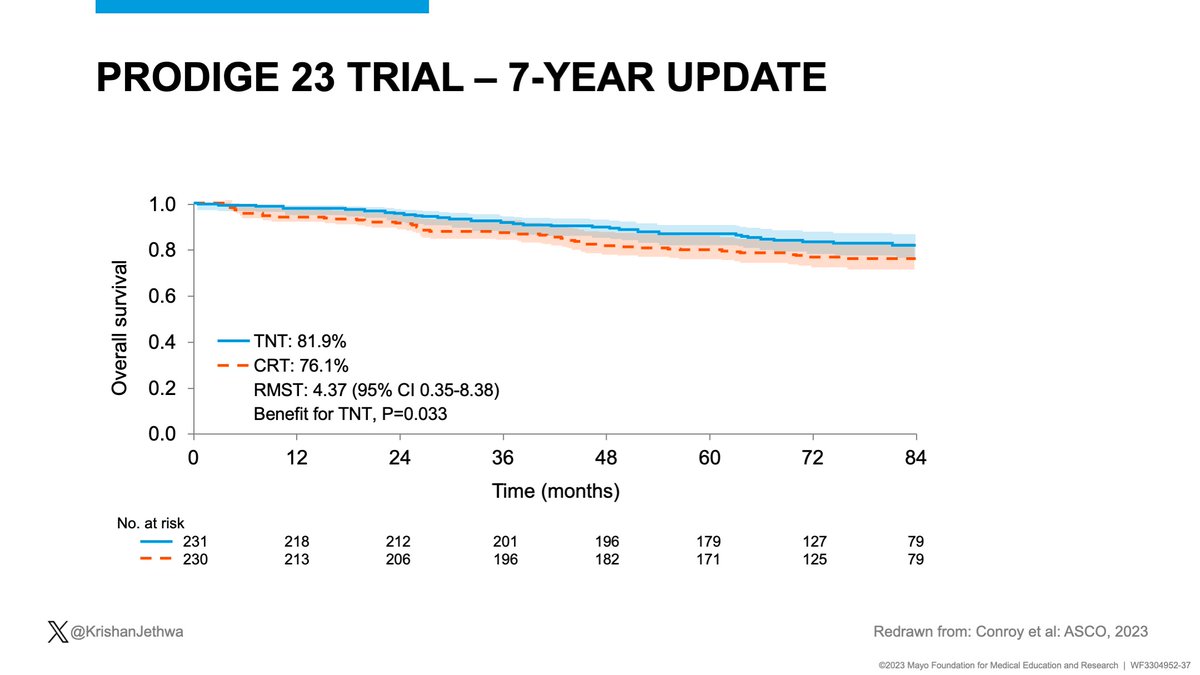
PRODIGE 23 included pts with cT3-4 disease
Randomized:
CRT➡️FOLFOX
vs.
mFOLFIRINOX ➡️CRT➡️S ➡️FOLFOX
Key results improved with TNT!
✅Improved DFS
✅Decreased DM
✅✅✅Improved OS!!!
9/
Randomized:
CRT➡️FOLFOX
vs.
mFOLFIRINOX ➡️CRT➡️S ➡️FOLFOX
Key results improved with TNT!
✅Improved DFS
✅Decreased DM
✅✅✅Improved OS!!!
9/


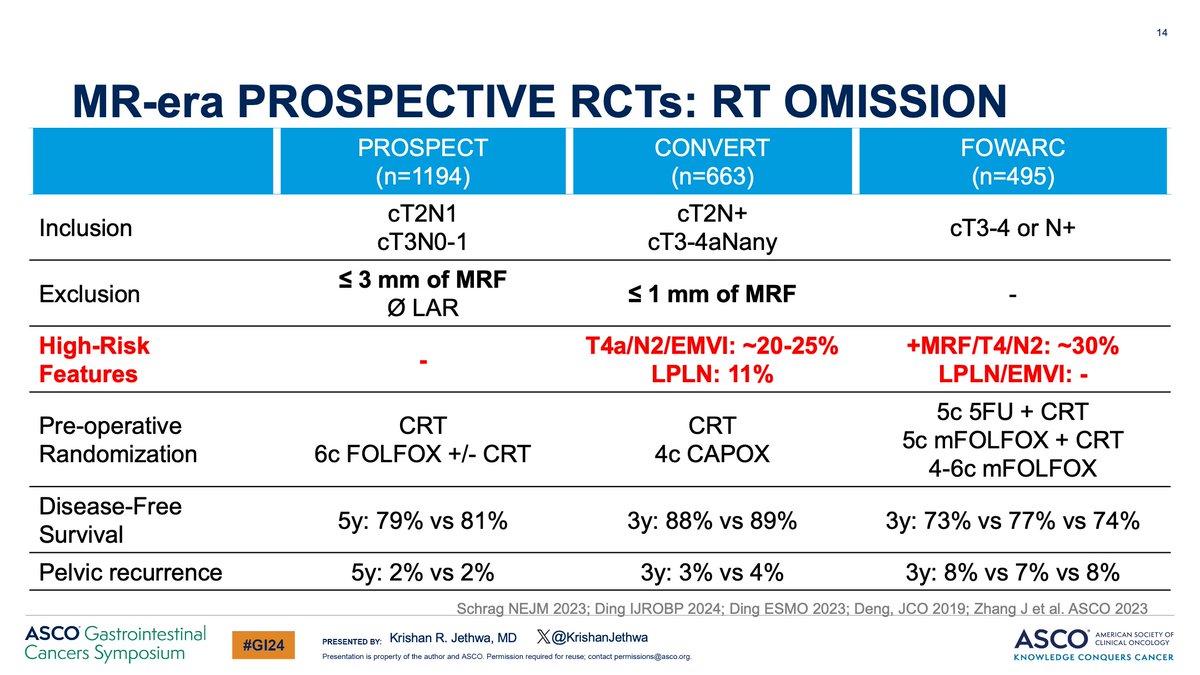
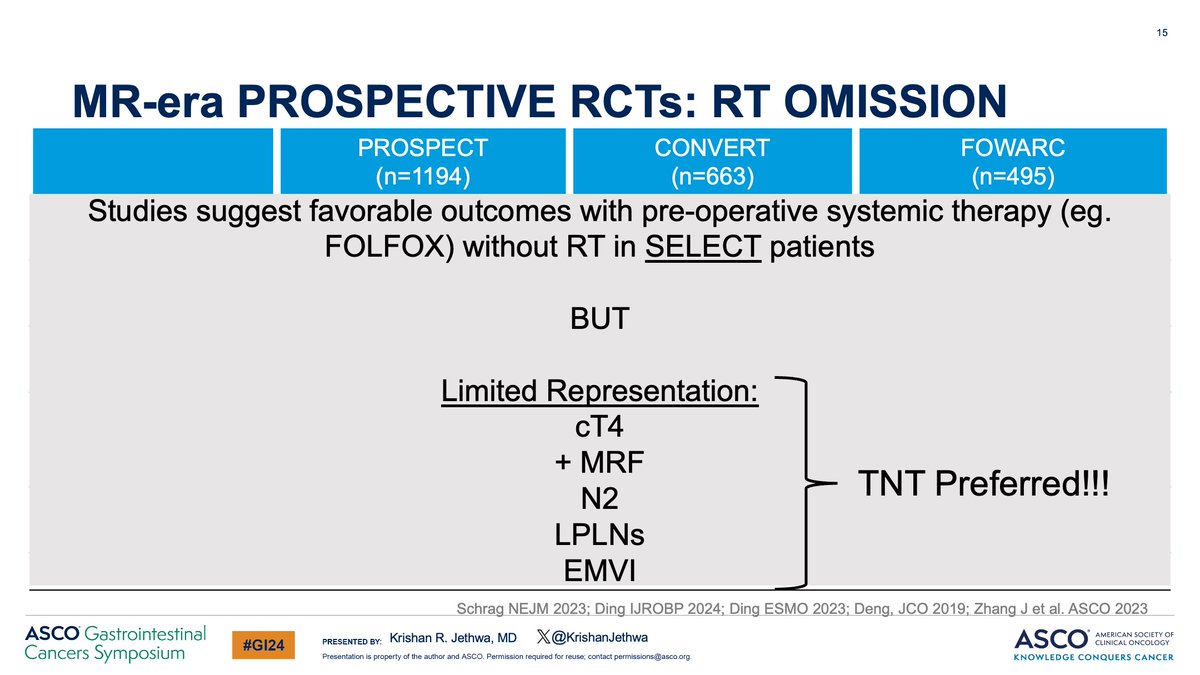
PROSPECT, CONVERT, and FOWARC suggest there is a subset of pts with LARC effectively treated with pre-op FOLFOX without RT
However, these studies had limited representation of high risk disease‼️
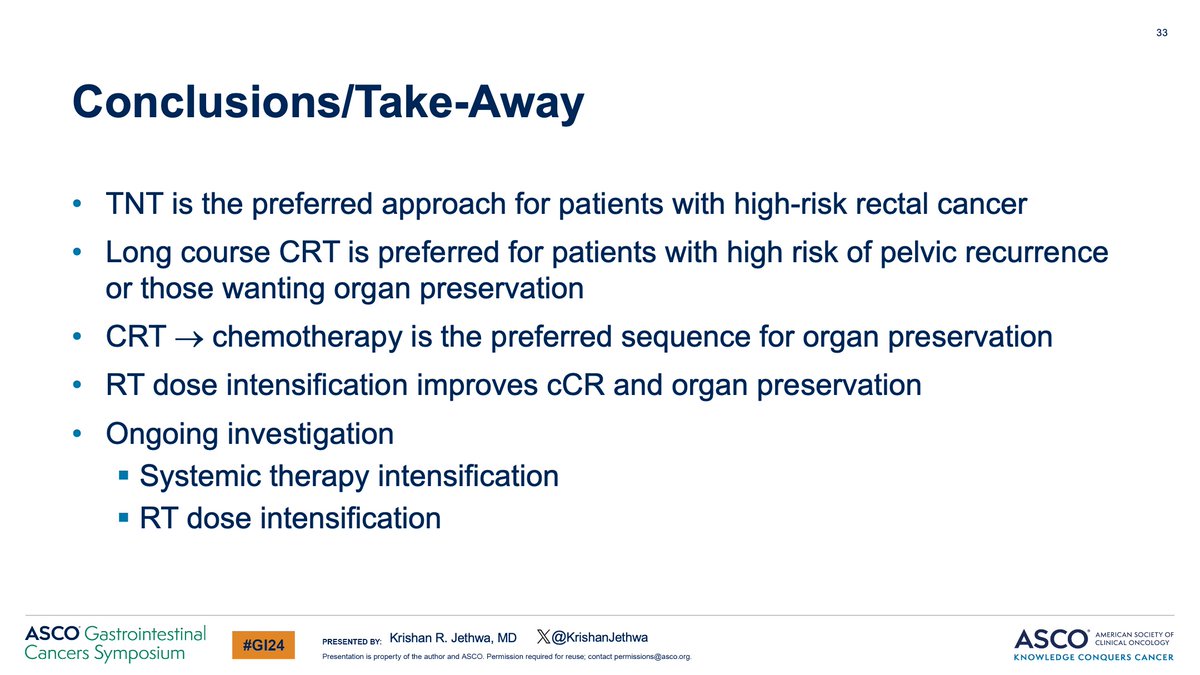
🔥 TNT, inclusive of RT, is preferred for patients with high risk disease!
10/
However, these studies had limited representation of high risk disease‼️
🔥 TNT, inclusive of RT, is preferred for patients with high risk disease!
10/
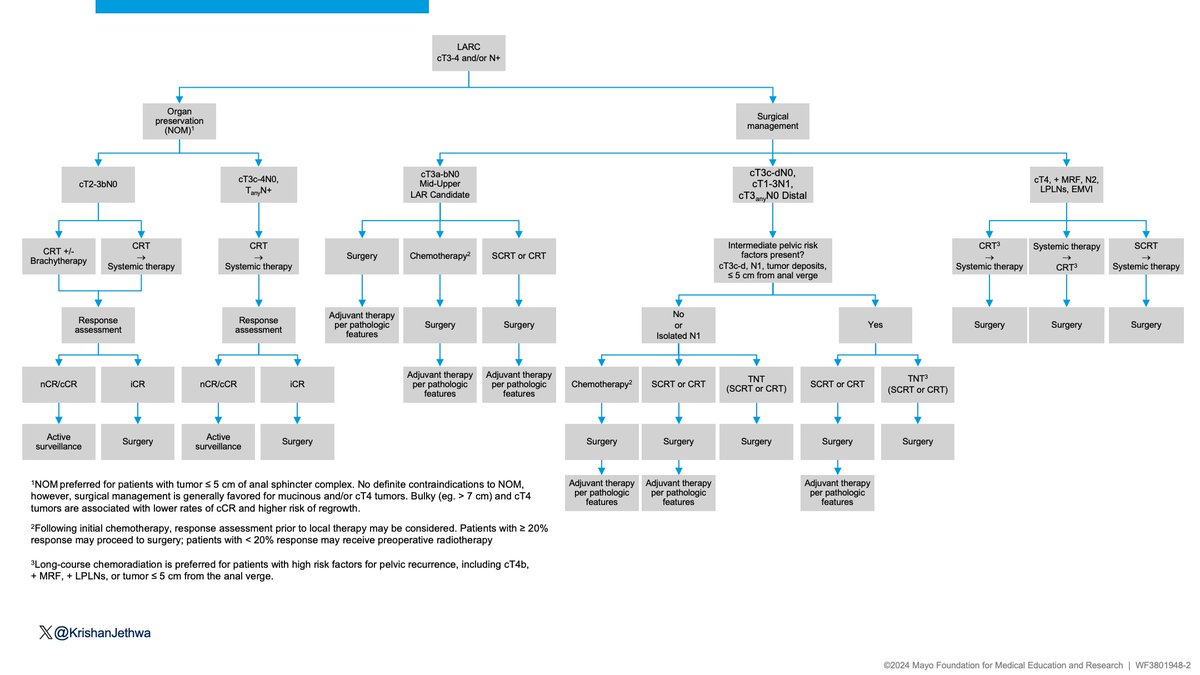
Let’s summarize!
🟢cT3a-bN0 tumors in the mid-upper rectum amenable to LAR with no additional risk factors ➡️ consider RT omission.
🔴High-risk rectal cancer (cT4, N2, + MRF, LPLNs, EMVI) ➡️ TNT
11/
🟢cT3a-bN0 tumors in the mid-upper rectum amenable to LAR with no additional risk factors ➡️ consider RT omission.
🔴High-risk rectal cancer (cT4, N2, + MRF, LPLNs, EMVI) ➡️ TNT
11/

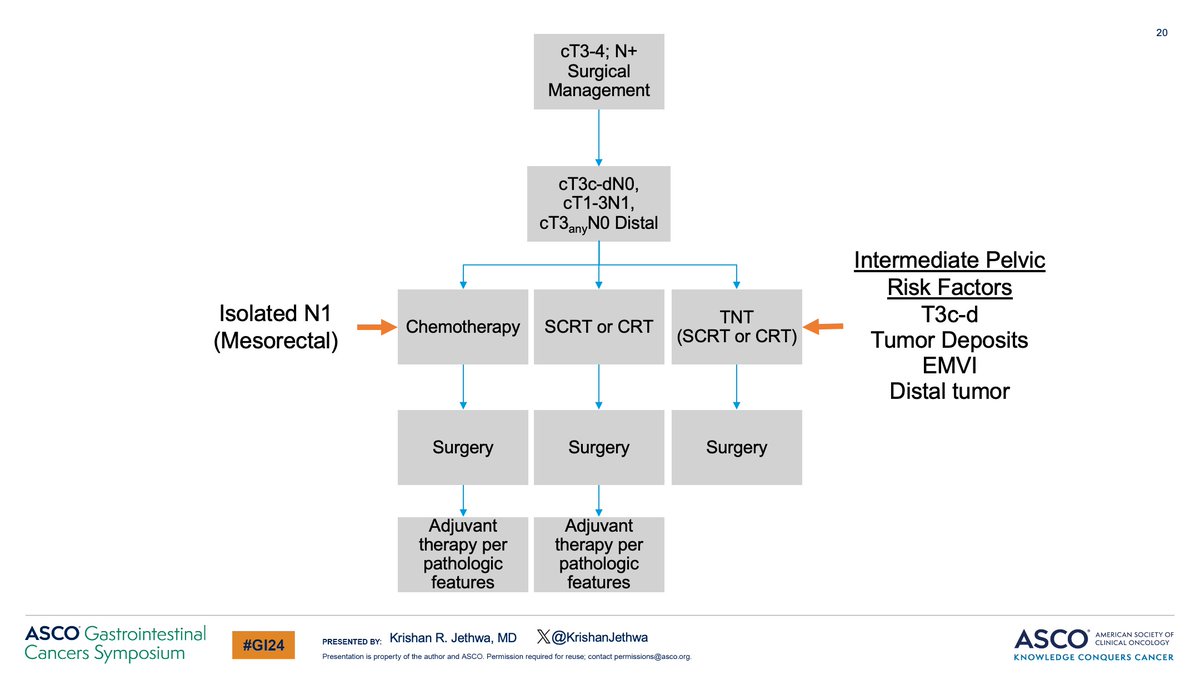
The intermediate risk cohort is much more nuanced!
🟡 Isolated N1, limited to mesorectum
➡️ Consider pre-operative chemotherapy with omission of RT
🟠 Additional pelvic risk factors (T3c-d, tumor deposits, EMVI, distal tumor)
➡️ Favor addition of RT
12/
🟡 Isolated N1, limited to mesorectum
➡️ Consider pre-operative chemotherapy with omission of RT
🟠 Additional pelvic risk factors (T3c-d, tumor deposits, EMVI, distal tumor)
➡️ Favor addition of RT
12/
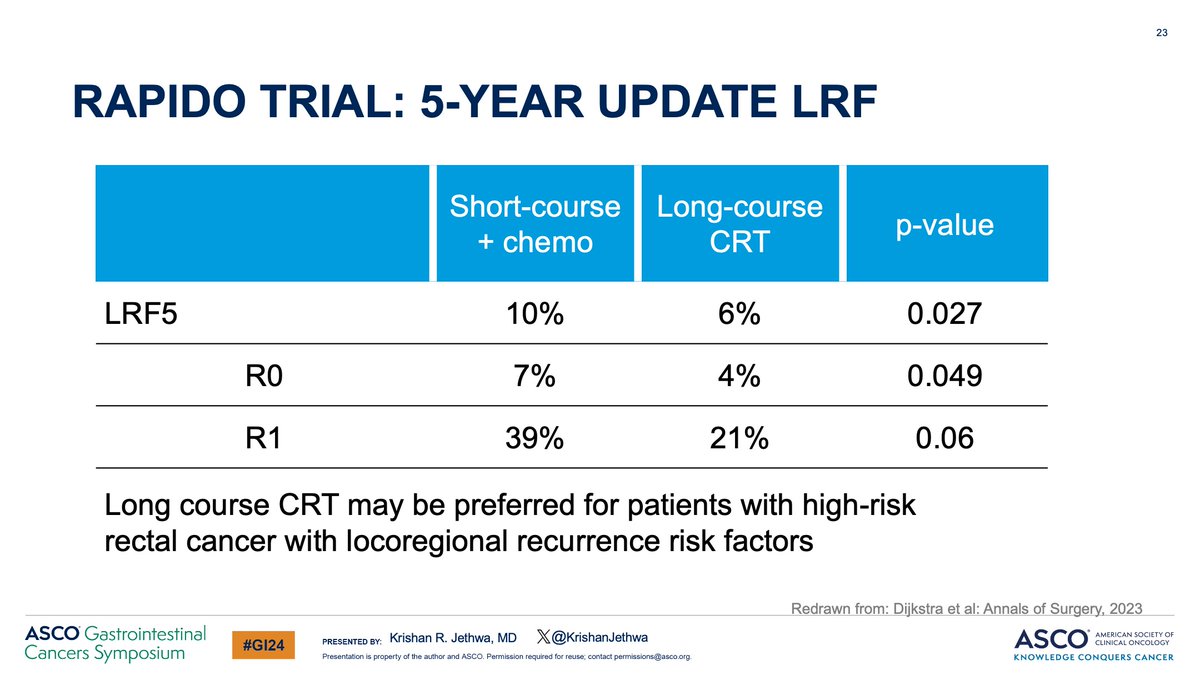
Let’s discuss SC-RT vs. LC-CRT
SCRT= similar LC, DFS, OS in prior studies of “average risk” patients.
🔥RAPIDO= high risk: ⬆️ pelvic recurrence (10% vs. 6%) with SC-TNT vs. LC-CRT.
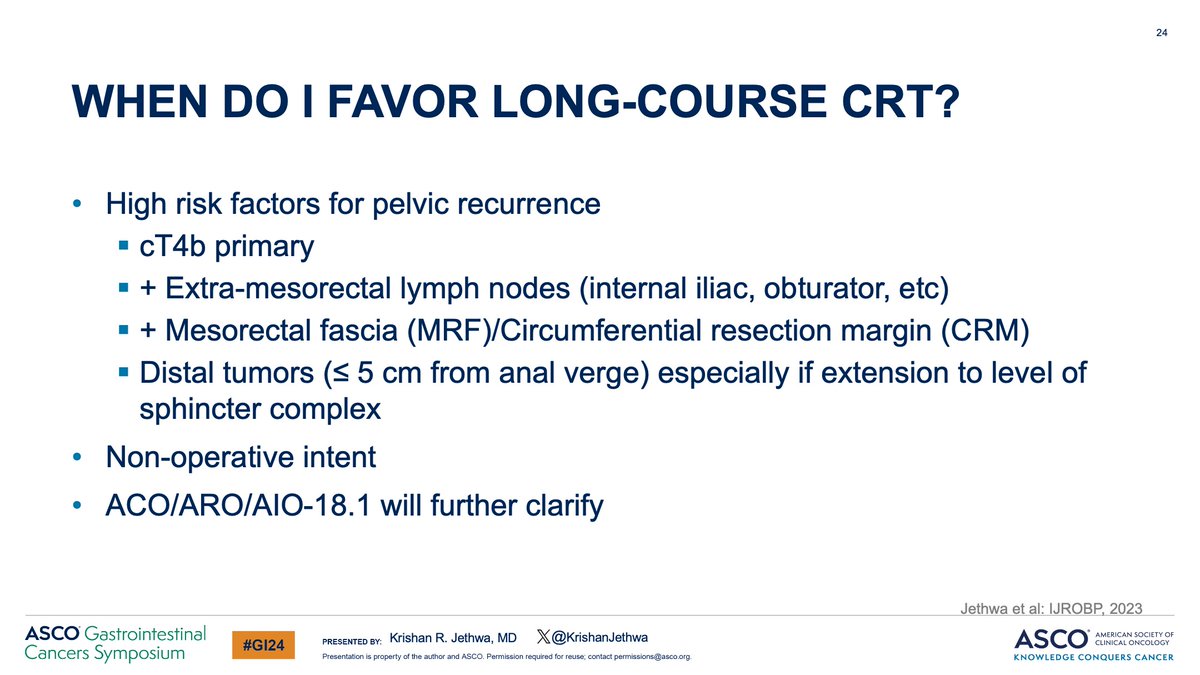
LC-CRT may be preferred for patients with high-risk rectal cancer
13/
SCRT= similar LC, DFS, OS in prior studies of “average risk” patients.
🔥RAPIDO= high risk: ⬆️ pelvic recurrence (10% vs. 6%) with SC-TNT vs. LC-CRT.
LC-CRT may be preferred for patients with high-risk rectal cancer
13/

Organ preservation❓❓
Goal= Preserve QoL and Function
LAR resulting in a low/coloanal anastomosis associated with poor bowel function
RT + Surgery is associated with poorer function
🔴Bowel
🔴Bladder
🔴Sexual
✅ Omission of surgery may better preserve function
14/
Goal= Preserve QoL and Function
LAR resulting in a low/coloanal anastomosis associated with poor bowel function
RT + Surgery is associated with poorer function
🔴Bowel
🔴Bladder
🔴Sexual
✅ Omission of surgery may better preserve function
14/
Let's review sequence of therapy!!
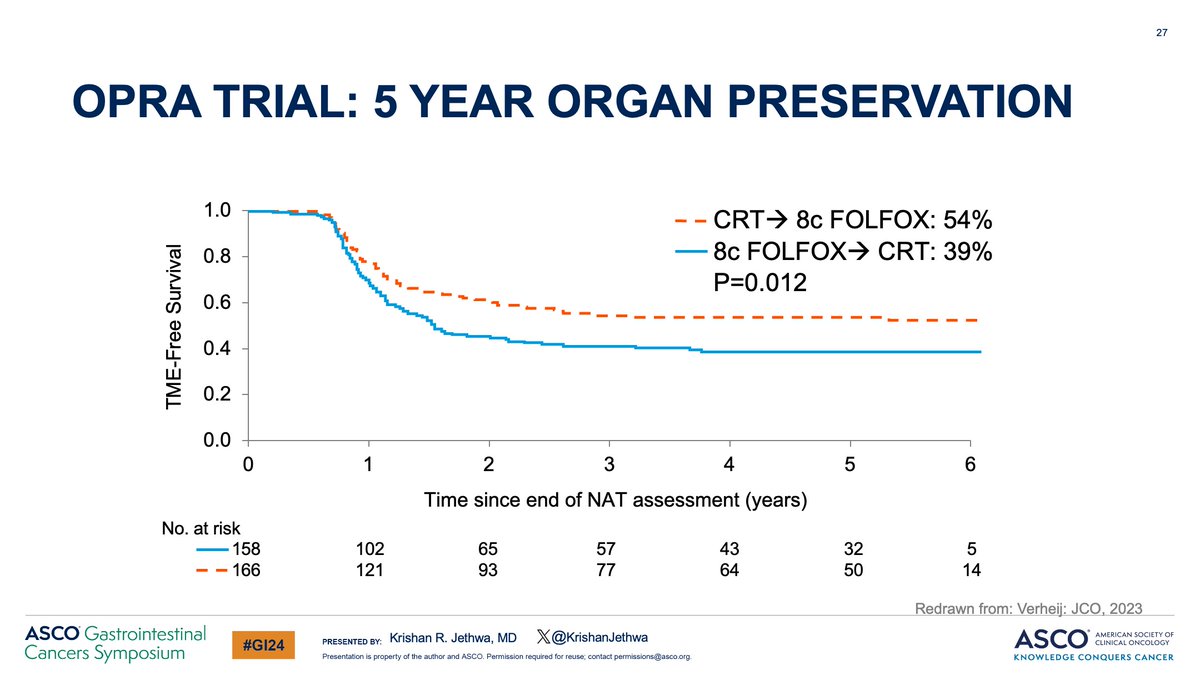
OPRA: ~50% may achieve long term organ preservation‼️
CRT ➡️chemo sequence vs. chemo ➡️ CRT:
✅⬇️ local regrowth and
✅⬆️ organ preservation with CRT➡️chemo
✅No difference in DFS or DFS after TME (initial iCR or regrowth)
15/
OPRA: ~50% may achieve long term organ preservation‼️
CRT ➡️chemo sequence vs. chemo ➡️ CRT:
✅⬇️ local regrowth and
✅⬆️ organ preservation with CRT➡️chemo
✅No difference in DFS or DFS after TME (initial iCR or regrowth)
15/

How can we improve cCR and organ preservation❓
RT perspective:
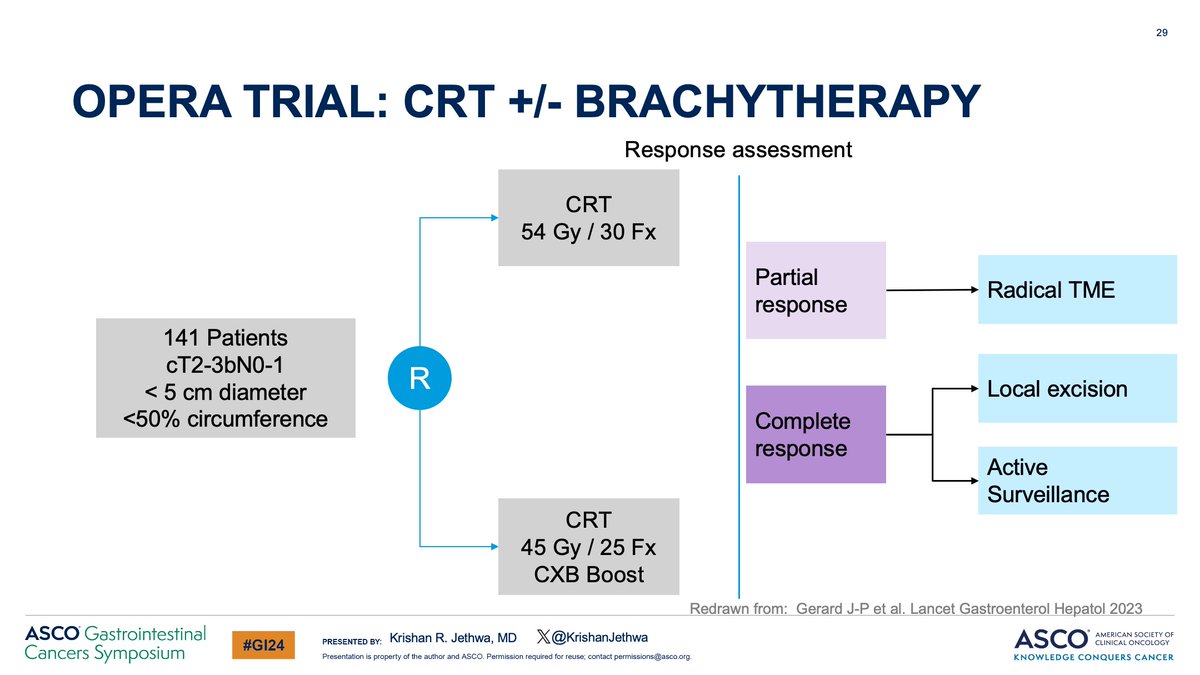
OPERA Trial
54 Gy/30 Fx CRT
vs.
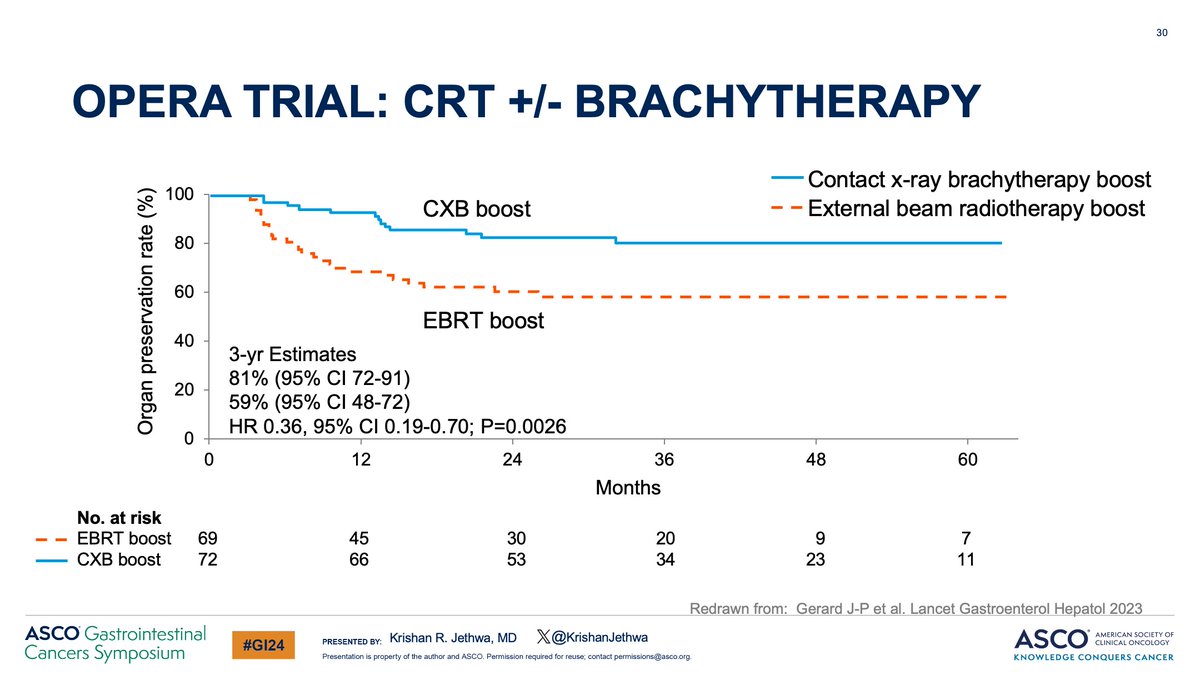
45 Gy/25 Fx CRT + Brachy boost (90 Gy/3 Fx)
✅Brachy= 3-year organ preservation: 81% vs. 59%
✅No detriment in severe toxicity or function!
Supports RT dose intensification‼️
16/
RT perspective:
OPERA Trial
54 Gy/30 Fx CRT
vs.
45 Gy/25 Fx CRT + Brachy boost (90 Gy/3 Fx)
✅Brachy= 3-year organ preservation: 81% vs. 59%
✅No detriment in severe toxicity or function!
Supports RT dose intensification‼️
16/
Key conclusions‼️
🔵 RT may be omitted in patients with MRI defined- favorable risk disease
🔵 TNT preferred for high risk disease
🔵 Organ preservation better preserves QoL and function
🔵CRT➡️chemo sequence preferred for NOM
🚨 LARC Algorithm here!
👆🏽 For discussion!
17/17
🔵 RT may be omitted in patients with MRI defined- favorable risk disease
🔵 TNT preferred for high risk disease
🔵 Organ preservation better preserves QoL and function
🔵CRT➡️chemo sequence preferred for NOM
🚨 LARC Algorithm here!
👆🏽 For discussion!
17/17
Loading suggestions...