

1/10
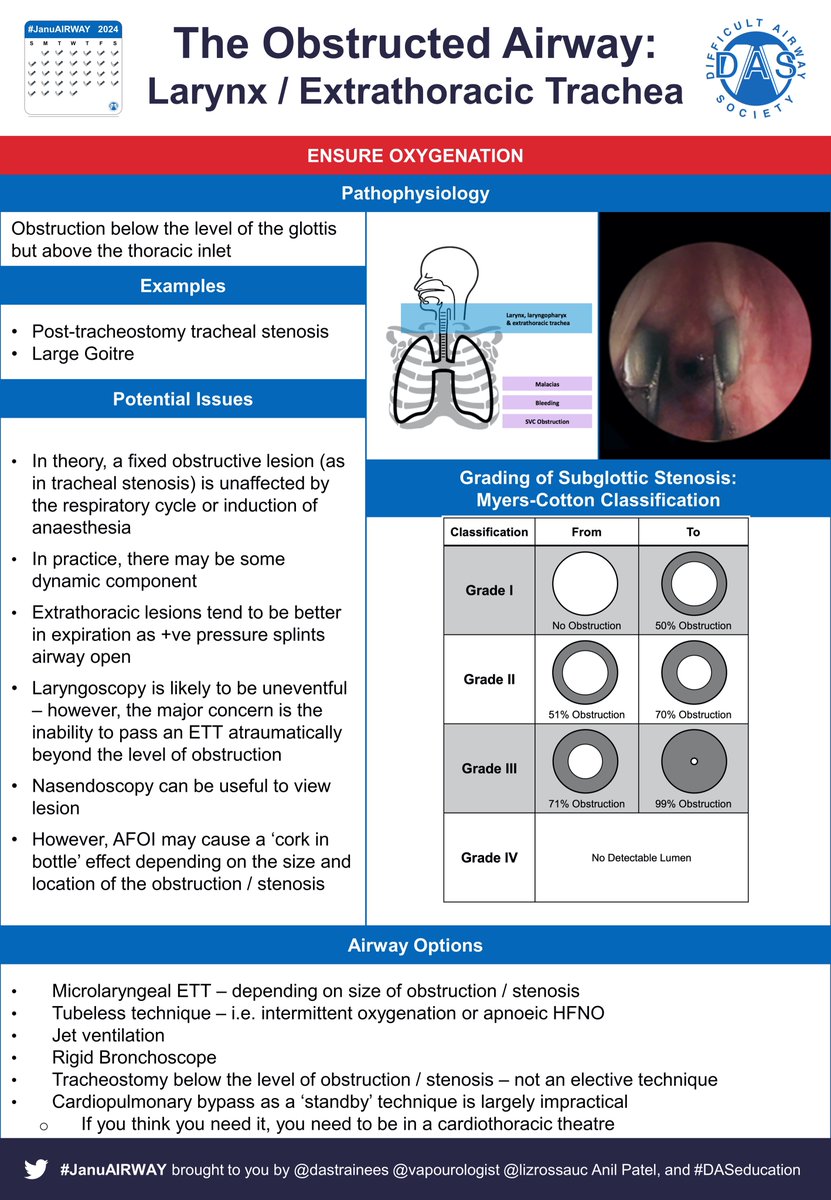

- Theory=fixed lesion unaffected by respiratory cycle / anaesthesia induction (but most have a dynamic element)
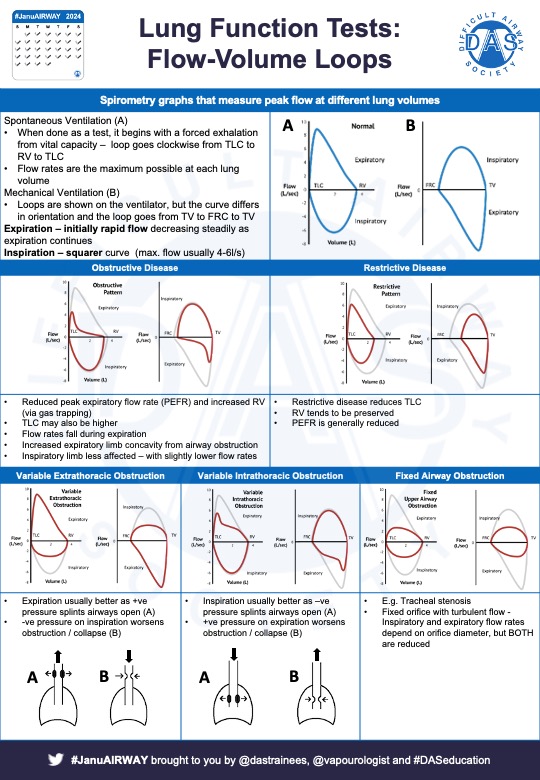
- Extrathoracic lesions usually better in expiration +ve pressure splints airway open
- Flow-volume loops can be helpful
#JanuAIRWAY 2/10
- Laryngoscopy likely to be easy – however, major concern = inability to pass ETT atraumatically beyond the level of obstruction
- Nasendoscopy can be useful to view lesion
- AFOI may cause ‘cork in bottle’ effect depending on lesion size/location
#JanuAIRWAY 3/10
ncbi.nlm.nih.gov
bjanaesthesia.org.uk associationofanaesthetists-publications.onlinelibrary.wiley.com
ajol.info
ispub.com
tandfonline.com
#JanuAIRWAY 4/10

Acute infective airway obstruction associated with subglottic stenosis
Pre-existing subglottic stenosis in a 22-month-old child with laryngotracheobronchitis resulted in f...
Internet Scientific Publications
Use your account on the social network Facebook, to create a profile on BusinessPress

Anaesthesia and subglottic airway obstruction
In this article, we describe the anaesthetic management and laser excision of a subglottic tumour th...

Subglottic stenosis in pregnancy
Subglottic stenosis (SGS) in pregnancy is rare but may cause a potentially life-threatening delivery...
Anaesthesia and subglottic airway obstruction
In this article, we describe the anaesthetic management and laser excision of a subglottic tumour th...

A multidisciplinary approach for managing the infraglottic difficult airway in the setting of the Coronavirus pandemic
Management of a difficult airway caused by pathology below the glottis is high-risk and requires a s...
- Upper/Mid lesions usually low risk – ETT may pass beyond
- Low tracheal/Bronchial lesions = high risk, best managed in specialist centres
- CT scan = essential
- Sudden obstruction can occur at ANY time
- Potential compression of heart/vessels
- 5/10
- Check position patient breaths best in
- Spont vent may help, IPPV may cause airway collapse
- Opinion re: IV vs inhalational = mixed
- Ketamine ?preserves chest wall tone
- Need back up plan
- Consider Heliox/bypass/ECMO before starting
#JanuAIRWAY 6/10
In an emergency – consider passing an ETT tube & then placing a jet catheter (e.g. Cook or Aintree) beyond obstruction.
Alternatively, an extra-long ETT can be created by cutting reinforced ETT & inserting into the free end of another
#JanuAIRWAY 7/10
- ATI/AFOI – view level of obstruction & try to pass ETT beyond before induction
- Rigid bronchoscope
- Jet vent.
- Cardiopulmonary bypass as ‘standby’ technique is often impractical - if you think you need it, need to be in a cardiothoracic theatre
#JanuAIRWAY 8/10
atsjournals.org
bmcresnotes.biomedcentral.com
jtd.amegroups.com ncbi.nlm.nih.gov
pubs.asahq.org
academic.oup.com
#JanuAIRWAY 9/10

Case Scenario: Perioperative Airway Management of a Patient with Tracheal Stenosis
TRACHEAL stenosis is a rare but a life-threatening condition and is caused by congenital problems, p...

Practical anesthetic considerations in patients undergoing tracheobronchial surgeries: a clinical review of current literature
Practical anesthetic considerations in patients undergoing tracheobronchial surgeries: a clinical re...

Stay in the Loop!
A 79-year-old man developed cough and rapidly progressive dyspnea. Physical examination featured acc...

Management of the patient with a central airway obstruction
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not im...

Airway stents: anaesthetic implications
Interventional management of airway lesions occluding the tracheobronchial tree include argon plasma...

The saw-tooth sign as a clinical clue for intrathoracic central airway obstruction - BMC Research Notes
Background The saw-tooth sign was first described by Sanders et al in patients with obstructive slee...
Loading suggestions...