

1/
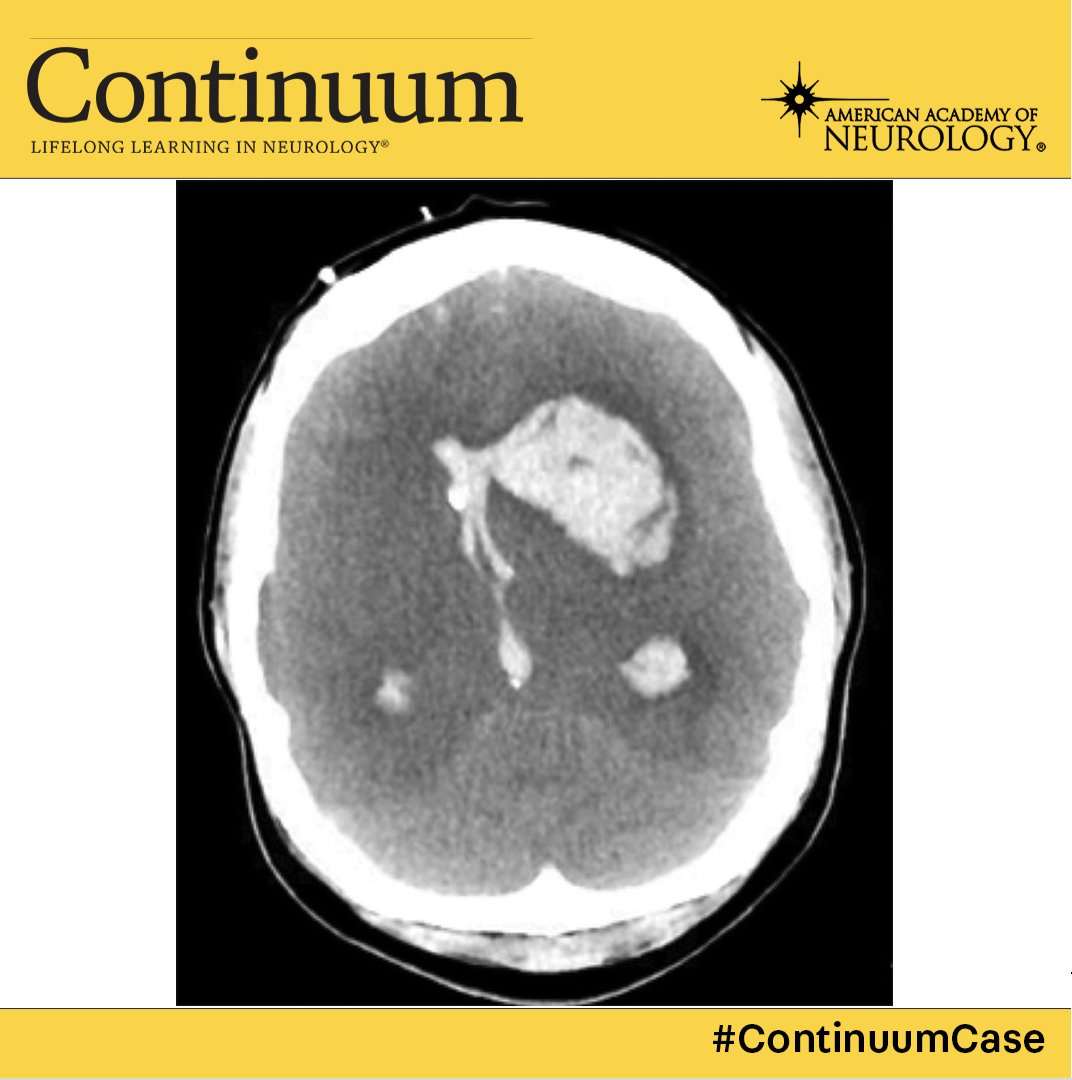
A 21 yo G1P0 reports a severe headache 3 days after delivery.
BP 182/100😱
While waiting to be admitted, she vomits & has a generalized tonic clonic seizure.
She is sedated and intubated for eclampsia.
The next morning, she has blown pupils.
A #continuumcase. @LyellJ
A 21 yo G1P0 reports a severe headache 3 days after delivery.
BP 182/100😱
While waiting to be admitted, she vomits & has a generalized tonic clonic seizure.
She is sedated and intubated for eclampsia.
The next morning, she has blown pupils.
A #continuumcase. @LyellJ
2/
(What happened to cases from the sleep issue, you ask!?
We’ll get back there, but I’m reviewing the 2022 issue on the neurology of pregnancy for the EB meeting… )
Didn't you want some tips on neuro-emergencies in pregnancy?
(What happened to cases from the sleep issue, you ask!?
We’ll get back there, but I’m reviewing the 2022 issue on the neurology of pregnancy for the EB meeting… )
Didn't you want some tips on neuro-emergencies in pregnancy?
3/
Pregnancy is a very scary time (having just been there myself I can confirm there seems to always be something to worry about!).
🤰Pregnancy TRIPLES the incident of stroke (compared to non-preg women childbearing age)
🤰Maternal stroke complicates 30 of 100,000 deliveries!!
Pregnancy is a very scary time (having just been there myself I can confirm there seems to always be something to worry about!).
🤰Pregnancy TRIPLES the incident of stroke (compared to non-preg women childbearing age)
🤰Maternal stroke complicates 30 of 100,000 deliveries!!
4/
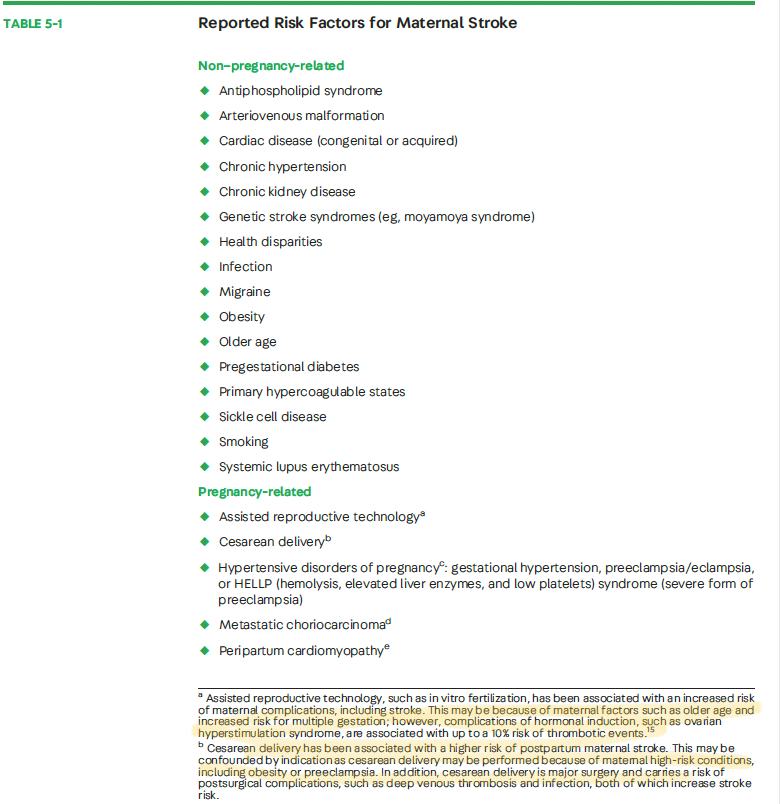
If you have a high-risk, comorbidity like hypertensive disorder of pregnany, the stroke incident may be as high as 1 in 500 deliveries.
PLUS, half of maternal strokes are hemorrhagic stroke: 👉carries a higher risk of morbidity
👉up to 50% are fatal.
If you have a high-risk, comorbidity like hypertensive disorder of pregnany, the stroke incident may be as high as 1 in 500 deliveries.
PLUS, half of maternal strokes are hemorrhagic stroke: 👉carries a higher risk of morbidity
👉up to 50% are fatal.
5/
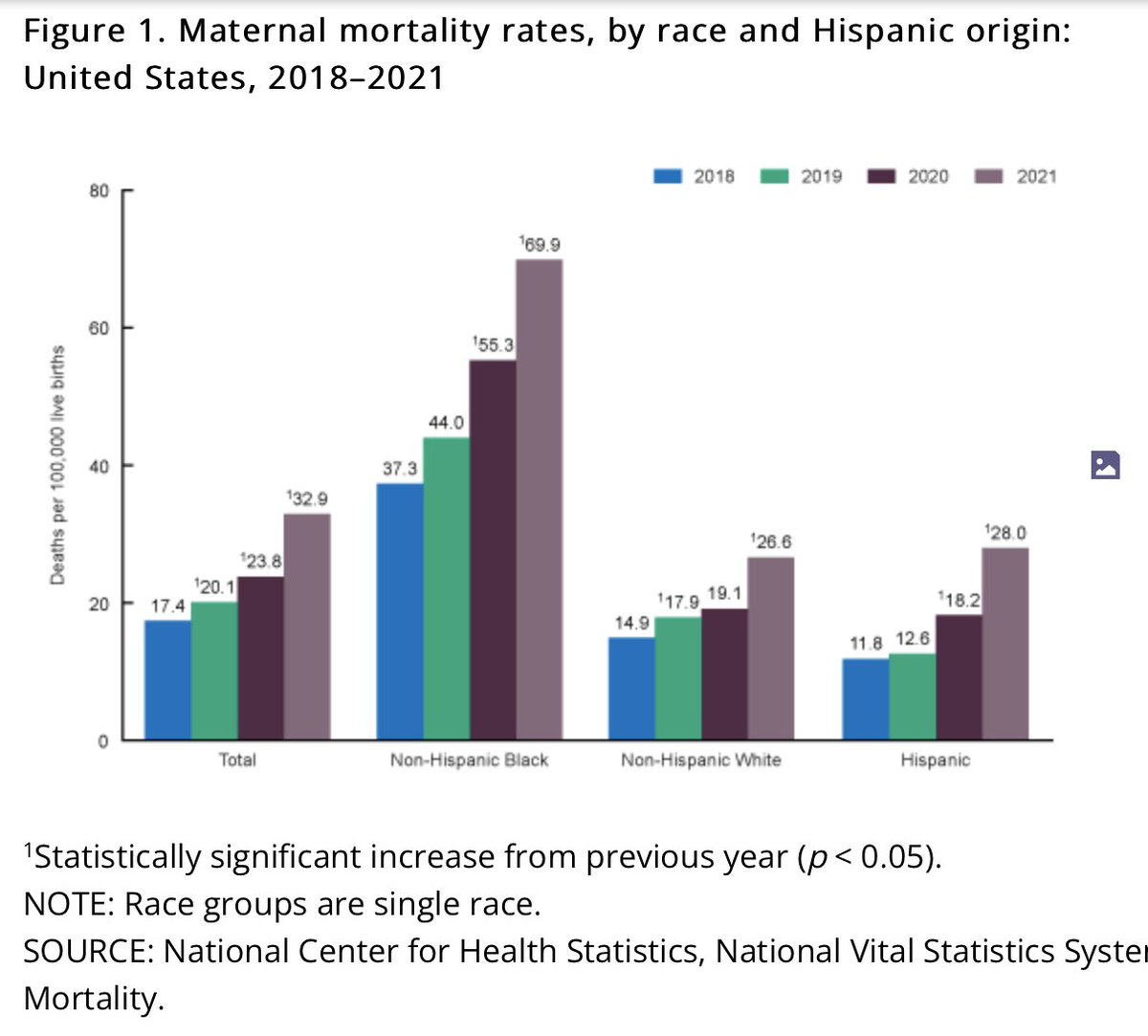
Stroke is associated with a 100-fold increase of maternal mortality.
100-fold.
And there is rampant disparity: Black women suffer the highest rate of material stroke regardless of socioeconomic status & comorbidities.
This is VERY not ok.
Stroke is associated with a 100-fold increase of maternal mortality.
100-fold.
And there is rampant disparity: Black women suffer the highest rate of material stroke regardless of socioeconomic status & comorbidities.
This is VERY not ok.
6/
And stroke rates are RISING🔼
Particularly in the postpartum period, which may in part be attributed to worsening health in women reflected in the rising rate in of risk factors, particularly obesity and HTN, as well as the trend to advancing maternal age.
Risk Factors:
And stroke rates are RISING🔼
Particularly in the postpartum period, which may in part be attributed to worsening health in women reflected in the rising rate in of risk factors, particularly obesity and HTN, as well as the trend to advancing maternal age.
Risk Factors:
7/
Although 'pregnancy' is the risk factor, most stroke occur AFTER delivery.
🩸First 2 weeks=highest risk period
🩸Maternal thromboembolic events & ICH remain definitively elevated for up to 12 weeks
& May be elevated for a full year after delivery! pubmed.ncbi.nlm.nih.gov
Although 'pregnancy' is the risk factor, most stroke occur AFTER delivery.
🩸First 2 weeks=highest risk period
🩸Maternal thromboembolic events & ICH remain definitively elevated for up to 12 weeks
& May be elevated for a full year after delivery! pubmed.ncbi.nlm.nih.gov

8/
Back to this case.
The patient had seizure like movements and was thought to have eclampsia.
But louder now, for the people in the back.
NOT ALL THAT SHAKES IS SEIZURE!
The availability of “loss of consciousness+hyperkinetic movement ”=“eclampsia” makes for an easy⚓️ point
Back to this case.
The patient had seizure like movements and was thought to have eclampsia.
But louder now, for the people in the back.
NOT ALL THAT SHAKES IS SEIZURE!
The availability of “loss of consciousness+hyperkinetic movement ”=“eclampsia” makes for an easy⚓️ point
9/
But -- if the eclamptic patient doesn’t rapidly return to baseline, they need a stat CT *AND* CTA!
⏰ CT for ?hemorrhage
⏰ CTA because nothing is worse than realizing too late that the altered patient has a basilar thrombus.
But -- if the eclamptic patient doesn’t rapidly return to baseline, they need a stat CT *AND* CTA!
⏰ CT for ?hemorrhage
⏰ CTA because nothing is worse than realizing too late that the altered patient has a basilar thrombus.
10/
Is this safe in pregnancy?
Yes.
👉Current CTs deliver up to 0.1mGy (far < 50 mGy threshold)
👉Contrast has a theoretic risk of neonatal hypothyroidism, but that risk is outweighed by the benefit of diagnosis acute stroke.
MRIs are also ok.
gadolinium = avoid if possible.
Is this safe in pregnancy?
Yes.
👉Current CTs deliver up to 0.1mGy (far < 50 mGy threshold)
👉Contrast has a theoretic risk of neonatal hypothyroidism, but that risk is outweighed by the benefit of diagnosis acute stroke.
MRIs are also ok.
gadolinium = avoid if possible.
11/
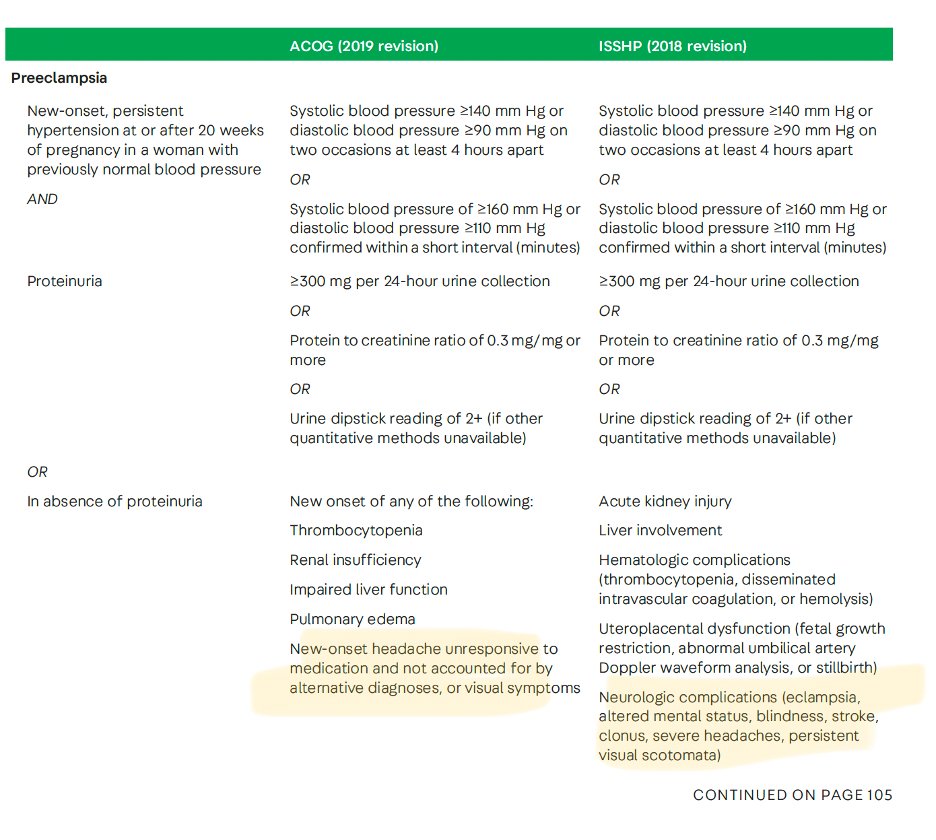
Back to our patient.
Hypertension (new dx) with a new-onset or different headache *is* pre-eclampsia whether they have proteinuria or not.
Back to our patient.
Hypertension (new dx) with a new-onset or different headache *is* pre-eclampsia whether they have proteinuria or not.
12/
Appropriately this patient was being admitted for IV magnesium therapy when the abrupt onset of AMS occurred (which would have still been indicated when ICH was discovered)
Beyond Mg, mgmt of ICH In a post-partum patient should focus on the basics:
🌬️Airway protection
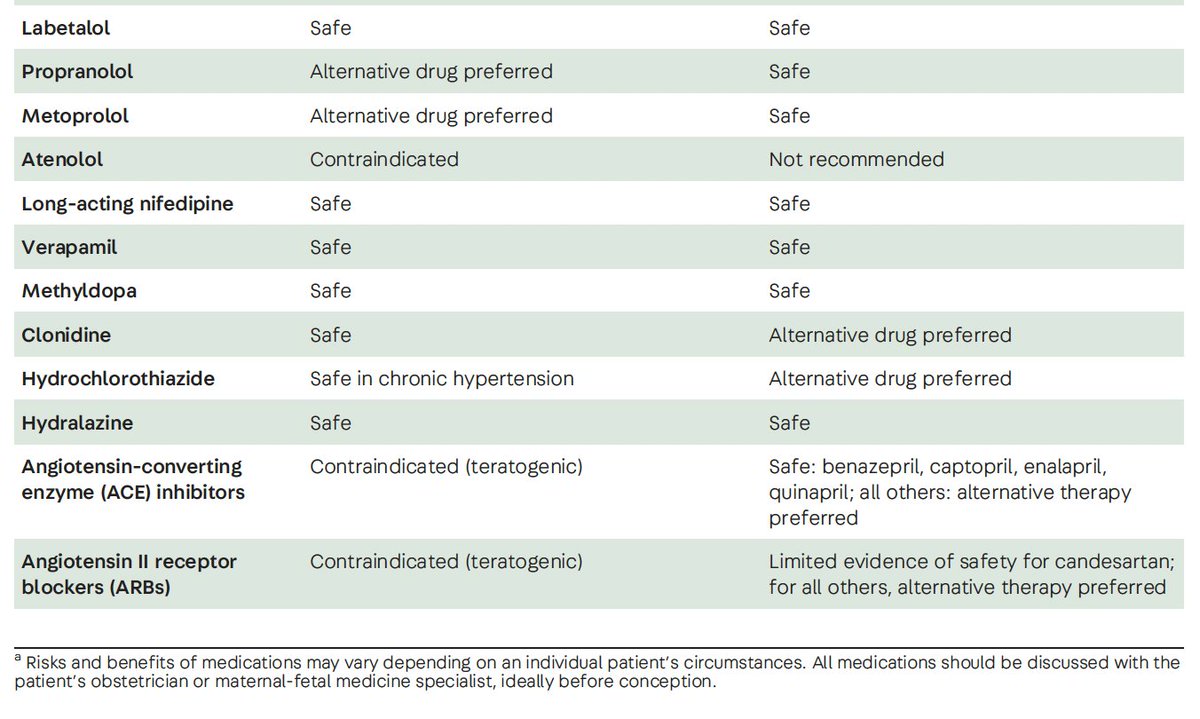
⏬ BP
Appropriately this patient was being admitted for IV magnesium therapy when the abrupt onset of AMS occurred (which would have still been indicated when ICH was discovered)
Beyond Mg, mgmt of ICH In a post-partum patient should focus on the basics:
🌬️Airway protection
⏬ BP
13/
what about hyperosmolar therapy?
Not a lot of data.
But, if the patient is still pregnant:
mannitol 0.25-0.5g/kg is considered safe
HTS can be considered but safety is less well established
what about hyperosmolar therapy?
Not a lot of data.
But, if the patient is still pregnant:
mannitol 0.25-0.5g/kg is considered safe
HTS can be considered but safety is less well established
14/
Hyperventilation can temporize... but it risks hypoperfusion of the fetus and fetal monitoring is highly recommended.
In general, whenever possible, a multidisciplinary approach should be taken to care for these patients with monitoring for mom and baby
Hyperventilation can temporize... but it risks hypoperfusion of the fetus and fetal monitoring is highly recommended.
In general, whenever possible, a multidisciplinary approach should be taken to care for these patients with monitoring for mom and baby

15/
There are so many awesome and informative @ContinuumAAN articles, but this one by @ElizaMillerMD is really a *standout* and these are complex, young patients. truly, a must read.
journals.lww.com
There are so many awesome and informative @ContinuumAAN articles, but this one by @ElizaMillerMD is really a *standout* and these are complex, young patients. truly, a must read.
journals.lww.com

Loading suggestions...