

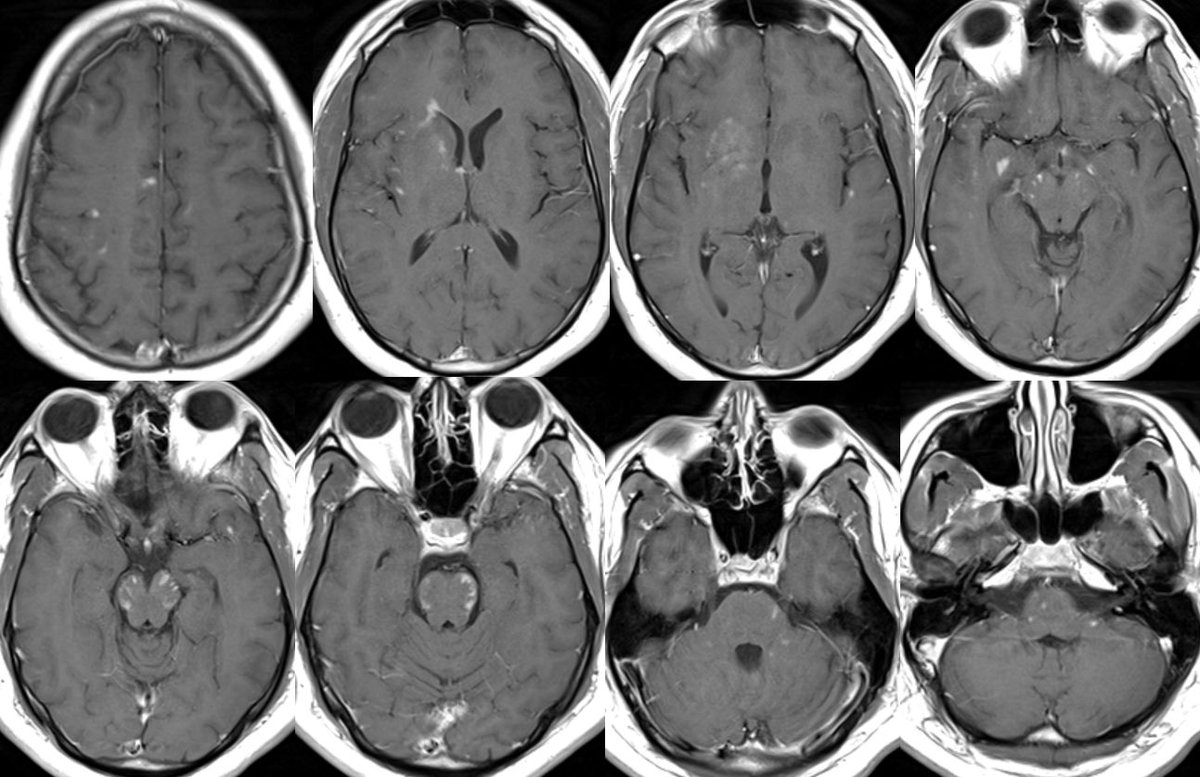
What is the most likely diagnosis in this 30 y/o M presenting w/ a few weeks of headaches, photophobia, vision loss, confusion, and ataxia?
More images in 🧵
#Neurology #Neurosurgery #radres #futureradres #MedEd #medicine @AlbanyMedRadRes
More images in 🧵
#Neurology #Neurosurgery #radres #futureradres #MedEd #medicine @AlbanyMedRadRes



More images



Answer: MOG antibody-associated disease (MOG-AAD)
Path: MOG-AAD is an autoimmune inflammatory demyelinating disease targeting oligodendrocytes (NMO targets AQP4)
Path: MOG-AAD is an autoimmune inflammatory demyelinating disease targeting oligodendrocytes (NMO targets AQP4)
Epidemiology:
▶️MOG-AAB: No significant gender predilection ▶️NMO: Strong FEMALE predilection (~8-9:1)
▶️MOG-AAD: Typically affects children and young adults
▶️NMO: Has a slightly older average age (~40 w/ about 15-20% occurring over 60 years)
▶️MOG-AAB: No significant gender predilection ▶️NMO: Strong FEMALE predilection (~8-9:1)
▶️MOG-AAD: Typically affects children and young adults
▶️NMO: Has a slightly older average age (~40 w/ about 15-20% occurring over 60 years)
Clinical (please add clinical pearls 🙏):
▶️Most common symptoms are impaired or double vision
▶️An infectious prodrome frequently precedes initial symptom onset in MOG-AAD (~60% of cases vs <10% in NMO)
▶️MOG-AAD is more likely monophasic with fewer relapses compared to NMO
▶️Most common symptoms are impaired or double vision
▶️An infectious prodrome frequently precedes initial symptom onset in MOG-AAD (~60% of cases vs <10% in NMO)
▶️MOG-AAD is more likely monophasic with fewer relapses compared to NMO
Typical Imaging of MOG-AAD:
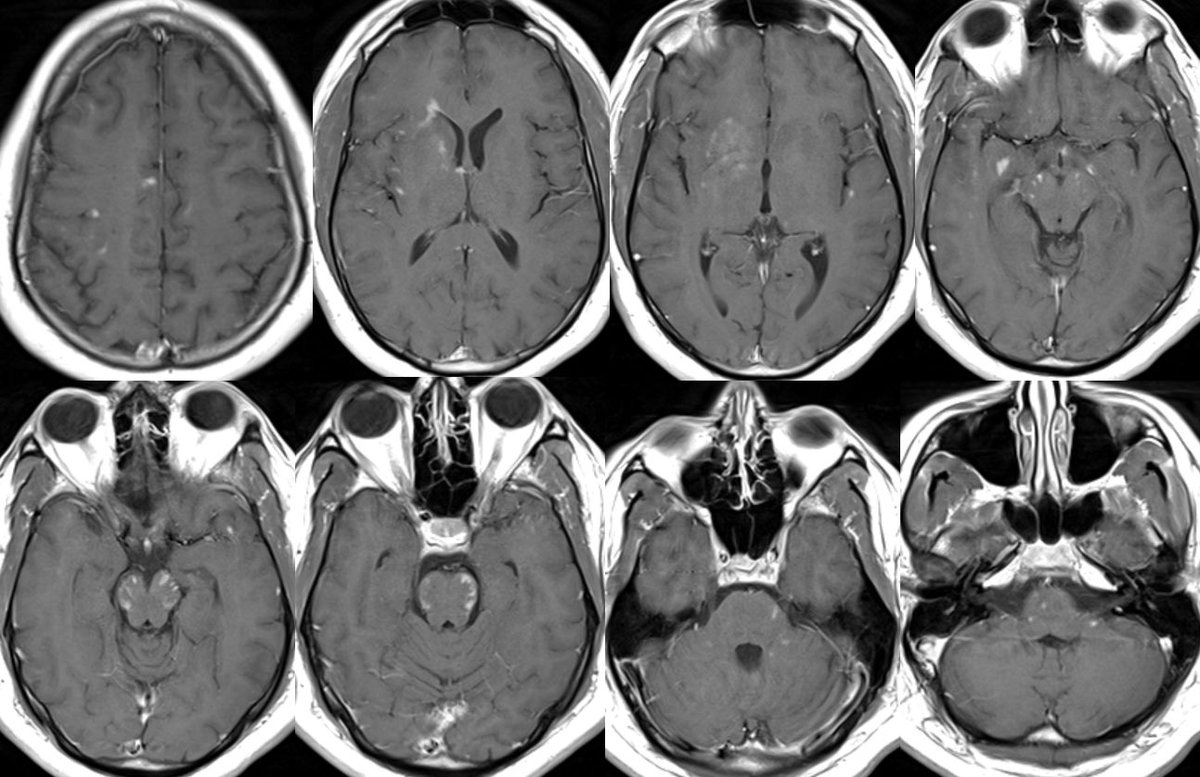
▶️OPTIC NERVES: Long segment BILATERAL edematous & tortuous optic nerves predominantly involving the ANTERIOR nerves (there was patchy involvement of the chiasm and tracts in this case but the predominant involvement was anterior)
▶️OPTIC NERVES: Long segment BILATERAL edematous & tortuous optic nerves predominantly involving the ANTERIOR nerves (there was patchy involvement of the chiasm and tracts in this case but the predominant involvement was anterior)


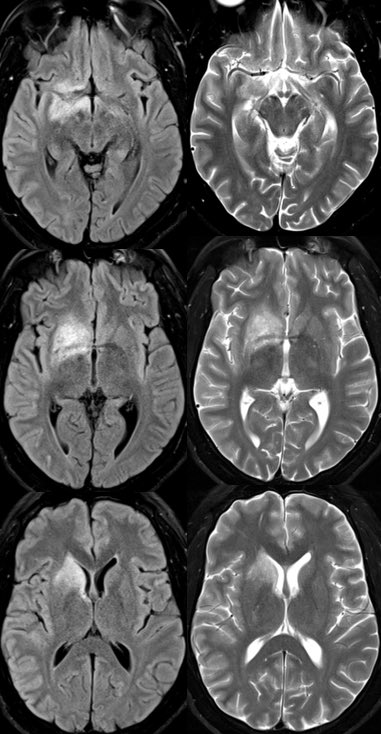
▶️BRAIN findings: Occur in <50% of patients though tend to involve the deep gray matter and infratentorium (particularly in children)
▶️Patterns include ADEM-like or CLIPPERS-like imaging features
▶️Leptomeningeal enhancement can also be seen in association with FLAMES
▶️Patterns include ADEM-like or CLIPPERS-like imaging features
▶️Leptomeningeal enhancement can also be seen in association with FLAMES
▶️SPINE findings: preferentially affects the lower cord, particularly the conus
▶️Patterns may be longitudinally extensive or short segment
▶️Spinal gray matter involvement can appear as thin linear T2 signal abnormality on sagittal or appear as on H on axial “H sign”
▶️Patterns may be longitudinally extensive or short segment
▶️Spinal gray matter involvement can appear as thin linear T2 signal abnormality on sagittal or appear as on H on axial “H sign”
💡 The thoracic cord is very prone to artifacts (pretty much every spine I read, I can hallucinate thoracic cord signal abnormality) so make sure the lesion you are calling can be confirmed in multiple planes and fits clinically otherwise it may be artifactual
💡 The conus can also commonly be affected in cord infarcts due to poor collateral supply after occlusion of the artery of Ademkiewicz (I’ve seen people misdiagnosis cord infarcts as MOG-AAD because of conus swelling)
Typical imaging of NMO:
▶️ AQP4 is abundantly expressed in the optic nerves, spinal cord, periventricular areas, hypothalamus, brainstem, and area postrema (keep this in mind for the imaging findings)
▶️ AQP4 is abundantly expressed in the optic nerves, spinal cord, periventricular areas, hypothalamus, brainstem, and area postrema (keep this in mind for the imaging findings)
▶️OPTIC NERVES: Bilateral long segment optic neuritis which tends to extend more posterior involving the optic chiasm and tracts
▶️BRAIN findings: Periventricular FLAIR signal abnormalities which may surround the lateral, 3rd, and/or 4th ventricle as well as the cerebral aqueduct
▶️BRAIN findings: Periventricular FLAIR signal abnormalities which may surround the lateral, 3rd, and/or 4th ventricle as well as the cerebral aqueduct
▶️Lesions may also involve the corticospinal tracts or can be tumefactive
▶️May see “cloud-like” enhancement or “pencil thin” periependymal or nodular enhancement
▶️SPINE findings: Longitudinally extensive cord involvement and more commonly involves the cervicomedullary junction
▶️May see “cloud-like” enhancement or “pencil thin” periependymal or nodular enhancement
▶️SPINE findings: Longitudinally extensive cord involvement and more commonly involves the cervicomedullary junction
Summary MOG vs NMO:
MOG-AAD:
1️⃣Younger w/ no gender predilection
2️⃣More likely to have viral prodrome and be monophasic
3️⃣ANTERIOR optic nerve involvement
4️⃣Brain findings occur in <50% and may be ADEM or CLIPPERS-like with typical involvement of deep gray and posterior fossa
MOG-AAD:
1️⃣Younger w/ no gender predilection
2️⃣More likely to have viral prodrome and be monophasic
3️⃣ANTERIOR optic nerve involvement
4️⃣Brain findings occur in <50% and may be ADEM or CLIPPERS-like with typical involvement of deep gray and posterior fossa
MOG-AAD summary cont’d:
5️⃣Spinal cord involvement tends is less often LETM and affects the lower thoracic cord and conus
NMO:
1️⃣Older with strong FEMALE predilection
2️⃣More likely to relapse and less likely to have viral prodrome
3️⃣POSTERIOR optic nerve involvement
5️⃣Spinal cord involvement tends is less often LETM and affects the lower thoracic cord and conus
NMO:
1️⃣Older with strong FEMALE predilection
2️⃣More likely to relapse and less likely to have viral prodrome
3️⃣POSTERIOR optic nerve involvement
NMO summary cont’d:
4️⃣Brain findings often mirror the distribution of AQP4 (periventricular, optic nerves, hypothalamus, spine)
5️⃣More likely to have LETM and affects the upper cord/cervicomedullary junction
For more reading 📚
ncbi.nlm.nih.gov
ajronline.org
4️⃣Brain findings often mirror the distribution of AQP4 (periventricular, optic nerves, hypothalamus, spine)
5️⃣More likely to have LETM and affects the upper cord/cervicomedullary junction
For more reading 📚
ncbi.nlm.nih.gov
ajronline.org

ncbi.nlm.nih.gov/pmc/articles/P…
MRI differences between MOG antibody disease and AQP4 NMOSD.
MOG antibody and AQP4 antibody seropositive diseases are immunological distinct subtypes of neuromye...
ajronline.org/doi/full/10.22…
MOGAD: How It Differs From and Resembles Other Neuroinflammatory Disorders | AJR
Myelin oligodendrocyte glycoprotein antibody–associated disease (MOGAD) is a distinct CNS inflammato...
جاري تحميل الاقتراحات...