



3/10
Answer (IMO)= PA rupture, massive hemoptysis, death.
INPT numbers of PA rupture d/t #PAC:
Largest (retrospective) report looked at 32,442 #PACs.
Single institution (OR/ICU), 17-year span.
Findings:
*0.03% PA rupture rate (10 cases)
*70% mortality journal.chestnet.org
Answer (IMO)= PA rupture, massive hemoptysis, death.
INPT numbers of PA rupture d/t #PAC:
Largest (retrospective) report looked at 32,442 #PACs.
Single institution (OR/ICU), 17-year span.
Findings:
*0.03% PA rupture rate (10 cases)
*70% mortality journal.chestnet.org
4/10
OUTPATIENT (cath lab) numbers for #PAC pulmonary hypertension (PH) cases
Multi PH center, 5.727 #PAC procedures.
Findings:
*0.05% fatal events (4 cases). *Only 1 related to PA rupture
sciencedirect.com
OUTPATIENT (cath lab) numbers for #PAC pulmonary hypertension (PH) cases
Multi PH center, 5.727 #PAC procedures.
Findings:
*0.05% fatal events (4 cases). *Only 1 related to PA rupture
sciencedirect.com

5/10
Back to the case.
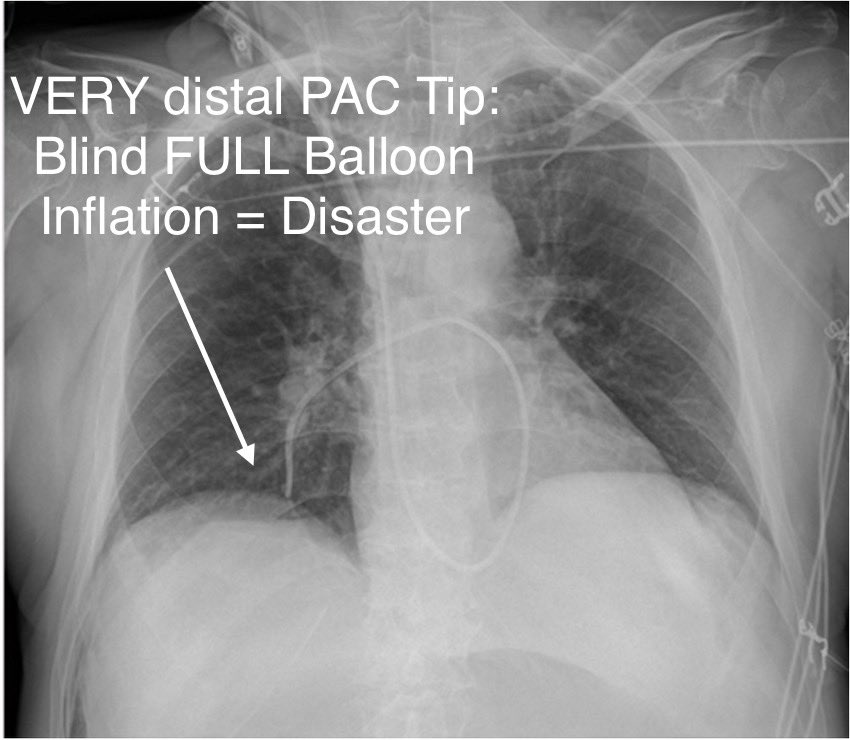
PA rupture risk likely much higher when #PAC balloon is advanced/inflated blindly (vs fluoroscopy-guided)
What could you have done differently to prevent a PA rupture complication?
8 KEY POINTS about balloon inflation (what I do; others may differ): 👇🏻
Back to the case.
PA rupture risk likely much higher when #PAC balloon is advanced/inflated blindly (vs fluoroscopy-guided)
What could you have done differently to prevent a PA rupture complication?
8 KEY POINTS about balloon inflation (what I do; others may differ): 👇🏻
7/10
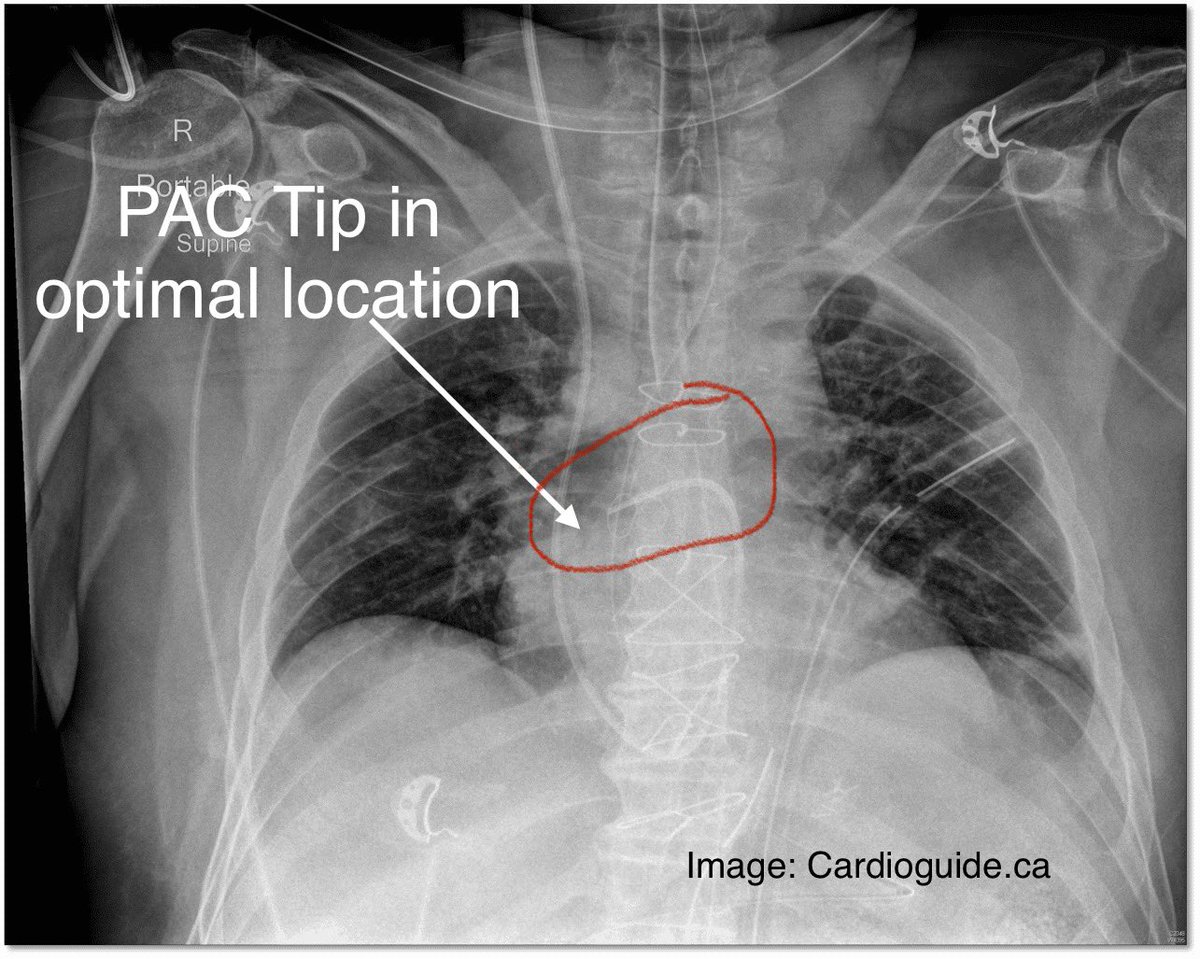
5. CXR: Tip ✅ location but poor WF, gently flush PAC tip
6. PA WF present: inflate balloon 0.1-0.2 cc x sec (my routine). Once “wedged” STOP inflating
7. Lock balloon, measure wedge. Then deflate, remove all air
8. Rule: “wedge” < 30-60 secs (⬇️ pulm infarction risk)
5. CXR: Tip ✅ location but poor WF, gently flush PAC tip
6. PA WF present: inflate balloon 0.1-0.2 cc x sec (my routine). Once “wedged” STOP inflating
7. Lock balloon, measure wedge. Then deflate, remove all air
8. Rule: “wedge” < 30-60 secs (⬇️ pulm infarction risk)
8/10
Balloon Inflation “PEARLS”
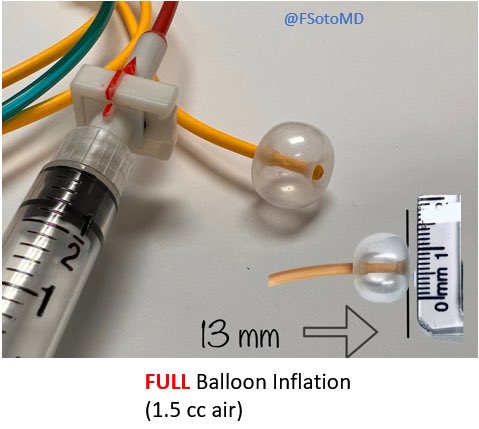
1st: based on how distal PAC tip is, you only need a small amount of air to occlude the vessel.
Pictures below illustrate smaller balloon volumes, just enough for distal or narrowed/diseased vessels.
PAC shown: Edwards Lifesciences Swan-Ganz.
Balloon Inflation “PEARLS”
1st: based on how distal PAC tip is, you only need a small amount of air to occlude the vessel.
Pictures below illustrate smaller balloon volumes, just enough for distal or narrowed/diseased vessels.
PAC shown: Edwards Lifesciences Swan-Ganz.



9/10
2nd: video👇🏻 shows dynamic balloon inflation.
After ~ 0.8cc (of 1.5 cc) rapid inflation occurs
When inflating, I look at the monitor (and not the syringe)
I inflate 0.1-0.2 cc x sec and STOP once “wedge” WF appears
2nd: video👇🏻 shows dynamic balloon inflation.
After ~ 0.8cc (of 1.5 cc) rapid inflation occurs
When inflating, I look at the monitor (and not the syringe)
I inflate 0.1-0.2 cc x sec and STOP once “wedge” WF appears

10/10
Video 👇🏻 illustrates a “slow but steady” balloon inflation until “wedge” WF appears (ICU setting)
DO NOT add additional air unless there is a specific need to cause additional occlusion (i.e., if WF suggests partial wedge WF).
Video 👇🏻 illustrates a “slow but steady” balloon inflation until “wedge” WF appears (ICU setting)
DO NOT add additional air unless there is a specific need to cause additional occlusion (i.e., if WF suggests partial wedge WF).

Finally, you may either love or hate #PAC
Even if you “despise” it, you may still take care of pts with one in place.
Learning how to troubleshoot it and avoiding PAC-related complications is still vital.
Pinging #PAC gurus @RyanTedfordMD @msiuba for additional thread wisdom
Even if you “despise” it, you may still take care of pts with one in place.
Learning how to troubleshoot it and avoiding PAC-related complications is still vital.
Pinging #PAC gurus @RyanTedfordMD @msiuba for additional thread wisdom
Found this thread helpful?
Retweet the 1st tweet to help someone else.
Coming up threads:
1. #PAC: basic components and functions
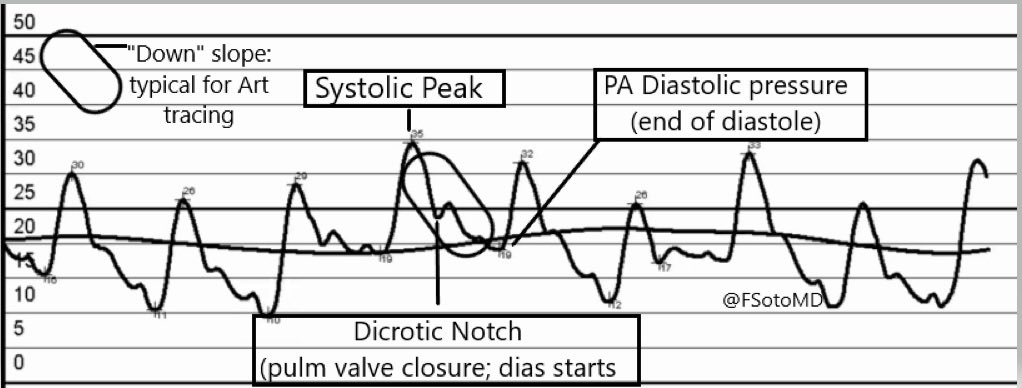
2. Proper waveform recognition
3. How to measure the pressures on the bedside monitor
4. How to manage (hopefully) a PA catheter rupture
Retweet the 1st tweet to help someone else.
Coming up threads:
1. #PAC: basic components and functions
2. Proper waveform recognition
3. How to measure the pressures on the bedside monitor
4. How to manage (hopefully) a PA catheter rupture
Loading suggestions...