

#JanuAirway Day 4. Gastric Ultrasound #POCUS or #HOCUM? Maybe these #OnePagers can convince you it’s no joke? Thanks to the legendary @elboghdadly for his help on this one! 1/12
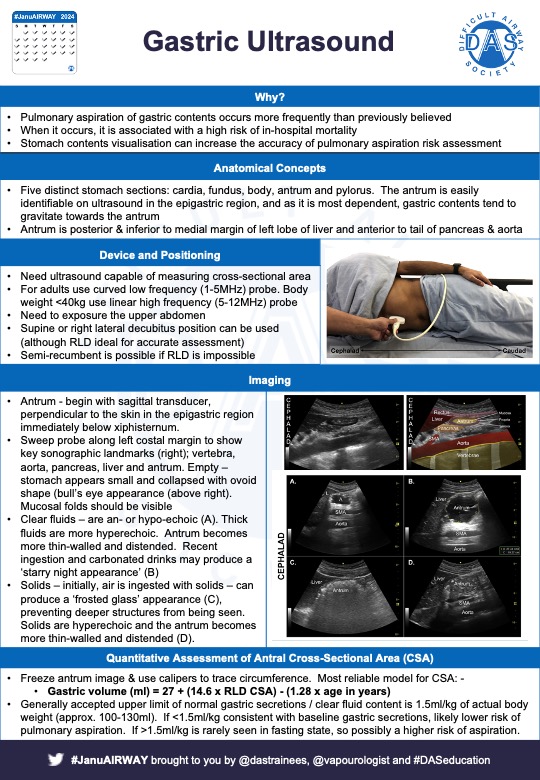
#JanuAirway Why do gastric ultrasound? The main reason is that pulmonary aspiration of gastric contents is more frequent than previously thought (1 in 2000-3000 elective GAs), and is a major risk factor for in-hospital mortality 2/12
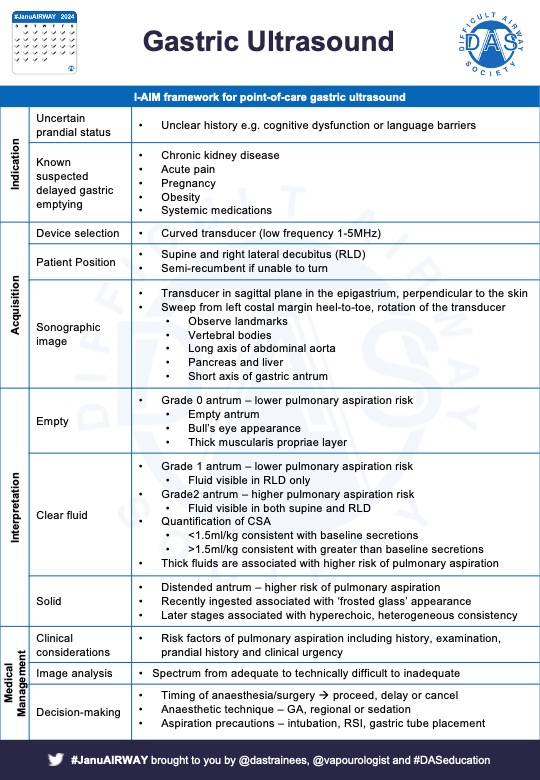
#JanuAirway If prandial status is unknown or there’s known/suspected delayed gastric emptying (e.g. medication, chronic kidney disease, etc), gastric ultrasound can be helpful in assessing aspiration risk 3/12
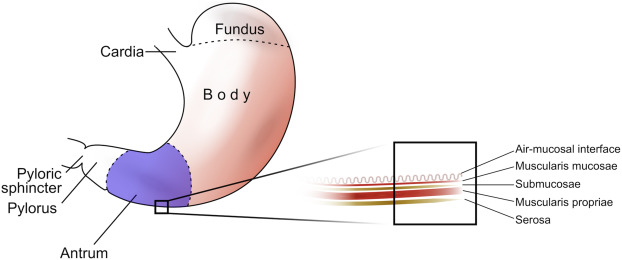
#JanuAirway The stomach has 5 distinct sections; cardiac, fundus, body, antrum and pylorus. The antrum is what we’re interested in in Gastric USS. It’s easily identifiable and a dependent area so contents gravitate towards it. There are 5 antral layers 4/12
#JanuAirway Probe – low frequency & curved. Positioning – can be supine (easier to visualise) or right lateral decubitus (harder to visualise, but more sensitive for smaller volumes. But remember some patients won’t be able to lie laterally. 5/12
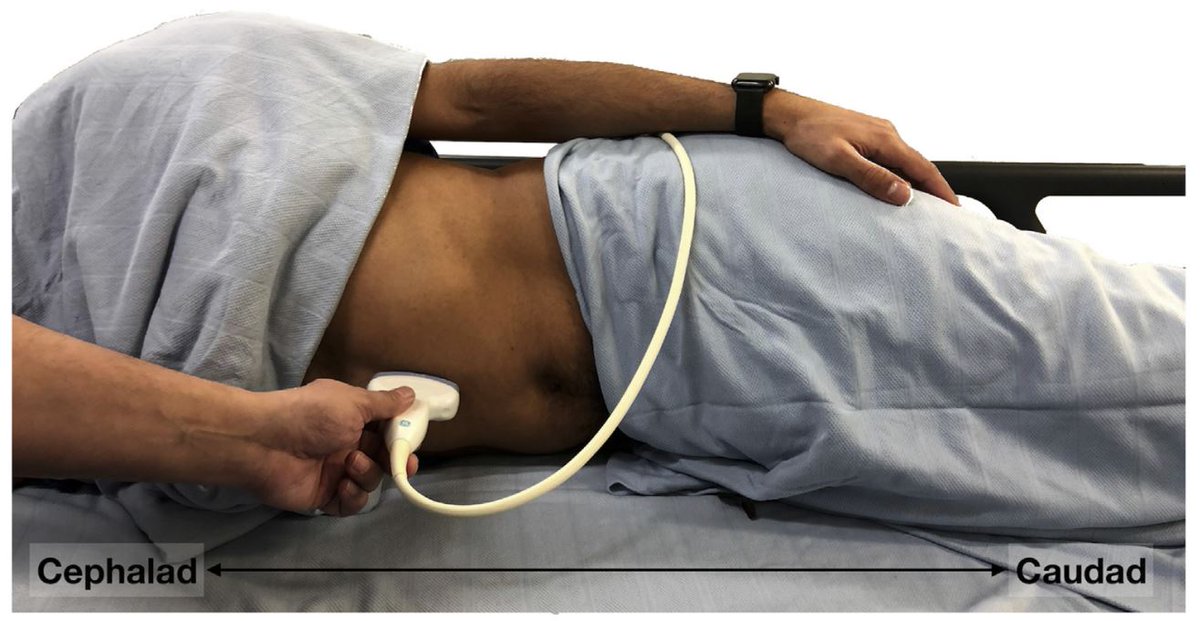
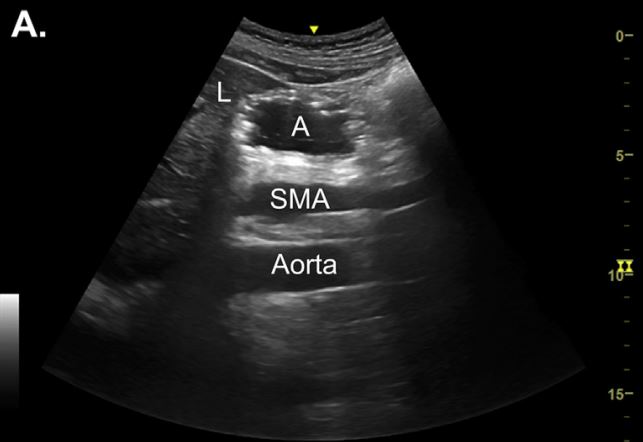
#JanuAirway Apply probe perpendicular to skin (sagittal plane) in epigastric region below the xiphisternum – then sweep from left costal margin looking for vertebral bodies, long axis of abdominal aorta, head/neck of pancreas, inf margin of left liver lobe & gastric antrum 6/12
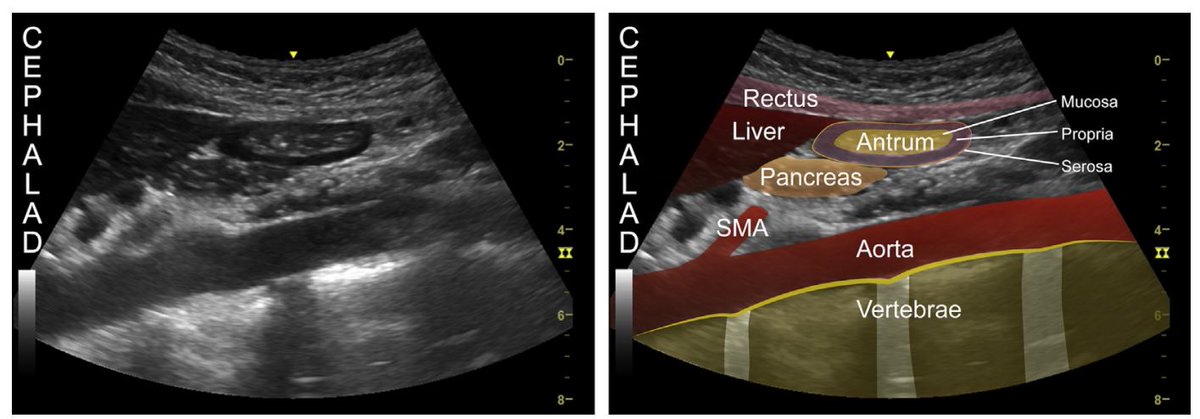
#JanuAirway The stomach will have thick hypoechoic muscularis and hyperechoic serosa and mucosal layers (~4mm thick) and be relatively superficial . If empty – stomach appears small, flat and collapsed
#FOAMed 7/12
#FOAMed 7/12
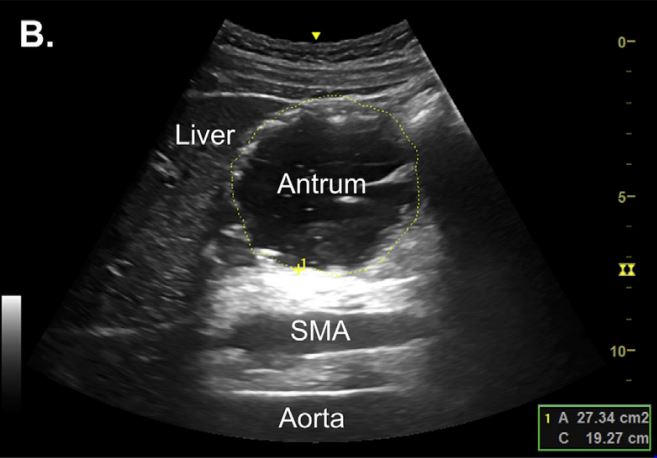
#JanuAirway Clear fluids are anechoic or hypoechoic, thick fluids like milk appear more echoic but homogenous and the antrum will appear distended with thinner walls. Carbonated drinks can show bubbles – ‘starry night’ appearance
#FOAMed 8/12
#FOAMed 8/12
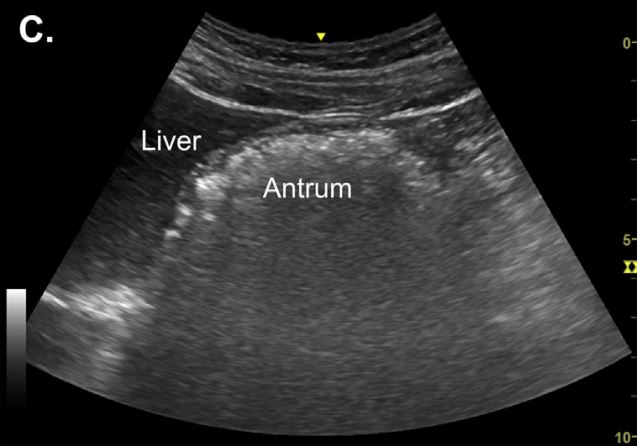
#JanuAirway Solids – eating results in swallow of air as well as food. Air causes ‘frosted glass’ appearance and stops visualisation of deeper structures. Contents are hyperechoic and heterogenous. Peristalsis may be seen
#FOAMed 9/12
#FOAMed 9/12
#JanuAirway Quantitative assessment – generally accepted upper limit of normal secretions = 1.5ml/kg of actual body wt. <1.5ml/kg suggests lower risk, >1.5mk/kg higher risk. Formula for calculation is Gastric vol (ml) = 27 + (14.6 X RLD CSA) – (1.28 x age in years) 10/12
Here are some papers / links that you might find interesting: -
· bjaed.org
·sciencedirect.com
· link.springer.com
If you have any others of interest, tweet them to us for inclusion next time!
#JanuAirway 11/12
· bjaed.org
·sciencedirect.com
· link.springer.com
If you have any others of interest, tweet them to us for inclusion next time!
#JanuAirway 11/12
link.springer.com/article/10.100…

sciencedirect.com/science/articl…
Ultrasound assessment of gastric content and volume
Pulmonary aspiration of gastric content is a serious anaesthetic complication that can lead to signi...
bjaed.org/article/S2058-…
Perioperative point-of-care gastric ultrasound
Pulmonary aspiration of gastric contents occurs once every 2000–3000 elective general anaesthetics a...
Hope that helps. We’ll see you tomorrow for more Airway #FOAMed. See you then! #JanuAirway 12/12
*Disclaimer: Inclusion of content (equipment, techniques and scoring systems etc.) in #JanuAIRWAY does not constitute DAS endorsement
*Disclaimer: Inclusion of content (equipment, techniques and scoring systems etc.) in #JanuAIRWAY does not constitute DAS endorsement
Loading suggestions...