

A lot of people respond to videos like this by saying “we’d mobilize patients earlier if we had the staff.”
Early ICU mobility is tied to both shorter ICU/hospital LOS & savings of ~$1m/year.
The best way to have more staff *IS* to mobilize people early in the ICU.
1/
Early ICU mobility is tied to both shorter ICU/hospital LOS & savings of ~$1m/year.
The best way to have more staff *IS* to mobilize people early in the ICU.
1/
This a meta-analysis of 15 RCTs (1941 patients) found early mobility was associated with:
🗓️1.8 days shorter ICU stay
🗓️3.9 days shorter hospital stay
Early mobility also reduced ICU acquired weakness, risk of DVTs, VAP, & pressure injury.
pubmed.ncbi.nlm.nih.gov
2/
🗓️1.8 days shorter ICU stay
🗓️3.9 days shorter hospital stay
Early mobility also reduced ICU acquired weakness, risk of DVTs, VAP, & pressure injury.
pubmed.ncbi.nlm.nih.gov
2/

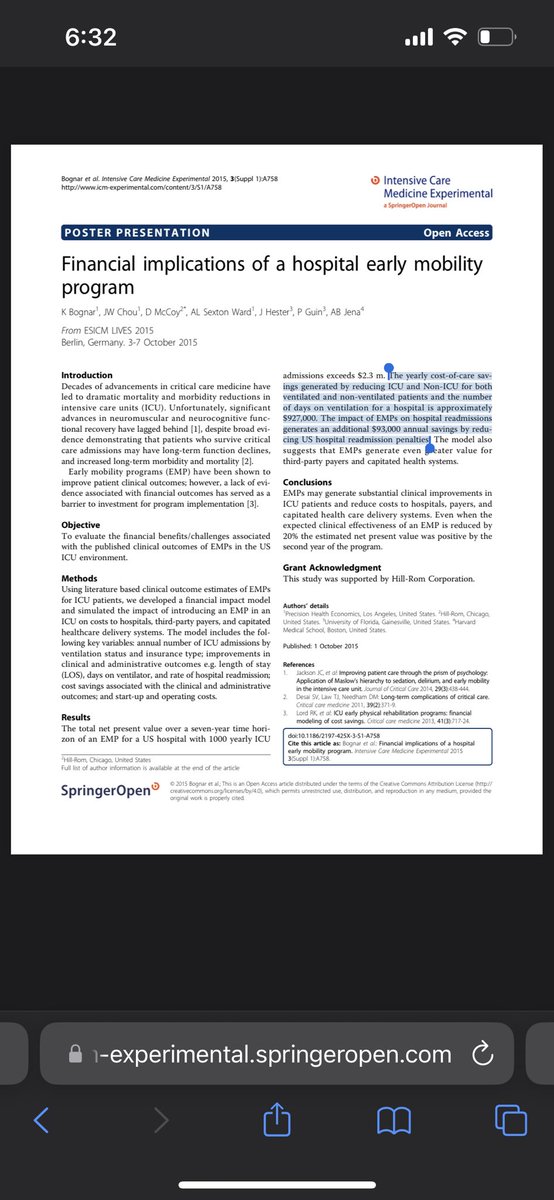
A financial analysis suggested that for an average ICU (1000 admissions/yr), adopting an early ICU mobility program resulted in a net savings of $927,000.
Plus another $97,000 by averting readmission penalties.
icm-experimental.springeropen.com
Early ICU mobility pays for itself!
3/
Plus another $97,000 by averting readmission penalties.
icm-experimental.springeropen.com
Early ICU mobility pays for itself!
3/

It’s also important to emphasize that clinicians like seeing our patients get better.
I suspect that having early mobility programs improves staff satisfaction and reduces burnout & turnover.
(We need more studies to prove this.)
4/
I suspect that having early mobility programs improves staff satisfaction and reduces burnout & turnover.
(We need more studies to prove this.)
4/
A lot of misunderstandings of this thread.
Assuming you have a fixed amount of ICU staff, if you shorten ICU LOS by 2 days, you’ve de facto increased the number of staff available to help mobilize patients. Even if you don’t/can’t hire more people, having fewer pts helps.
Assuming you have a fixed amount of ICU staff, if you shorten ICU LOS by 2 days, you’ve de facto increased the number of staff available to help mobilize patients. Even if you don’t/can’t hire more people, having fewer pts helps.
Loading suggestions...