

🚨🚨🚨🚨
Which is the best technique (Tx) for a pancreatico-enteric anastomosis ⟖ ⟖ after a #Whipple Operation (#pancreaticoduodenectomy) for #PancreaticCancer?
#Bookmark this #Thread 🧵🧵...
The Pancreatico-enteric anastomosis ready reckoner!
Winning Tx revealed at d end!
Which is the best technique (Tx) for a pancreatico-enteric anastomosis ⟖ ⟖ after a #Whipple Operation (#pancreaticoduodenectomy) for #PancreaticCancer?
#Bookmark this #Thread 🧵🧵...
The Pancreatico-enteric anastomosis ready reckoner!
Winning Tx revealed at d end!


🧿 Post-operative Pancreatic fistula (POPF)-
Incidence- PD - 22-26%, DP - >30%, MP 20-60%!!
🧿 Most relevant & harmful complication; ~26% mortality in Grade C POPF (ISGPS 2016 defn)
🧿 How do you avoid an anastomosis from leaking? By not doing one!
Is that the solution?
Incidence- PD - 22-26%, DP - >30%, MP 20-60%!!
🧿 Most relevant & harmful complication; ~26% mortality in Grade C POPF (ISGPS 2016 defn)
🧿 How do you avoid an anastomosis from leaking? By not doing one!
Is that the solution?
Closure of d MPD by ligation/glue/stapler is clinically ineffective —> Pancreatitis!!
Option 2 - Total Pancreatectomy - (Xtrm high risk, Soft gland, multifocal Ca, MPD <3mm) Downside - Brittle DM
So what is the way out?
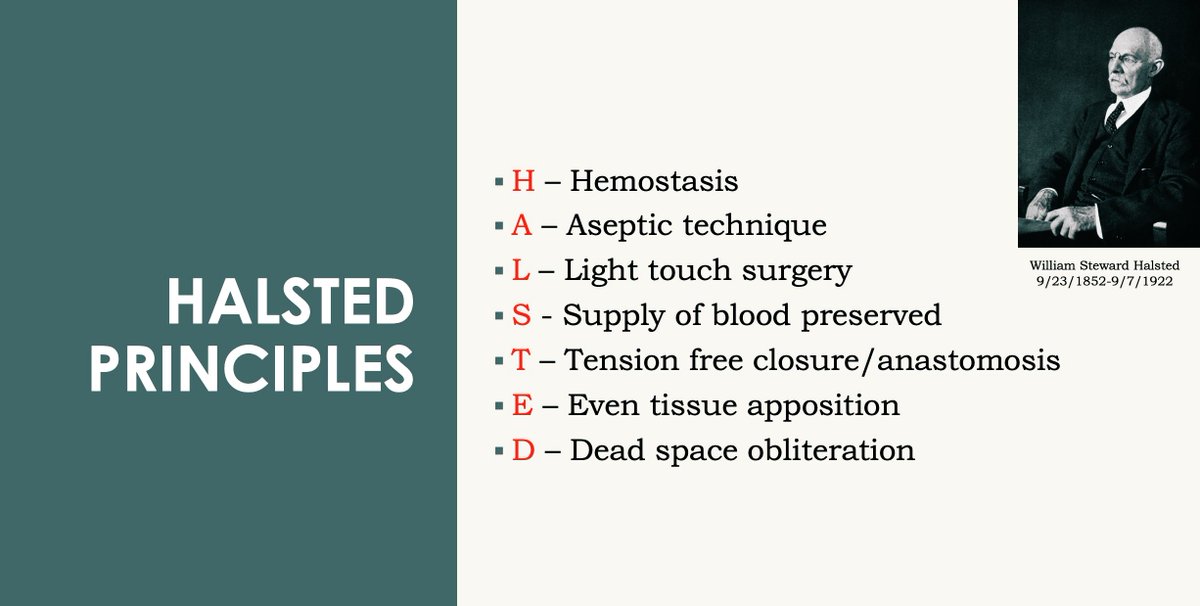
A technically sound anastomosis, respecting Dr Halsted
Option 2 - Total Pancreatectomy - (Xtrm high risk, Soft gland, multifocal Ca, MPD <3mm) Downside - Brittle DM
So what is the way out?
A technically sound anastomosis, respecting Dr Halsted
P-E anastomosis - most effective & safe!
Types of anastomosis - PancJej, PancGast
PancJej - Whipple 1940;
2 major types -
🚨 Invagination - End-end / end-side
🚨 Duct-to-mucosa
t.ly
Types of anastomosis - PancJej, PancGast
PancJej - Whipple 1940;
2 major types -
🚨 Invagination - End-end / end-side
🚨 Duct-to-mucosa
t.ly
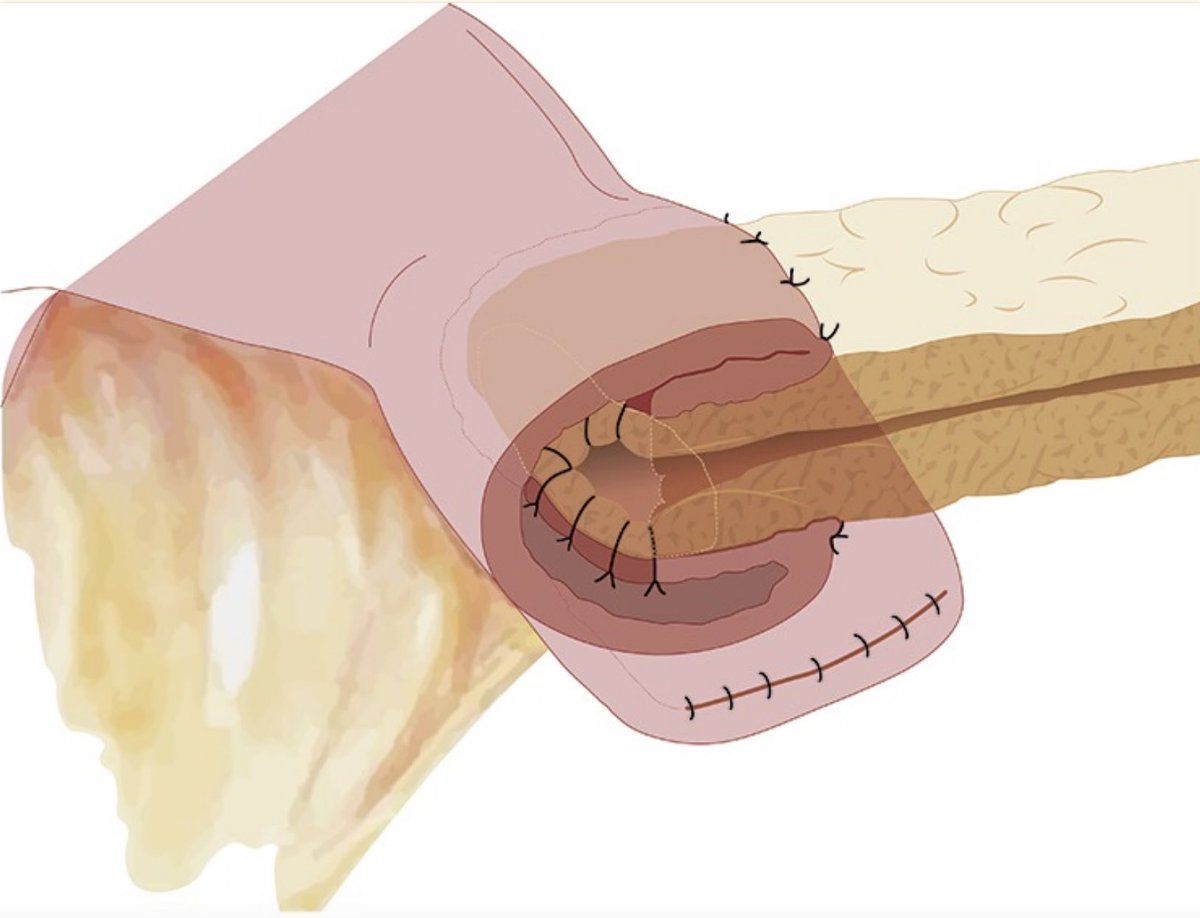

🚨 Standard Invagination Tx - invagination of 1–2 cm of proximal end of d stump into jejunum, end-to-end or end-to-side.
Narrow MPD (<3mm), soft texture
Pro-tip - 1st layer sutures (pans capsule and jejunal seromuscular) should make the jejunal wall go under the stump
Narrow MPD (<3mm), soft texture
Pro-tip - 1st layer sutures (pans capsule and jejunal seromuscular) should make the jejunal wall go under the stump
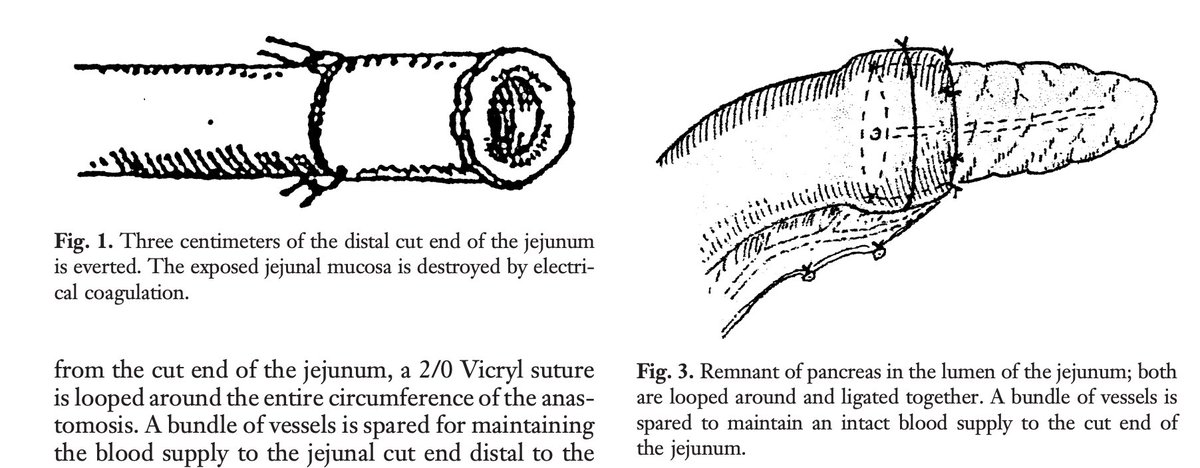
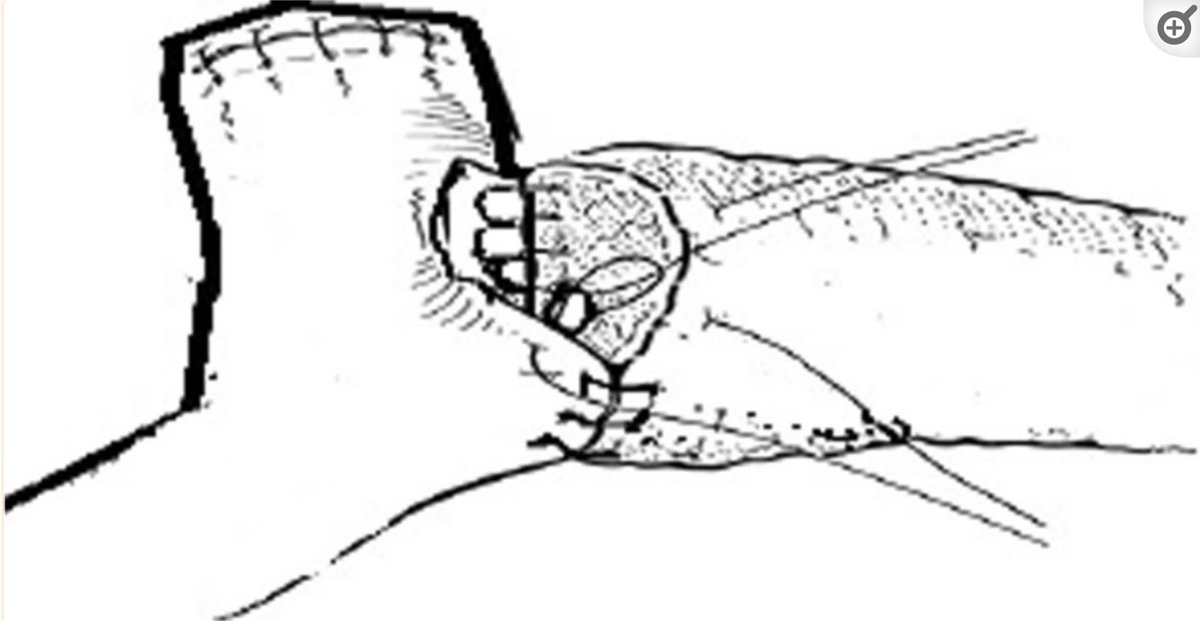
🚨 Peng’s “Binding” Ax -
3 cm of stump & jejunum prepared -> Jejunum everted & mucosa of this part destroyed -> Stump sutured to edge of everted mucosa -> jejunum reverted & wraps 3 cm of stump —> Jejunum compressed by a ligature around it
n = 227 Ax - No leak, not replicated
3 cm of stump & jejunum prepared -> Jejunum everted & mucosa of this part destroyed -> Stump sutured to edge of everted mucosa -> jejunum reverted & wraps 3 cm of stump —> Jejunum compressed by a ligature around it
n = 227 Ax - No leak, not replicated
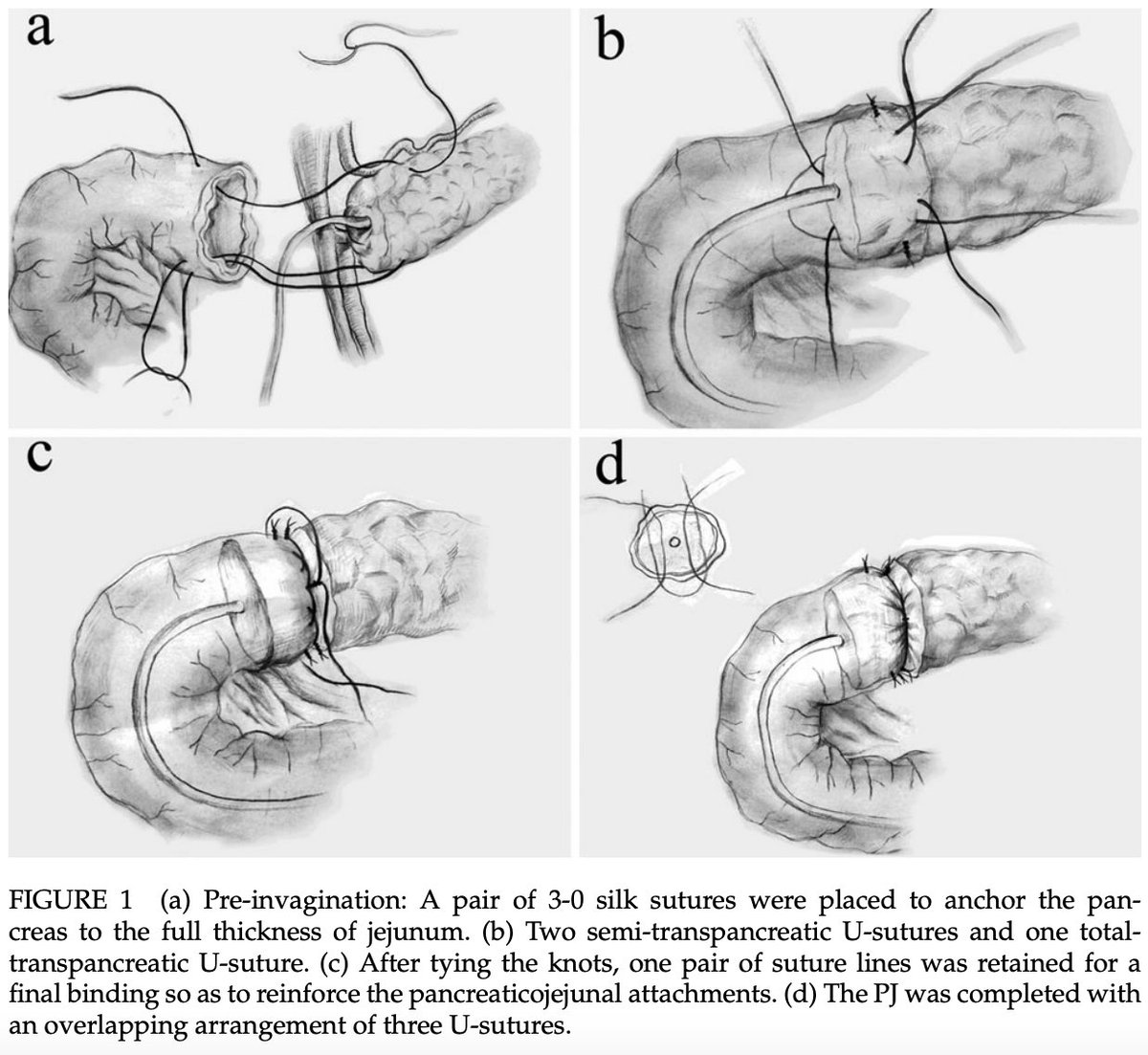
Modifications of Peng Tx - (E -E)
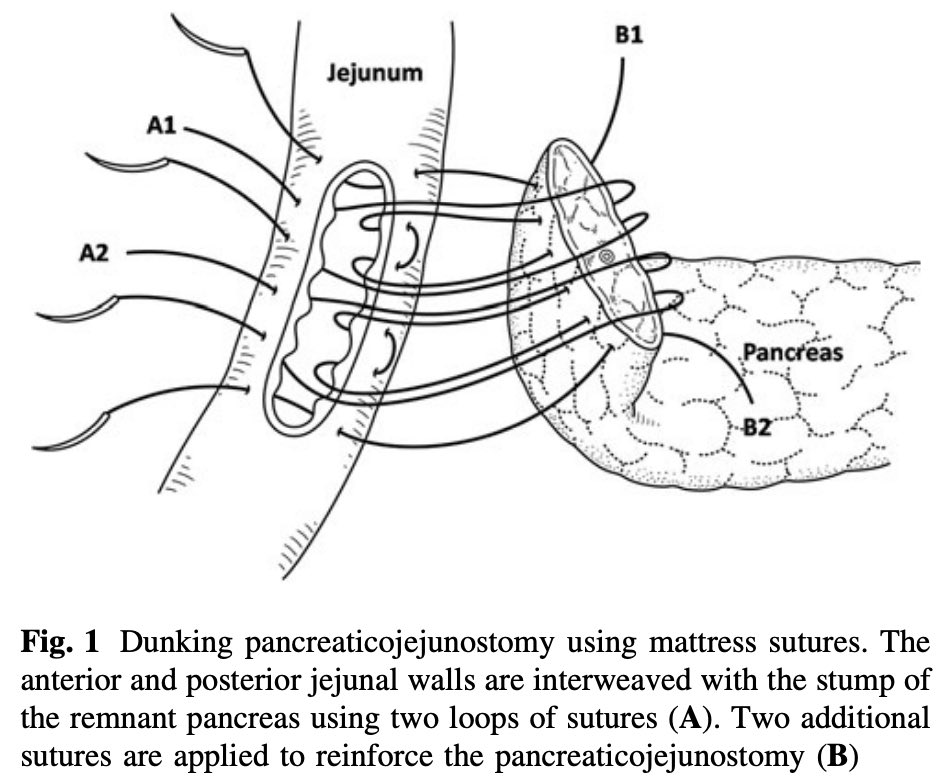
🧩 Kim Tx - Only two transpancreatic U-sutures securing upper & lower border of jejunum, tied using special square buttresses
🧩 Li Tx - 3 overlapping transpancreatic U-sutures to secure d pancreatic stump dunked 3 cm deep into d intestine
🧩 Kim Tx - Only two transpancreatic U-sutures securing upper & lower border of jejunum, tied using special square buttresses
🧩 Li Tx - 3 overlapping transpancreatic U-sutures to secure d pancreatic stump dunked 3 cm deep into d intestine
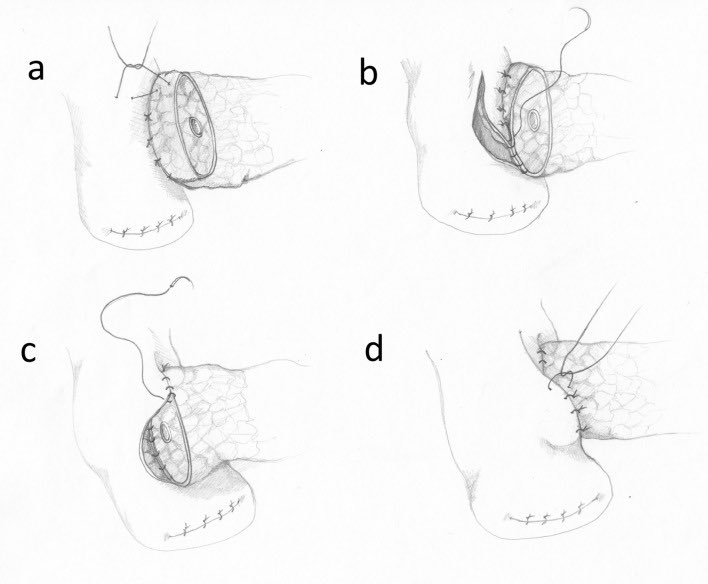
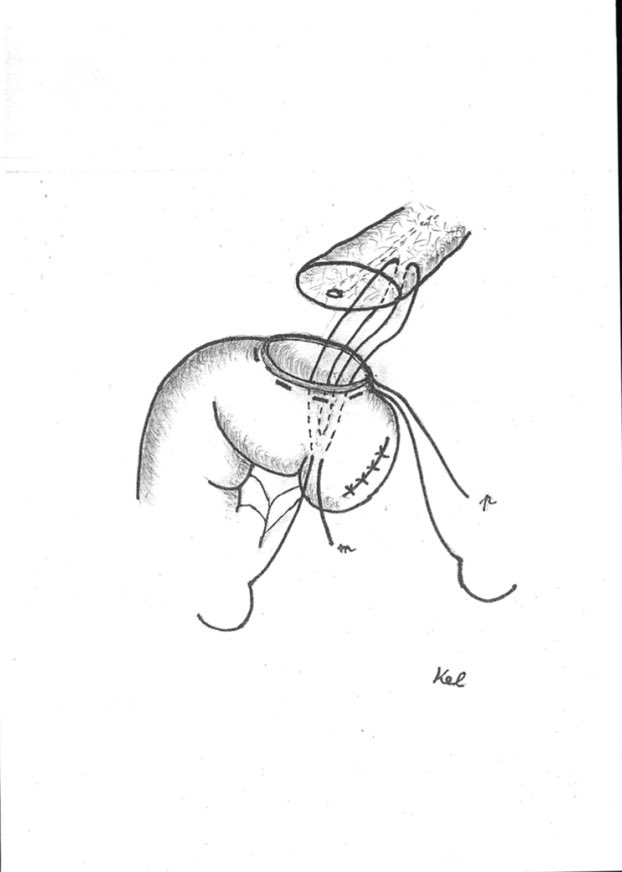
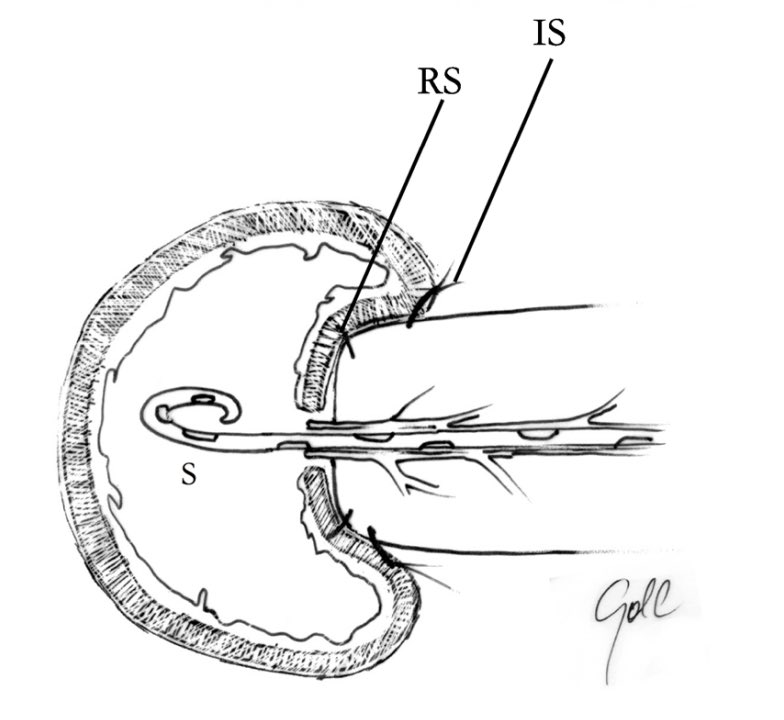
🚨 Kelemen Tx - (E-S) dunking d pancreatic stump 2–3 cm into jejunum with only 3 stitches.
🧿 purse string around jej opening
🧿 two U-sutures fix d end of pancreatic stump deep inside d jejunum
🧿 purse–string suture is tied so as to surround d stump by the jej SM layer
🧿 purse string around jej opening
🧿 two U-sutures fix d end of pancreatic stump deep inside d jejunum
🧿 purse–string suture is tied so as to surround d stump by the jej SM layer
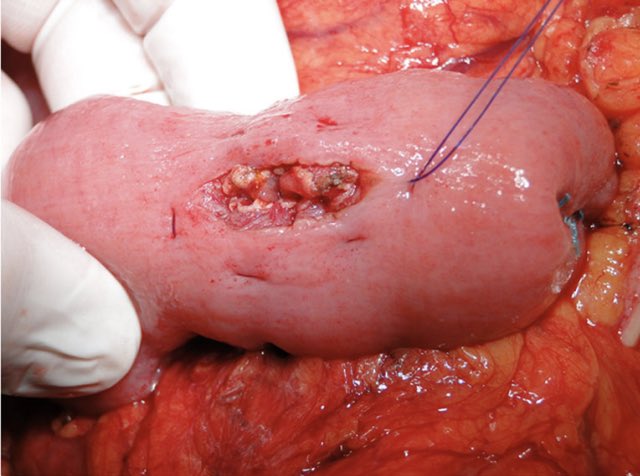
🚨 Gupta Tx - single layer of 4–0 sutures b/w d pancreatic stump & jejunum (through pancreatic capsule, parenchyma & through the whole jejunal wall)
Minimizes the risk of pancreatic trauma
Minimizes the risk of pancreatic trauma
🚨 Chen Tx - (E-E) 2–4 single interrupted double armed U-sutures (Chen’s U-suture)
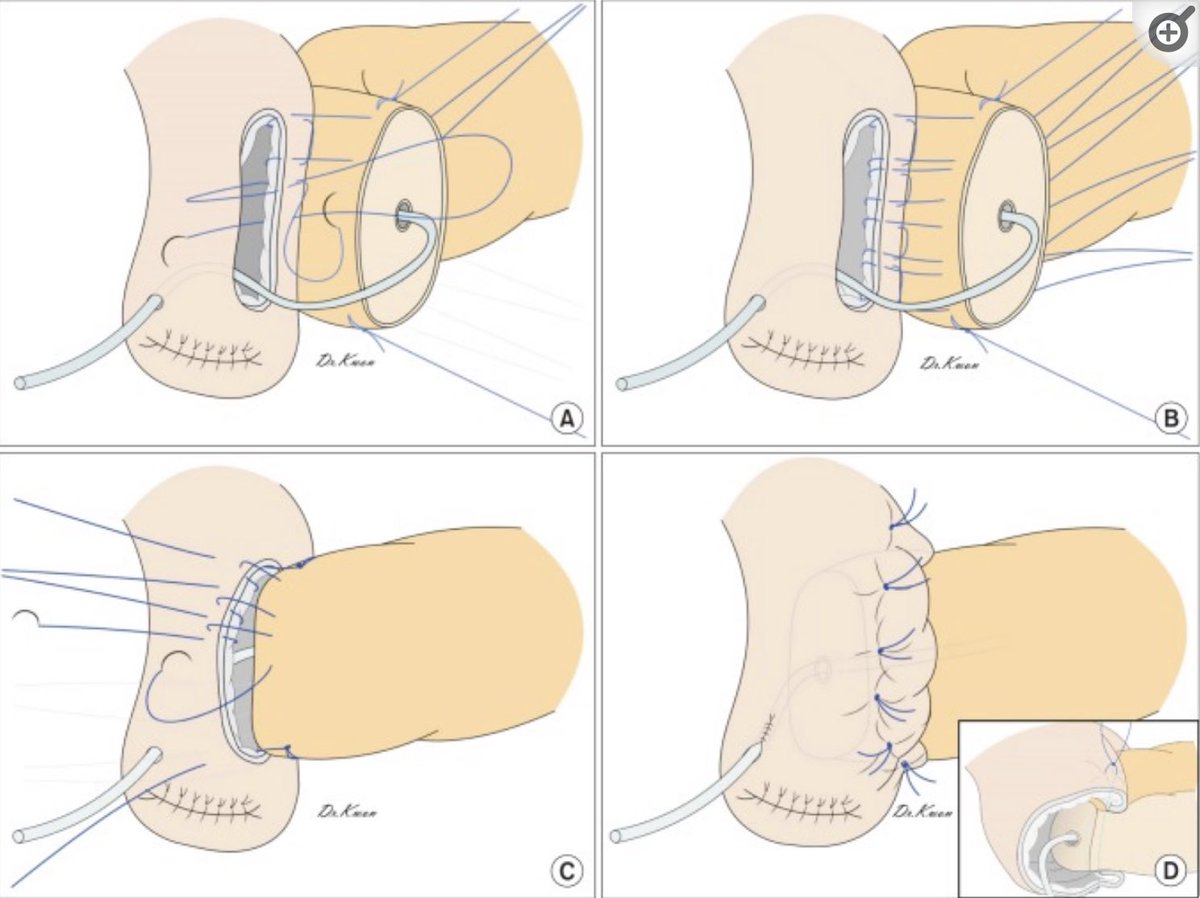
🧩 Cho Tx - (E-S) - single interrupted mattress invaginating sutures - narrow MPD & soft pancreas
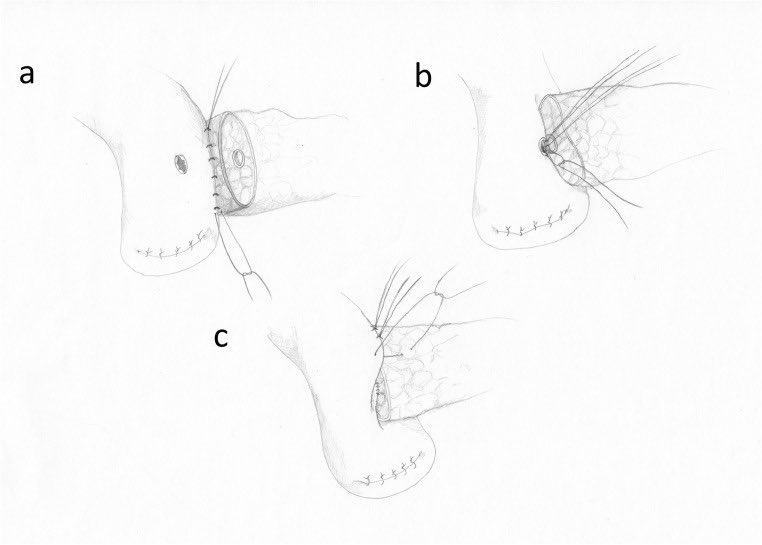
🧩 Kwon Tx - similar to Cho Tx
🧩 Cho Tx - (E-S) - single interrupted mattress invaginating sutures - narrow MPD & soft pancreas
🧩 Kwon Tx - similar to Cho Tx

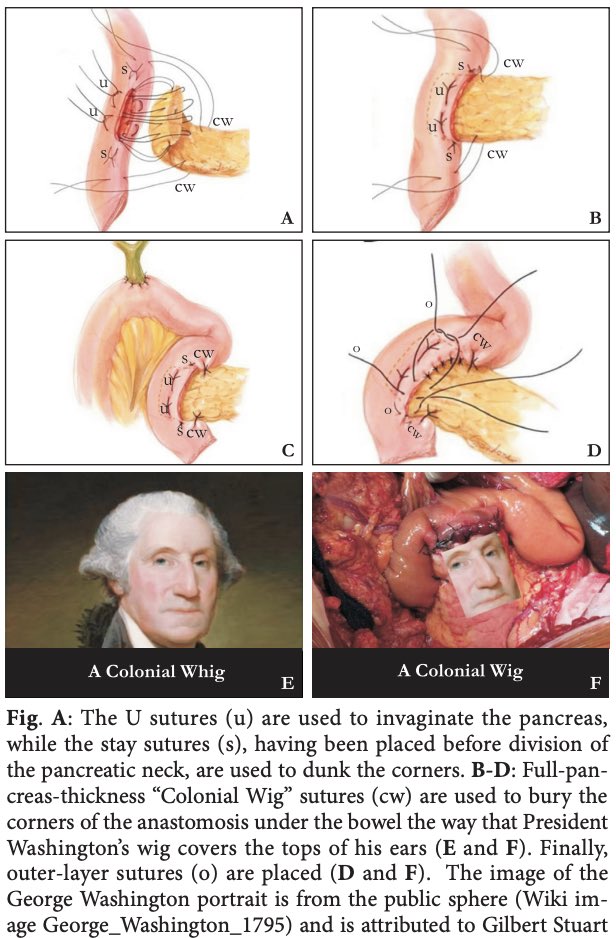
🧩 Yang “Colonial Wig” -
1) panc invaginated by U-sutures into jejunum
2) closed end of jej & deferent loop r sutured by interrupted stitches to pancreatic trunk - secures U & L corners
3) sealing layer of interrupted sutures b/w d capsule & intestinal wall
🧩 Morelli Tx -
1) panc invaginated by U-sutures into jejunum
2) closed end of jej & deferent loop r sutured by interrupted stitches to pancreatic trunk - secures U & L corners
3) sealing layer of interrupted sutures b/w d capsule & intestinal wall
🧩 Morelli Tx -
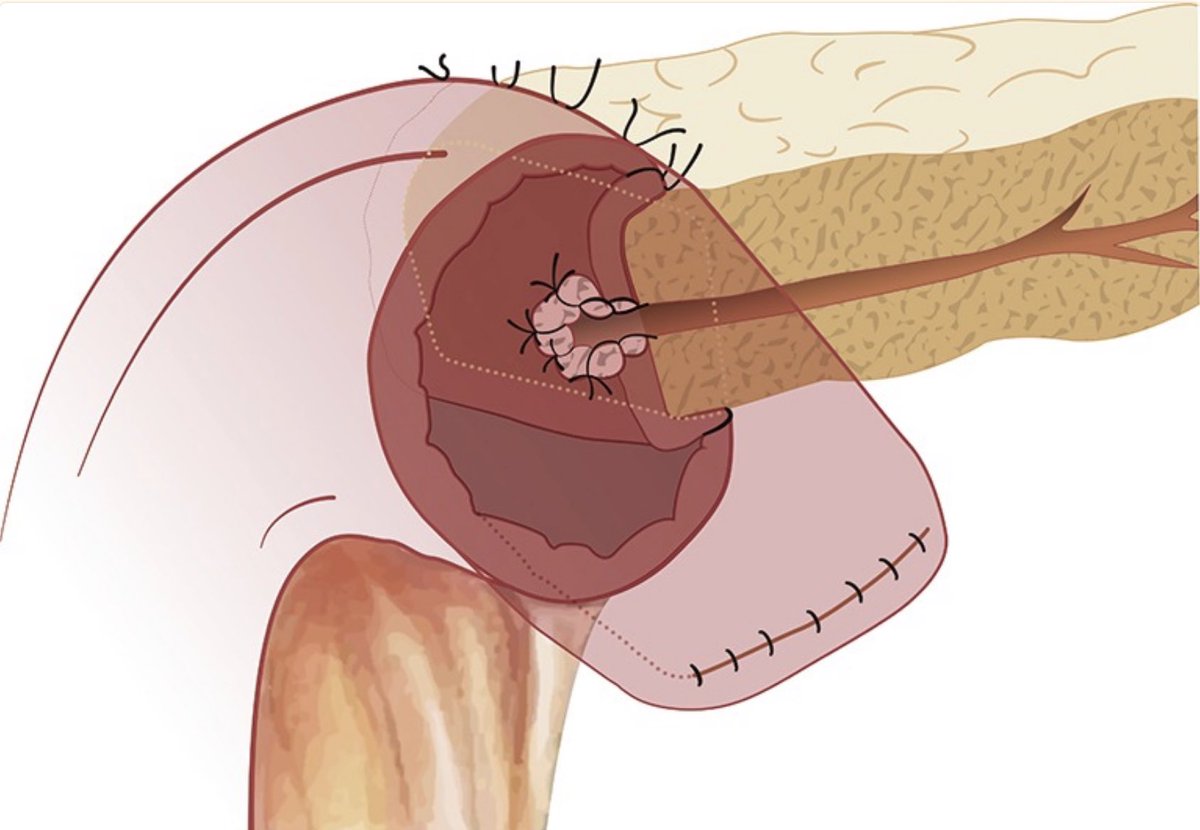
🚨 Duct - Mucosa Ax - MPD sutured to jejunotomy
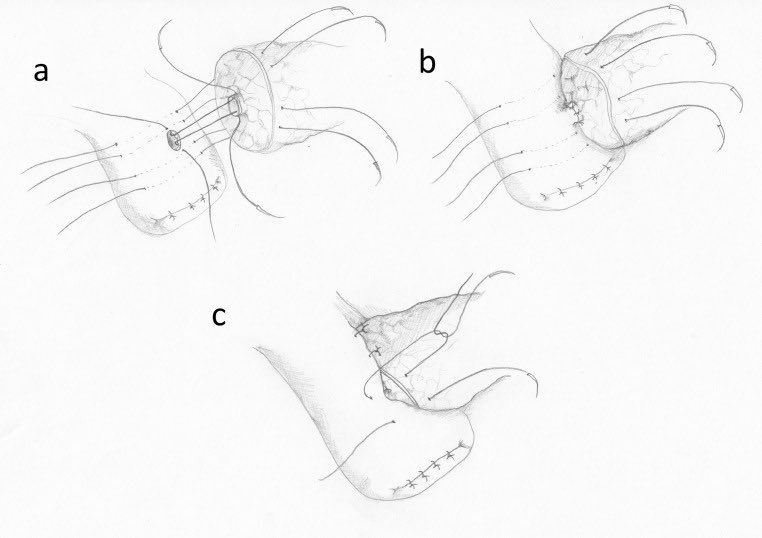
🚨 Cattell-Warren Tx - interrupted monofilament 4–0 sutures thru posterior pancr capsule & seromusc jej
6–12 interrupted monofil 5–0 sutures thru MPD & jejunotomy
external anterior layer - pancreatic capsule & d seromuscular jej
🚨 Cattell-Warren Tx - interrupted monofilament 4–0 sutures thru posterior pancr capsule & seromusc jej
6–12 interrupted monofil 5–0 sutures thru MPD & jejunotomy
external anterior layer - pancreatic capsule & d seromuscular jej
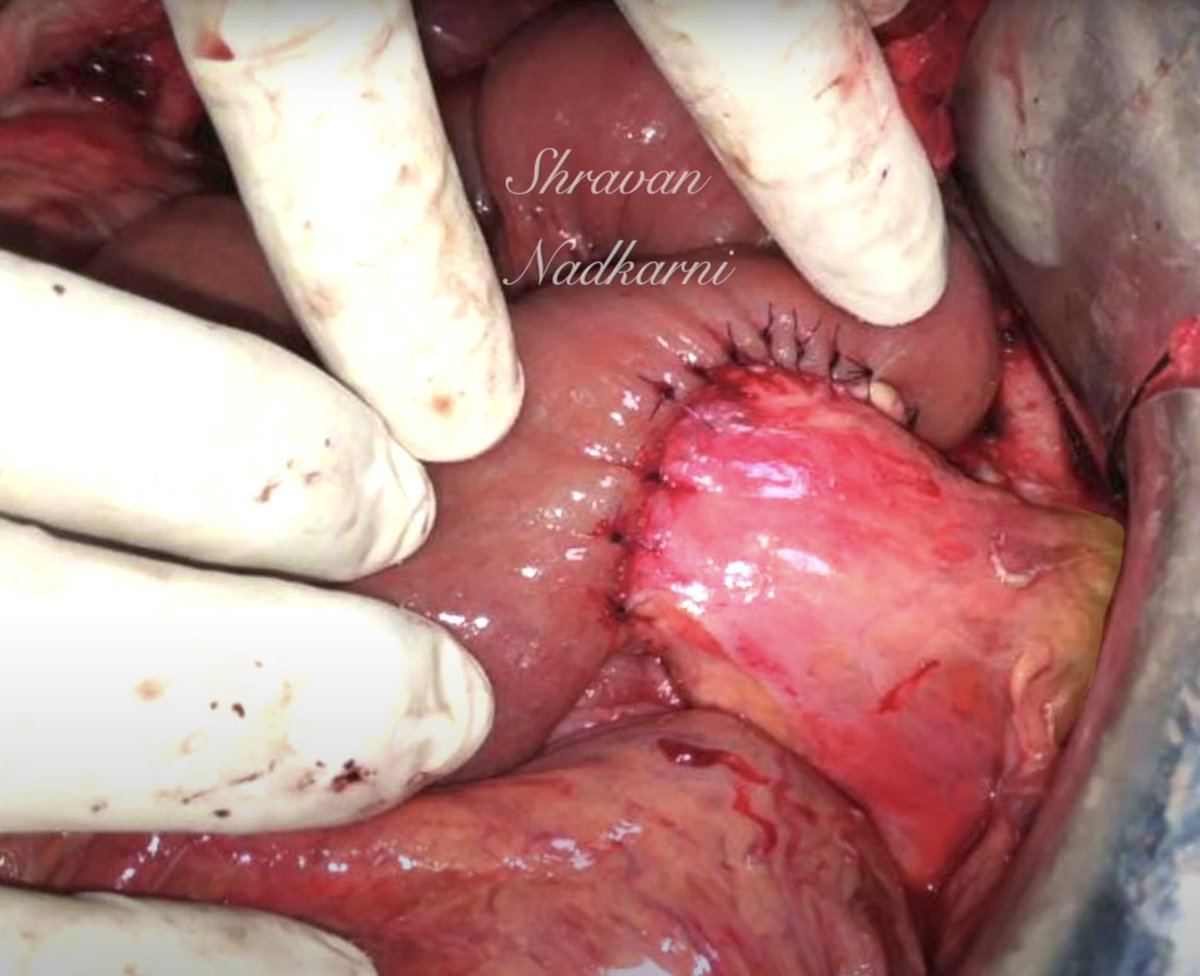
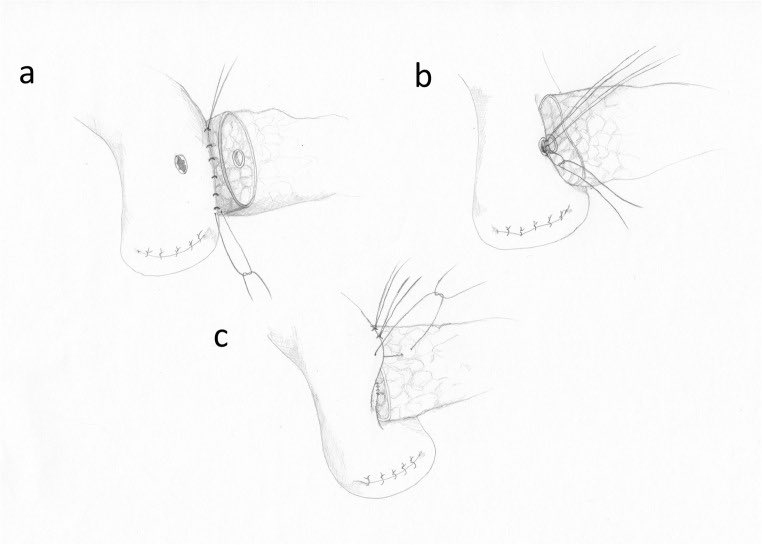
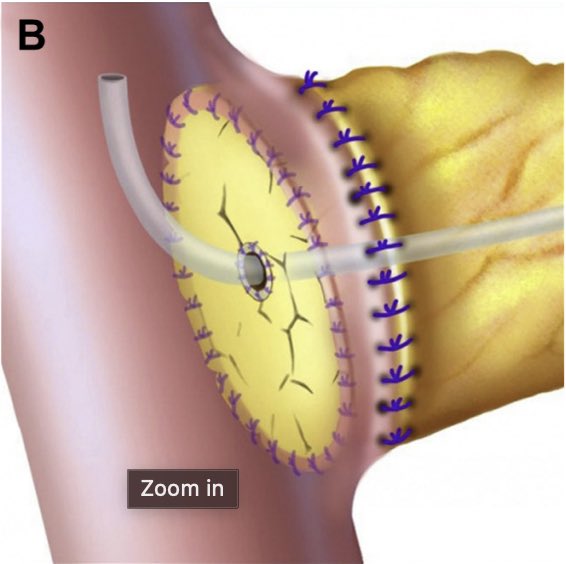
🚨 🚨 Modified Heidelberg Tx - MPD bites at 4, 6, 8 o’clock posterior wall and 10, 12, 2 o’clock anterior wall.
Posterior and anterior layers thru capsule and seromuscular jej
🧩 Su Tx - 3-layer d-m - t.ly
Posterior and anterior layers thru capsule and seromuscular jej
🧩 Su Tx - 3-layer d-m - t.ly

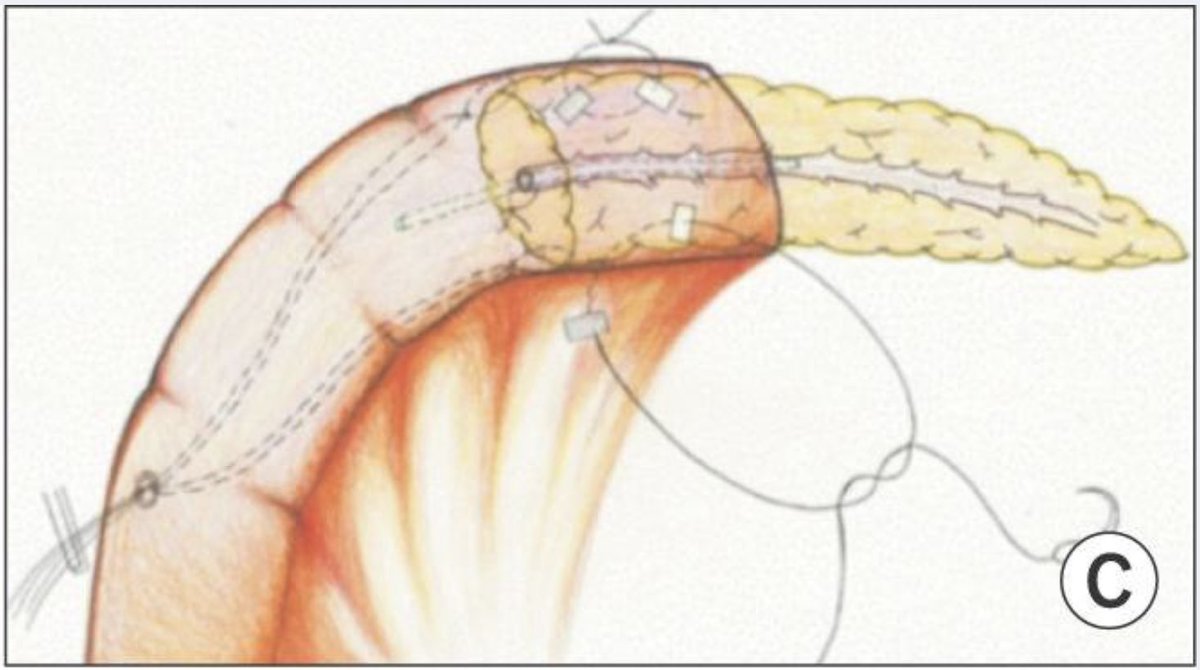
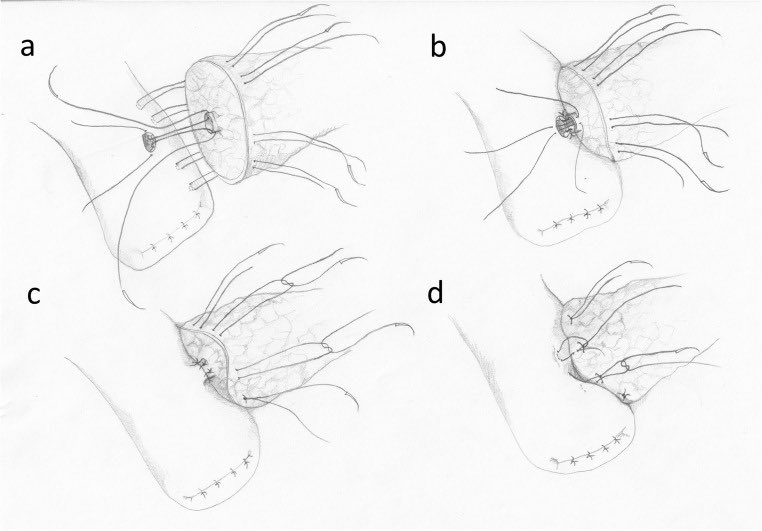
🚨 Blumgart Tx - Transpancreatic sutures
- external layer consists of 4–8 U-sutures
- duct - mucosa - 2 layers
- needles of U sutures passed again through the seromuscular layer of jejunum and tied 2nd time
- external layer consists of 4–8 U-sutures
- duct - mucosa - 2 layers
- needles of U sutures passed again through the seromuscular layer of jejunum and tied 2nd time
🚨 Kakita Tx - duct-mucosa with the external layer - 4 simple interrupted sutures placed transpancreatically & thru seromuscular jej
Ref - t.ly
Ref - t.ly

So which of these is the best technique of all?
PANasta trial - Cattell Warren versus Blumgart Tx, double blinded, multicentre trial
🚨 No significant differences in POPF
t.ly
PANasta trial - Cattell Warren versus Blumgart Tx, double blinded, multicentre trial
🚨 No significant differences in POPF
t.ly

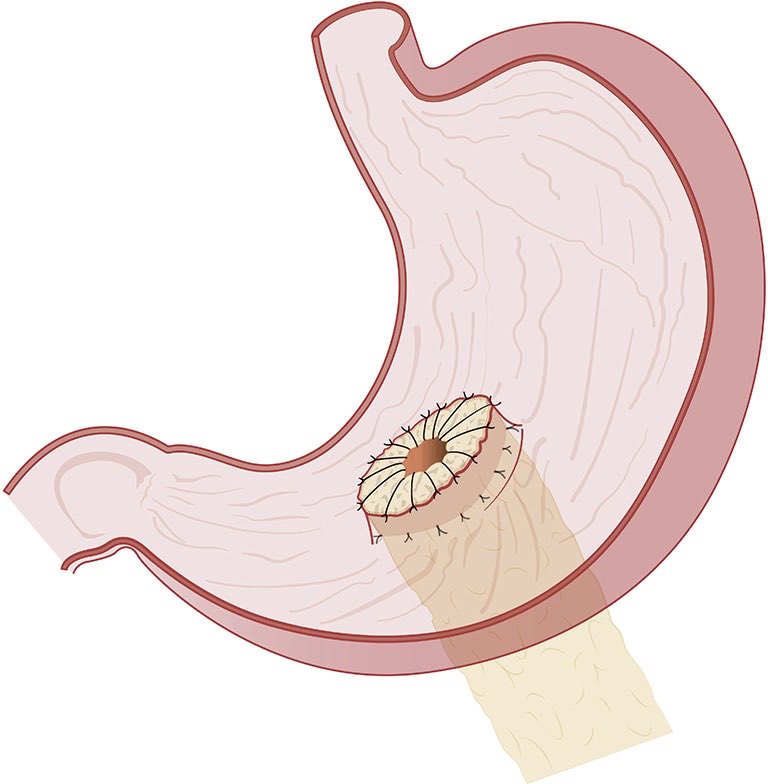
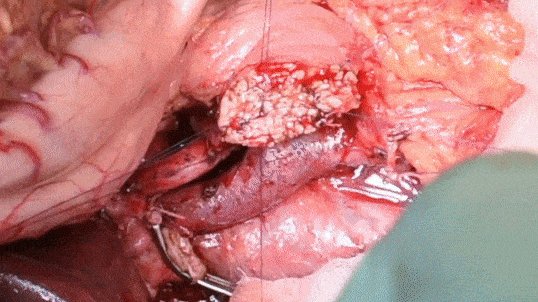
What about Pancreaticogastrostomy?
Rationale -
🧩 Deterrence of pancreatic enzyme activation by gastric acidity
🧩 vicinity of pancreas to gastric wall - tension-free
🧩 Thicker gastric wall, better blood supply, decompression of stomach with an NG tube - ?better healing
Rationale -
🧩 Deterrence of pancreatic enzyme activation by gastric acidity
🧩 vicinity of pancreas to gastric wall - tension-free
🧩 Thicker gastric wall, better blood supply, decompression of stomach with an NG tube - ?better healing

PJ vs PG Meta-analysis -
🧩 POPF rate - PJ 24.3% vs 21.4%
🧩 Need for surgical re‐intervention 11.6% vs 10.3%
🧩 Rate of complications (46.5% vs 44.5%)
🧩 PPH 9.3% 🧨 vs 13.8% (PG)
🚨 No reliable evidence supporting one procedure over the other
t.ly
🧩 POPF rate - PJ 24.3% vs 21.4%
🧩 Need for surgical re‐intervention 11.6% vs 10.3%
🧩 Rate of complications (46.5% vs 44.5%)
🧩 PPH 9.3% 🧨 vs 13.8% (PG)
🚨 No reliable evidence supporting one procedure over the other
t.ly

Summary- Means to an end, no single technique better than d other
Probably best to master 1-2 Txs for different scenarios & use them with fidelity
Our SOP - 🧨 Mod Heidelberg D-M 🧨
In cricketing lingo - “When you have a winning team, don’t change it” quoting @Shrikhande_SV
Probably best to master 1-2 Txs for different scenarios & use them with fidelity
Our SOP - 🧨 Mod Heidelberg D-M 🧨
In cricketing lingo - “When you have a winning team, don’t change it” quoting @Shrikhande_SV
@Shrikhande_SV @TataMemorial @TMC_Varanasi @hbchsangrur @YouppiePancreas @surgery_hps @EurPancClub @PancreasClub @PanCAN @PancreaticCanUK @PancreasVerona @IHPBA @APHPBA2023 @HpbKarolinska @HpbChl @GIoncology_MICC @HpbLounge @hpbsurgeon1 @ItaruEndo @JasSamra8 @somedocs @me4_so @Some4SurgeryIT1 @hpb_so @SoMeHPBNepal @PhilipMueller_1 @ProfessorMWB @pjshukla @PAHPBS1 @harsh_kanhere @EAHPBA @AHPBA @JSHBPS @T4UGIS @IndianYoungOnco @OPENoncology @ESSOnews @SocSurgOnc @WorldSurgical @modern_surgeon @for_surgery @for_surgeons @aahpbs @OxfordHPB @aamirparray18 @sgeorgebarreto
@Shrikhande_SV @TataMemorial @TMC_Varanasi @hbchsangrur @YouppiePancreas @surgery_hps @EurPancClub @PancreasClub @PanCAN @PancreaticCanUK @PancreasVerona @IHPBA @APHPBA2023 @HpbKarolinska @HpbChl @GIoncology_MICC @HpbLounge @hpbsurgeon1 @ItaruEndo @JasSamra8 @somedocs @me4_so @Some4SurgeryIT1 @hpb_so @SoMeHPBNepal @PhilipMueller_1 @ProfessorMWB @pjshukla @PAHPBS1 @harsh_kanhere @EAHPBA @AHPBA @JSHBPS @T4UGIS @IndianYoungOnco @OPENoncology @ESSOnews @NawazUsmanDr @NaveenaANKumar1 @TeamSurgery247 @SStattner @Giampaolo_Perri @Manishbhandare4 @DrVAChaudhari @Saneya_2810 @Vivekanandkem @sanketbankar1 @DrPJagannath @DrGuruduttVarty @drsadiqs
@Shrikhande_SV @TataMemorial @TMC_Varanasi @hbchsangrur @YouppiePancreas @surgery_hps @EurPancClub @PancreasClub @PanCAN @PancreaticCanUK @PancreasVerona @IHPBA @APHPBA2023 @HpbKarolinska @HpbChl @GIoncology_MICC @HpbLounge @hpbsurgeon1 @ItaruEndo @JasSamra8 @somedocs @me4_so @Some4SurgeryIT1 @hpb_so @SoMeHPBNepal @PhilipMueller_1 @ProfessorMWB @pjshukla @PAHPBS1 @harsh_kanhere @EAHPBA @AHPBA @JSHBPS @T4UGIS @IndianYoungOnco @OPENoncology @ESSOnews @NawazUsmanDr @NaveenaANKumar1 @TeamSurgery247 @SStattner @Giampaolo_Perri @Manishbhandare4 @DrVAChaudhari @Saneya_2810 @vivekanandkem @sanketbankar1 @DrPJagannath @DrGuruduttVarty 🧩🧩
The ISGPS Consensus statement on Pancreatic-enteric anastomosis
@ISGPS_news
pubmed.ncbi.nlm.nih.gov
Full text - t.ly
The ISGPS Consensus statement on Pancreatic-enteric anastomosis
@ISGPS_news
pubmed.ncbi.nlm.nih.gov
Full text - t.ly

pubmed.ncbi.nlm.nih.gov/28027816/
Pancreatic anastomosis after pancreatoduodenectomy: A position statement by the International Study Group of Pancreatic Surgery (ISGPS) - PubMed
Currently, no specific technique can eliminate development of clinically relevant postoperative panc...
t.ly/5NR7K
ClinicalKey
@Shrikhande_SV @TataMemorial @TMC_Varanasi @hbchsangrur @YouppiePancreas @surgery_hps @EurPancClub @PancreasClub @PanCAN @PancreaticCanUK @PancreasVerona @IHPBA @APHPBA2023 @HpbKarolinska @HpbChl @GIoncology_MICC @HpbLounge @hpbsurgeon1 @ItaruEndo @JasSamra8 @somedocs @me4_so @Some4SurgeryIT1 @hpb_so @SoMeHPBNepal @PhilipMueller_1 @ProfessorMWB @pjshukla @PAHPBS1 @harsh_kanhere @EAHPBA @AHPBA @JSHBPS @T4UGIS @IndianYoungOnco @OPENoncology @ESSOnews @NawazUsmanDr @NaveenaANKumar1 @TeamSurgery247 @SStattner @Giampaolo_Perri @Manishbhandare4 @DrVAChaudhari @Saneya_2810 @vivekanandkem @sanketbankar1 Technique of a pancreaticogastrostomy -
@durgatoshpandey @TMC_Varanasi @docswapnil01
@durgatoshpandey @TMC_Varanasi @docswapnil01
@Shrikhande_SV @TataMemorial @TMC_Varanasi @hbchsangrur @YouppiePancreas @surgery_hps @EurPancClub @PancreasClub @PanCAN @PancreaticCanUK @PancreasVerona @IHPBA @APHPBA2023 @HpbKarolinska @HpbChl @GIoncology_MICC @HpbLounge @hpbsurgeon1 @ItaruEndo @JasSamra8 @somedocs @me4_so @Some4SurgeryIT1 @hpb_so @SoMeHPBNepal @PhilipMueller_1 @ProfessorMWB @pjshukla @PAHPBS1 @harsh_kanhere @EAHPBA @AHPBA @JSHBPS @T4UGIS @IndianYoungOnco @OPENoncology @ESSOnews @NawazUsmanDr @NaveenaANKumar1 @TeamSurgery247 @SStattner @Giampaolo_Perri @Manishbhandare4 @DrVAChaudhari @Saneya_2810 @vivekanandkem @sanketbankar1 @durgatoshpandey @docswapnil01 Let me add 1 final tweet
Mortality of a #Whipple has reduced to <5% (high vol centers) from ~25-30% - v r probably managing pts better
But Morbidity still remains high (30-60%) - despite refinement in Txs
What are v missing?
t.ly
t.ly
Mortality of a #Whipple has reduced to <5% (high vol centers) from ~25-30% - v r probably managing pts better
But Morbidity still remains high (30-60%) - despite refinement in Txs
What are v missing?
t.ly
t.ly

t.ly/G_gFk
Defining post-operative pancreatitis as a new pancreatic specific complication following pancreatic resection
Post-operative pancreatic fistula has been well defined. However the underlying aetiology remains po...

t.ly/gecab
Acinar cell density at the pancreatic resection margin is associated with post-pancreatectomy pancreatitis and the development of postoperative pancreatic fistula - PubMed
The development of POPF may involve a complex interaction between acinar cell density, immediate lea...
@Shrikhande_SV @TataMemorial @TMC_Varanasi @hbchsangrur @YouppiePancreas @surgery_hps @EurPancClub @PancreasClub @PanCAN @PancreaticCanUK @PancreasVerona @IHPBA @APHPBA2023 @HpbKarolinska @HpbChl @GIoncology_MICC @HpbLounge @hpbsurgeon1 @ItaruEndo @JasSamra8 @somedocs @me4_so @Some4SurgeryIT1 @hpb_so @SoMeHPBNepal @PhilipMueller_1 @ProfessorMWB @pjshukla @PAHPBS1 @harsh_kanhere @EAHPBA @AHPBA @JSHBPS @T4UGIS @IndianYoungOnco @OPENoncology @ESSOnews @NawazUsmanDr @NaveenaANKumar1 @TeamSurgery247 @SStattner @Giampaolo_Perri @Manishbhandare4 @DrVAChaudhari @Saneya_2810 @vivekanandkem As usual, the 🚨🚨🧨 BONUS tweet -
🧩 Recommended reading
Latest @ISGPS_news article on the definition and grading of Postpancreatectomy Acute Pancreatitis (PPAP)
t.ly
@Shrikhande_SV @Gio_Marchegiani @sgeorgebarreto
🧩 Recommended reading
Latest @ISGPS_news article on the definition and grading of Postpancreatectomy Acute Pancreatitis (PPAP)
t.ly
@Shrikhande_SV @Gio_Marchegiani @sgeorgebarreto

Loading suggestions...