

1/5
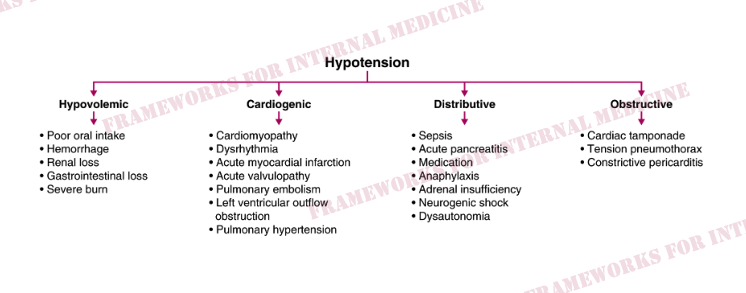
One of my favorite frameworks in #FrameworksForInternalMedicine.
Each main category of hypotension is associated with a unique mechanism, which makes it easy for our brains to file and recall this information.
And cardiac physiology is intuitive and fun.
One of my favorite frameworks in #FrameworksForInternalMedicine.
Each main category of hypotension is associated with a unique mechanism, which makes it easy for our brains to file and recall this information.
And cardiac physiology is intuitive and fun.
2/5
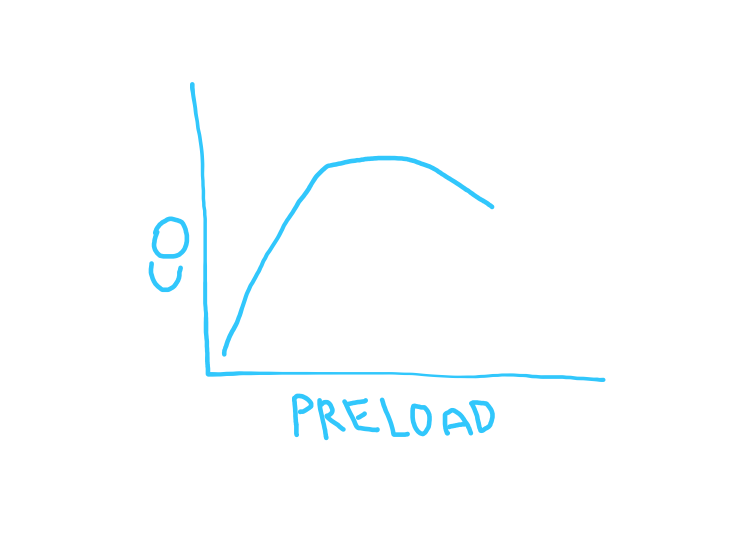
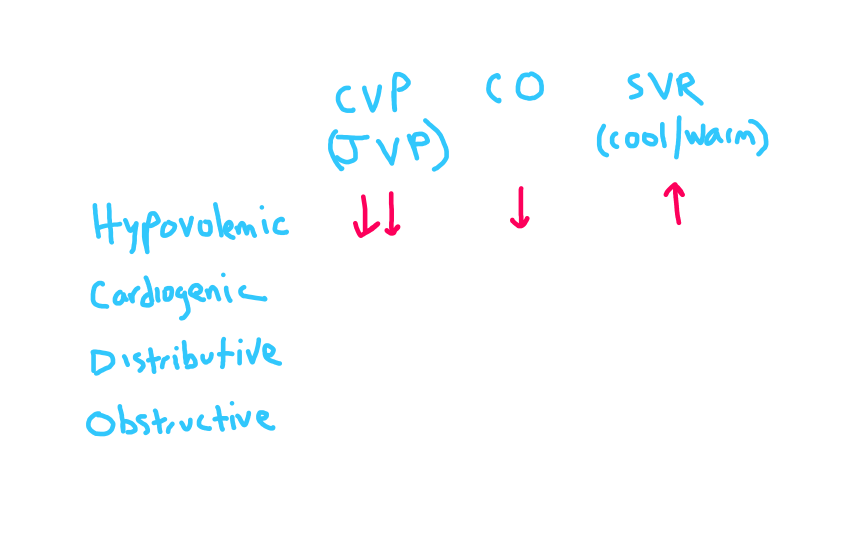
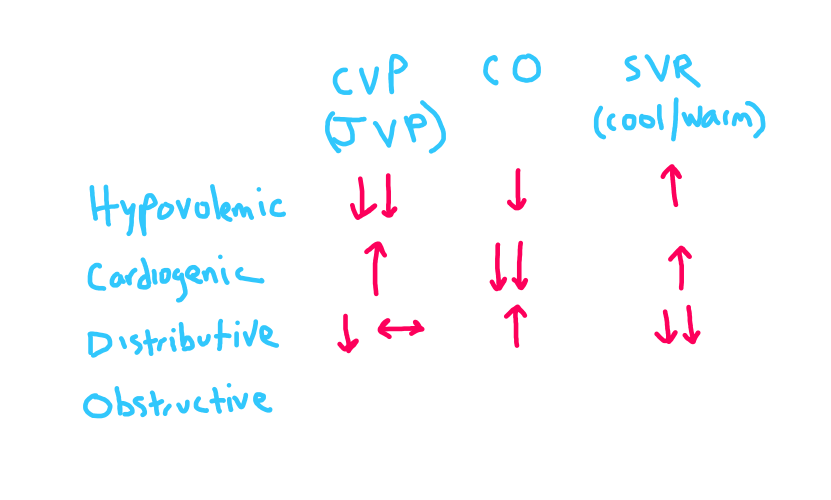
Hypovolemic hypotension occurs because of a decrease in preload. The pump is ready, the blood vessels are ready, but the "ammunition" is not there. JVP low, extremities cool.
2 arrows down for CVP/JVP since that is the primary issue.
Hypovolemic hypotension occurs because of a decrease in preload. The pump is ready, the blood vessels are ready, but the "ammunition" is not there. JVP low, extremities cool.
2 arrows down for CVP/JVP since that is the primary issue.
3/5
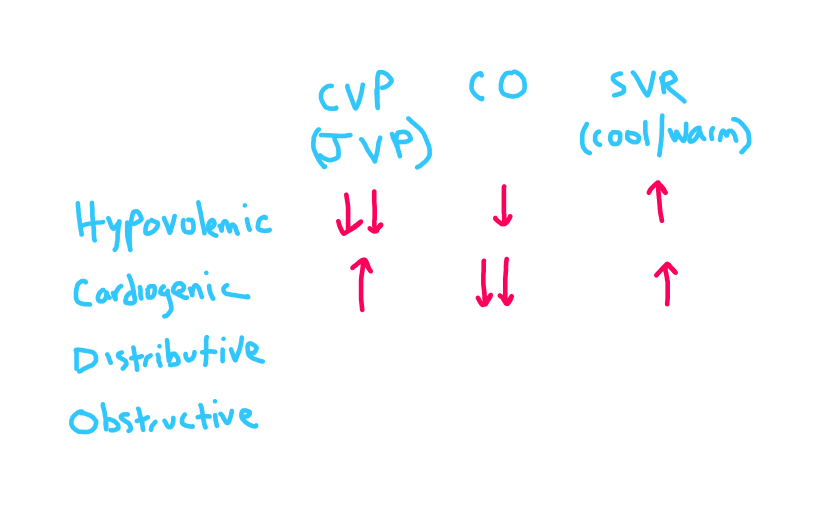
Cardiogenic hypotension occurs when the ammunition (preload) is there, the blood vessels are ready to go, but the pump is not working. JVP up, extremities cool.
2 down arrows for cardiac output (primary issue).
Cardiogenic hypotension occurs when the ammunition (preload) is there, the blood vessels are ready to go, but the pump is not working. JVP up, extremities cool.
2 down arrows for cardiac output (primary issue).
4/5
Distributive hypotension occurs when the ammunition is there, the pump is working, but the blood vessels are dilated/leaky and impossible to "fill" to generate pressure. Extremities warm w evidence of high output (eg, Quincke's pulse).
2 down arrows for SVR (primary issue).
Distributive hypotension occurs when the ammunition is there, the pump is working, but the blood vessels are dilated/leaky and impossible to "fill" to generate pressure. Extremities warm w evidence of high output (eg, Quincke's pulse).
2 down arrows for SVR (primary issue).
5/5
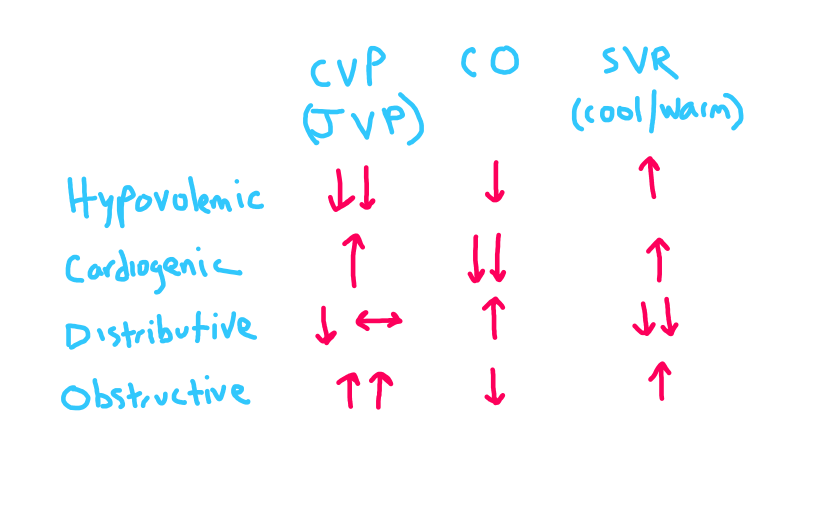
Obstructive hypotension occurs when the pump is working and the blood vessels are ready, but there is a mechanical impedance to RV filling.
2 up arrows for CVP/JVP (primary issue).
Obstructive hypotension occurs when the pump is working and the blood vessels are ready, but there is a mechanical impedance to RV filling.
2 up arrows for CVP/JVP (primary issue).
Here is an example of a patient with hypovolemic hypotension with very low CVP/JVP. She had low blood pressure with cool extremities.

Here is an example of a patient with distributive hypotension (from sepsis) with Quincke's pulse (evidence of high cardiac output). He also had warm extremities despite a low blood pressure.

Here is an example of a patient with obstructive hypotension from cardiac tamponade. Note the markedly elevated CVP/JVP. He had low BP with cool extremities.

Loading suggestions...