

1/17
🤔Why don't we transfuse to a normal hemoglobin?
In many cases, we aim to restore values to the normal range. Potassium and other electrolytes. Even white blood cells.
But not hemoglobin.
In most situations, we accept >7g/dL, far less than normal. Why are we so tolerant?
🤔Why don't we transfuse to a normal hemoglobin?
In many cases, we aim to restore values to the normal range. Potassium and other electrolytes. Even white blood cells.
But not hemoglobin.
In most situations, we accept >7g/dL, far less than normal. Why are we so tolerant?
2/
The principal rationale for red blood cell transfusion is to increase the O₂-carrying capacity and therefore O₂ delivery to tissues.
As hemoglobin is lowered O₂ delivery decreases, assuming all else remains unchanged.
So giving blood makes sense.
The principal rationale for red blood cell transfusion is to increase the O₂-carrying capacity and therefore O₂ delivery to tissues.
As hemoglobin is lowered O₂ delivery decreases, assuming all else remains unchanged.
So giving blood makes sense.
3/
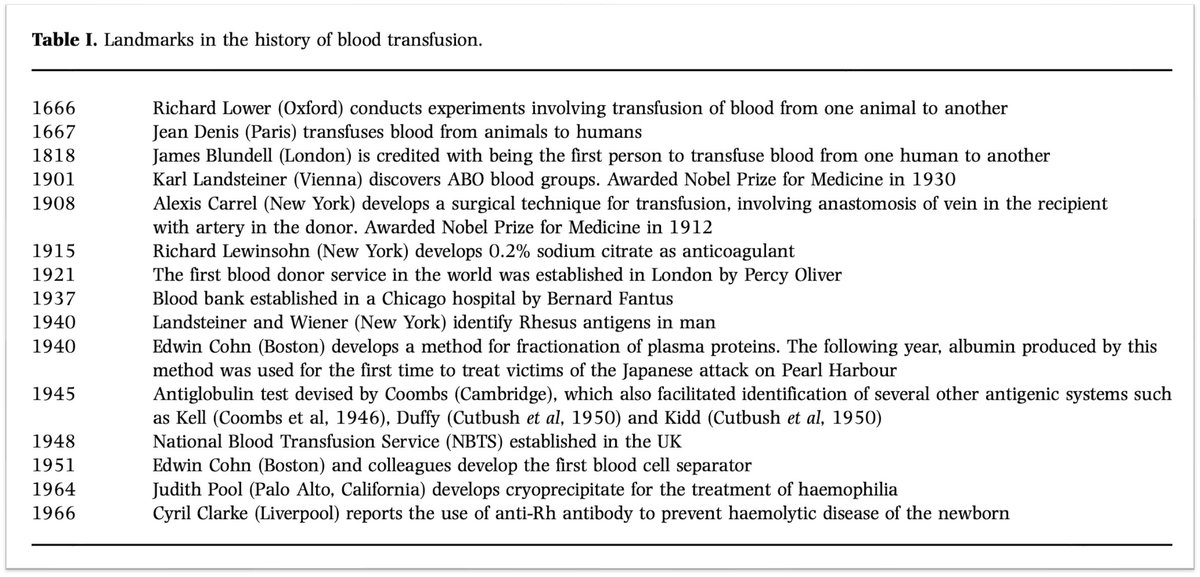
Historically we did not transfuse to normal because we did not transfuse. The risks far outstripped the benefits.
There were also technical constraints and storage limitations. This meant that transfusions were reserved for acute conditions.
onlinelibrary.wiley.com
Historically we did not transfuse to normal because we did not transfuse. The risks far outstripped the benefits.
There were also technical constraints and storage limitations. This meant that transfusions were reserved for acute conditions.
onlinelibrary.wiley.com
4/
By the mid-1900s most of the obstacles had been overcome. We now could store blood as individual components and more safely administer it.
And though scarcity remains an issue, it alone doesn't preclude our need to transfuse back to normal.
redcross.org
By the mid-1900s most of the obstacles had been overcome. We now could store blood as individual components and more safely administer it.
And though scarcity remains an issue, it alone doesn't preclude our need to transfuse back to normal.
redcross.org

5/
First, evolution has given us quite a bit of wiggle room when it comes to the tolerable hemoglobin value.
Why?
O₂ delivery >>>> O₂ consumption
This difference provides a reserve. Hemoglobin can decrease a lot before O₂ delivery no longer meets the demands of tissues.
First, evolution has given us quite a bit of wiggle room when it comes to the tolerable hemoglobin value.
Why?
O₂ delivery >>>> O₂ consumption
This difference provides a reserve. Hemoglobin can decrease a lot before O₂ delivery no longer meets the demands of tissues.
6/
How much reserve?
Animal studies have found the following values, at rest:
☞O₂ delivery: 20-30 mL O₂·kg⁻¹·min⁻¹
☞O₂ consumption: 6 mL O₂·kg⁻¹·min⁻¹
💡This difference shows that, at rest, we deliver far more O₂ than we need.
pubmed.ncbi.nlm.nih.gov
How much reserve?
Animal studies have found the following values, at rest:
☞O₂ delivery: 20-30 mL O₂·kg⁻¹·min⁻¹
☞O₂ consumption: 6 mL O₂·kg⁻¹·min⁻¹
💡This difference shows that, at rest, we deliver far more O₂ than we need.
pubmed.ncbi.nlm.nih.gov

7/
In addition to this reserve, the body compensates for the decreased O₂-carrying capacity seen in anemia. You see:
☞Increased O₂ delivery
☞Increased O₂ extraction
☞Blood flow redistribution to vital organs
thebloodproject.com
In addition to this reserve, the body compensates for the decreased O₂-carrying capacity seen in anemia. You see:
☞Increased O₂ delivery
☞Increased O₂ extraction
☞Blood flow redistribution to vital organs
thebloodproject.com
8/
Because hemorrhage also leads to volume depletion, it is hard to isolate the effect of anemia.
💡To address this, researchers perform studies of acute severe isovolemic anemia.
Blood is removed and an equal volume of fluid is given back.
onlinelibrary.wiley.com
Because hemorrhage also leads to volume depletion, it is hard to isolate the effect of anemia.
💡To address this, researchers perform studies of acute severe isovolemic anemia.
Blood is removed and an equal volume of fluid is given back.
onlinelibrary.wiley.com
9/
In one study, healthy subjects had 450-900 mL of blood removed to reduce their hemoglobin to 5.0 g/dL.
Isovolemia was maintained with 5% human albumin and/or plasma.
jamanetwork.com
In one study, healthy subjects had 450-900 mL of blood removed to reduce their hemoglobin to 5.0 g/dL.
Isovolemia was maintained with 5% human albumin and/or plasma.
jamanetwork.com
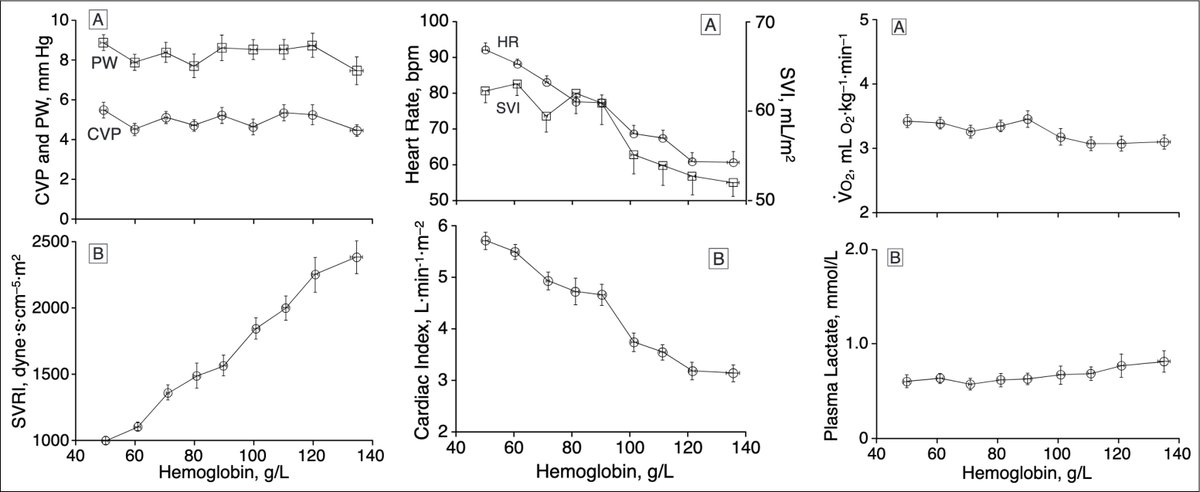
10/
Researchers reported the following:
↑heart rate, stroke volume, and cardiac index (CI)
↓systemic vascular resistance (SVR)
Lactate was unchanged.
O₂ consumption increased.
💡This suggests that O₂ delivery can be maintained, even at 5 g/dL.
jamanetwork.com
Researchers reported the following:
↑heart rate, stroke volume, and cardiac index (CI)
↓systemic vascular resistance (SVR)
Lactate was unchanged.
O₂ consumption increased.
💡This suggests that O₂ delivery can be maintained, even at 5 g/dL.
jamanetwork.com
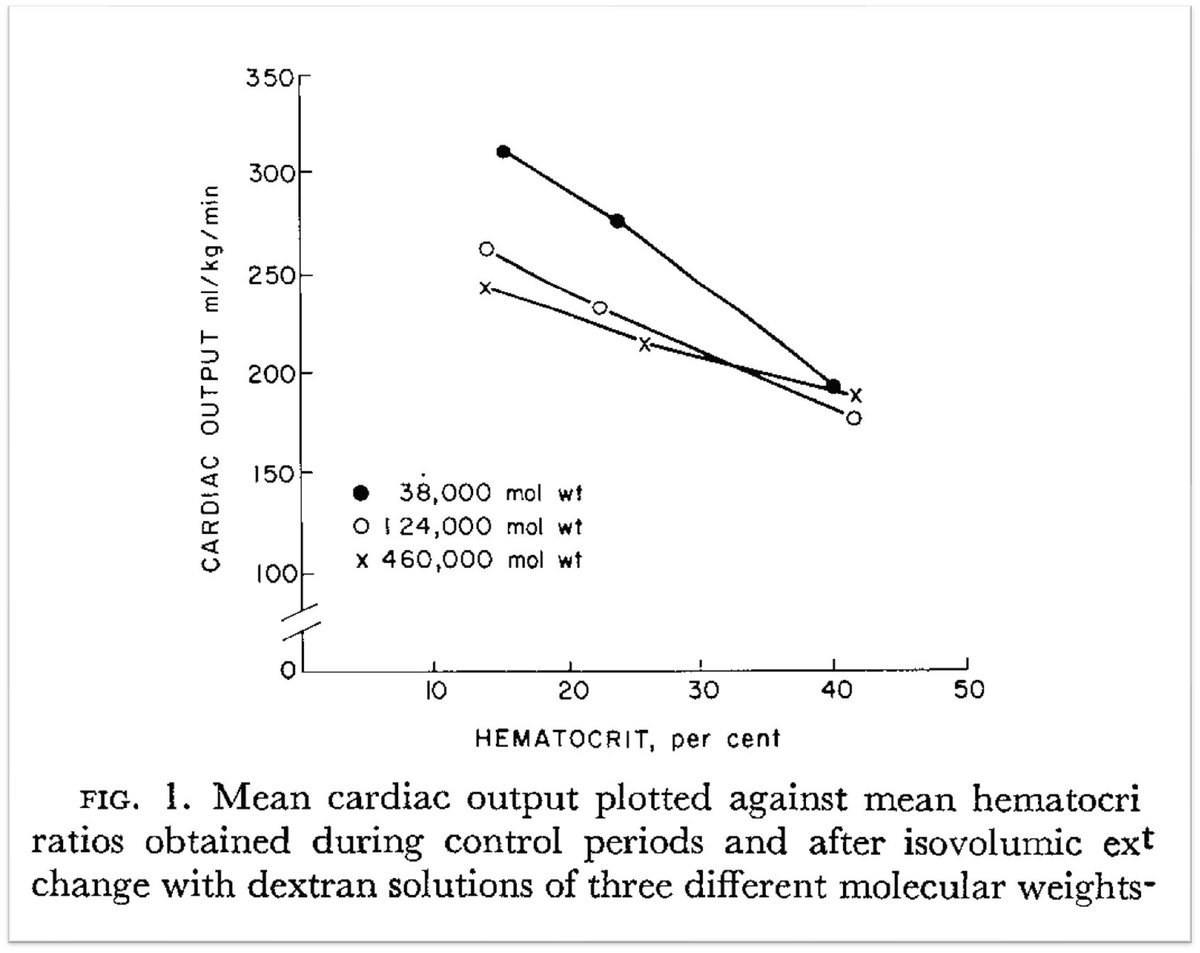
11/
The increase in CI is fostered by the drop in SVR.
The decrease in SVR isn't just due to vasodilation and an increase in the cross-sectional area of blood vessels.
💡It also relates to a decrease in blood viscosity.
The increase in CI is fostered by the drop in SVR.
The decrease in SVR isn't just due to vasodilation and an increase in the cross-sectional area of blood vessels.
💡It also relates to a decrease in blood viscosity.
12/
As the viscosity of blood decreases, venous return increases leading to an increase in cardiac output.
journals.physiology.org
As the viscosity of blood decreases, venous return increases leading to an increase in cardiac output.
journals.physiology.org
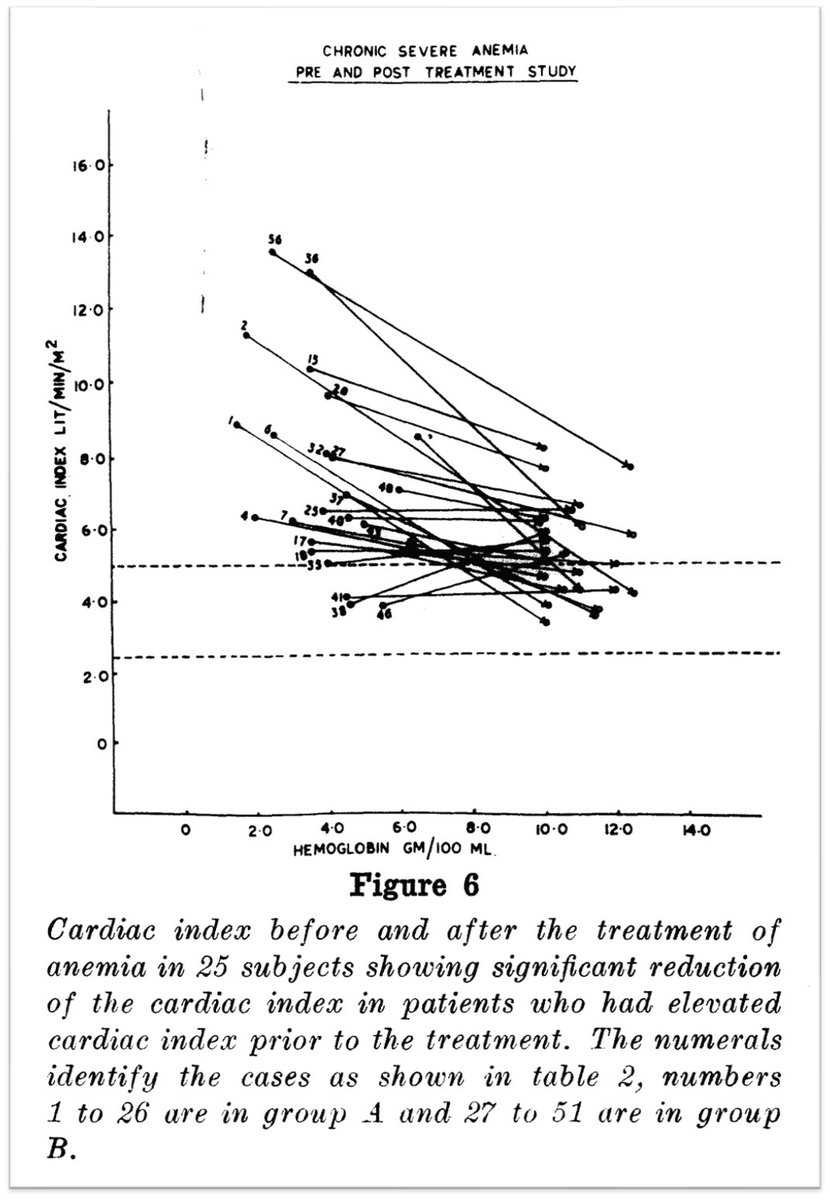
13/
We see similar findings in chronic anemia.
↓systemic vascular resistance (SVR)
↑heart rate, stroke volume, and cardiac index (CI)
ahajournals.org
We see similar findings in chronic anemia.
↓systemic vascular resistance (SVR)
↑heart rate, stroke volume, and cardiac index (CI)
ahajournals.org
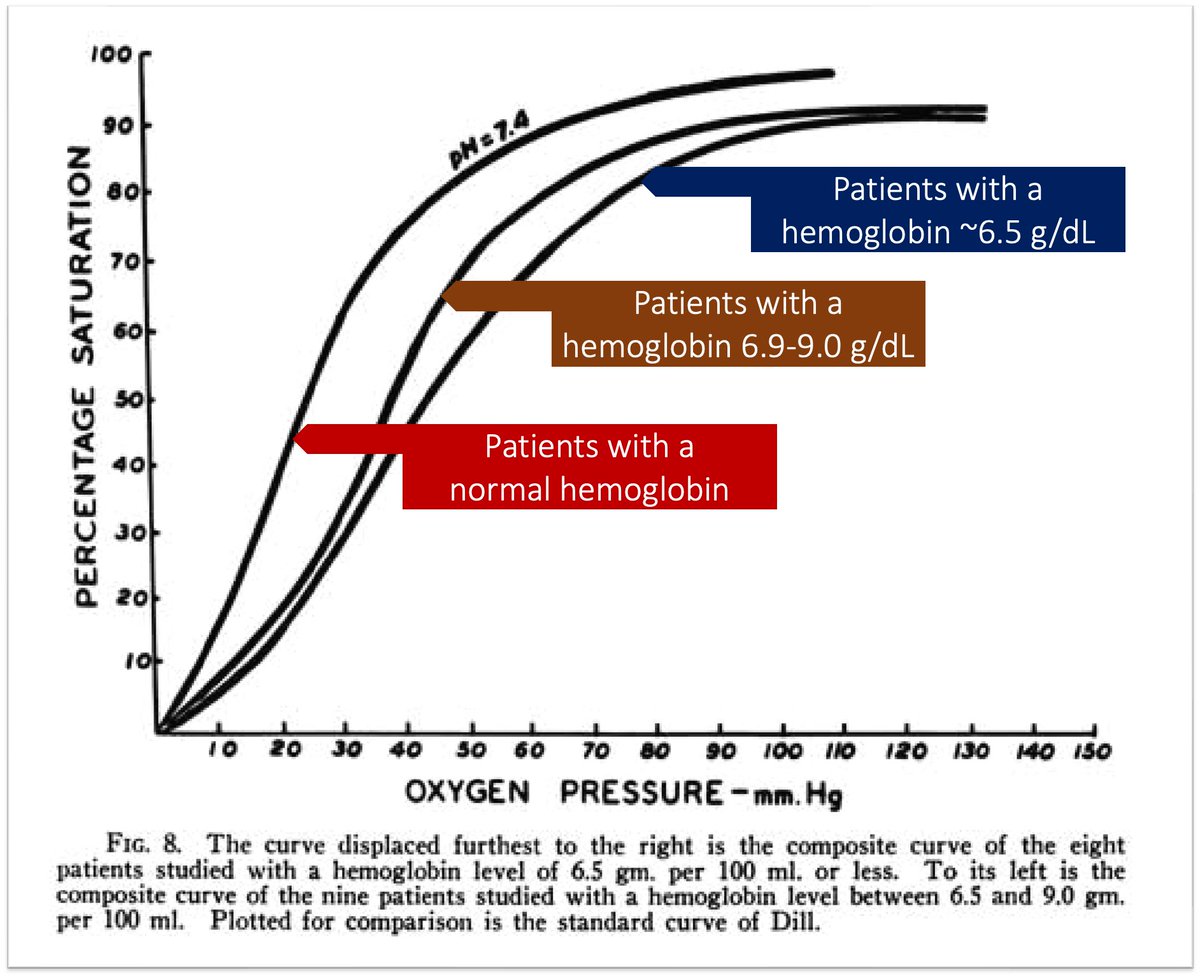
14/
Another major factor ensuring tissue oxygenation is the increased release of O₂. This occurs in part from a right shift on the hemoglobin dissociation curve.
This, in turn, is facilitated by an increase in 2,3-diphosphoglycerate (2,3-DPG).
acpjournals.org
Another major factor ensuring tissue oxygenation is the increased release of O₂. This occurs in part from a right shift on the hemoglobin dissociation curve.
This, in turn, is facilitated by an increase in 2,3-diphosphoglycerate (2,3-DPG).
acpjournals.org
15/
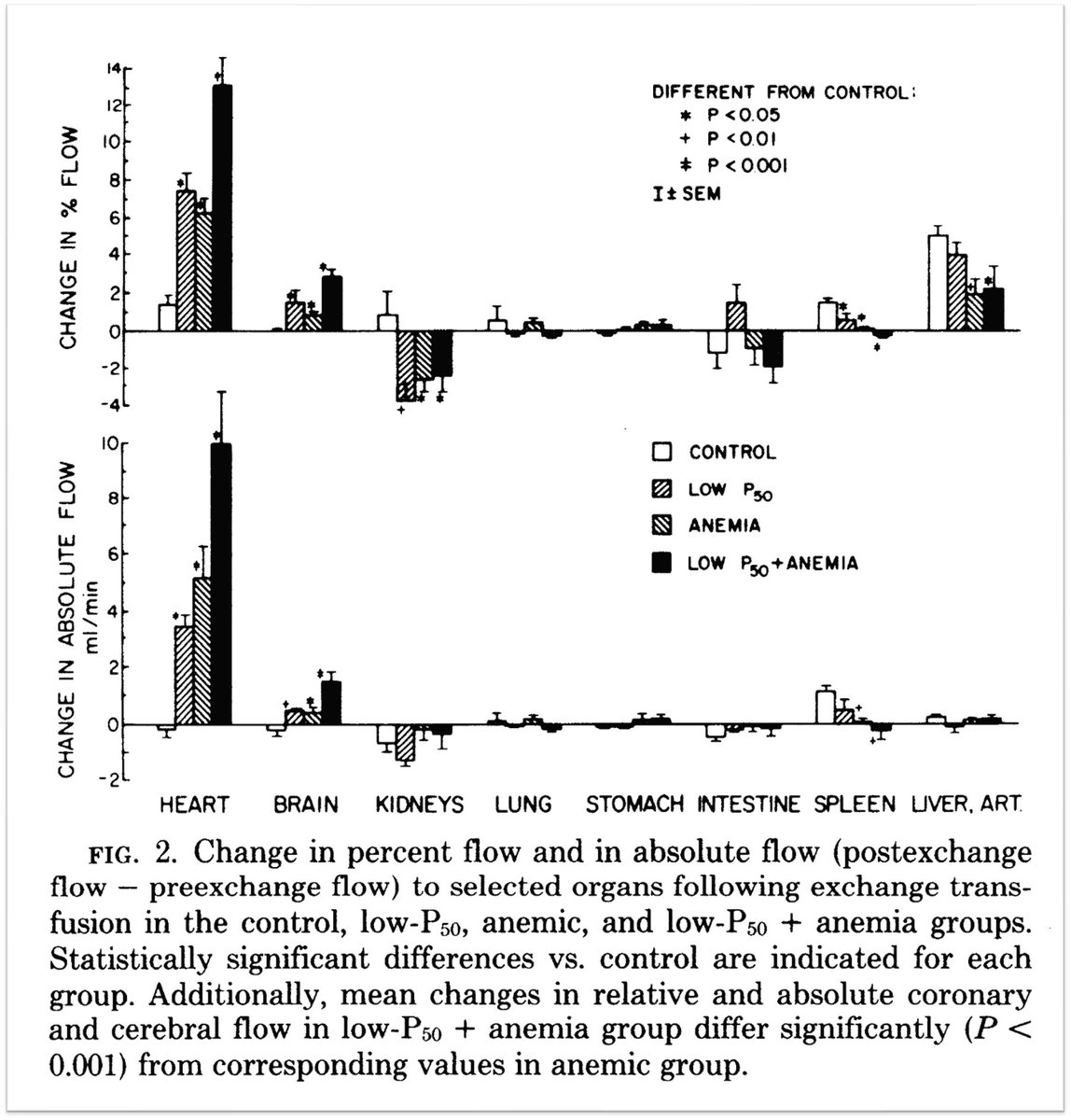
A final adaptation is the redistribution of blood flow to augment the heart and brain over other organs.
This ensures that the most vital organs continue to receive adequate O₂ delivery.
journals.physiology.org
A final adaptation is the redistribution of blood flow to augment the heart and brain over other organs.
This ensures that the most vital organs continue to receive adequate O₂ delivery.
journals.physiology.org

16/
In follow-up tweets, I'll share examples of the extremes of anemia and how individuals were able to survive.
In the meantime, read more about blood transfusions, particularly how we got to current thresholds, on my substack, Origin Stories.
tonybreu.substack.com
In follow-up tweets, I'll share examples of the extremes of anemia and how individuals were able to survive.
In the meantime, read more about blood transfusions, particularly how we got to current thresholds, on my substack, Origin Stories.
tonybreu.substack.com

17/17
🩸When transfusing, our target is not a normal hemoglobin
🩸This stems from risk/benefit ratio, evidence-based medicine, and blood scarcity
🩸Fortunately, the human body has more hemoglobin than is needed
🩸Many physiologic adaptations ensue in acute and chronic anemia
🩸When transfusing, our target is not a normal hemoglobin
🩸This stems from risk/benefit ratio, evidence-based medicine, and blood scarcity
🩸Fortunately, the human body has more hemoglobin than is needed
🩸Many physiologic adaptations ensue in acute and chronic anemia
جاري تحميل الاقتراحات...