

1/
A 32 yo woman presents with headache and somnolence.
She is febrile to 102.6F.
Exam reveals neck stiffness and this rash…which, when your attending arrives, is absent #hatethat!
A #continuumcase @ContinuumAAN @LyellJ
A 32 yo woman presents with headache and somnolence.
She is febrile to 102.6F.
Exam reveals neck stiffness and this rash…which, when your attending arrives, is absent #hatethat!
A #continuumcase @ContinuumAAN @LyellJ

2/
Rashes can be a sign of many neurocutaneous disorders & infectious etiologies.
High fever + neck stiffness + a rash=🔼 concern for neisseria meningococcal meningitis
However, the rash in meningococcal meningitis is often caused by DIC, looks more like this & doesn't vanish
Rashes can be a sign of many neurocutaneous disorders & infectious etiologies.
High fever + neck stiffness + a rash=🔼 concern for neisseria meningococcal meningitis
However, the rash in meningococcal meningitis is often caused by DIC, looks more like this & doesn't vanish

3/
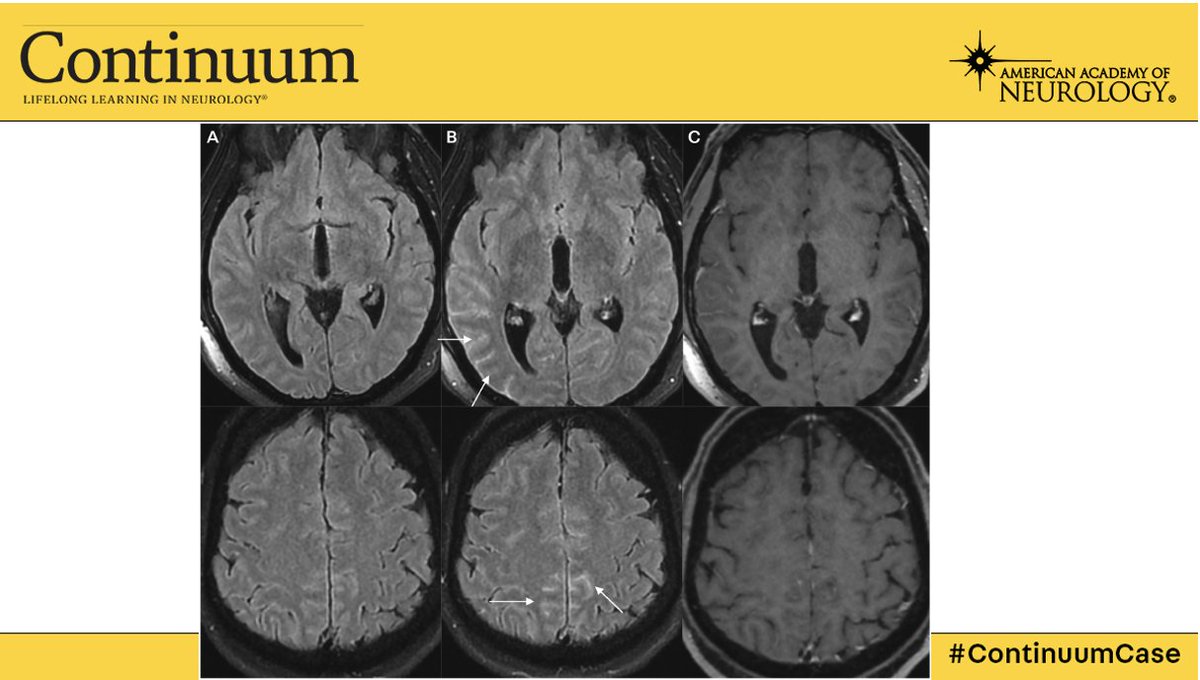
Still, there’s a high concern for infectious meningitis and an LP is performed, which demonstrates a neutrophilic pleocytosis and hypoglycorrhachia and an elevated opening pressure.
MRI confirms Leptomeningeal enhancement and flair non-suppression.
Still, there’s a high concern for infectious meningitis and an LP is performed, which demonstrates a neutrophilic pleocytosis and hypoglycorrhachia and an elevated opening pressure.
MRI confirms Leptomeningeal enhancement and flair non-suppression.
4/
Case closed this is a bacterial thing, right?
Case closed this is a bacterial thing, right?

5/
I agree! All of this seems highly supportive of a bacterial process, but extensive workup with biofire, cultures, TB testing is non-revealing. RPR is negative. Lyme testing negative.
Those tricky culture-neg organisms like coxiella, bartonella are sought with antibody testing
I agree! All of this seems highly supportive of a bacterial process, but extensive workup with biofire, cultures, TB testing is non-revealing. RPR is negative. Lyme testing negative.
Those tricky culture-neg organisms like coxiella, bartonella are sought with antibody testing
6/
Nothing.
Fungal etiologies are evaluated for and screened for and nothing comes back positive.
Nothing.
Fungal etiologies are evaluated for and screened for and nothing comes back positive.
7/
Hypoglycorrhachia, but culture negative….🤔🤔🤔
✨ Is this a malignant neoplastic process?
🔥 Is this sarcoid?
Hypoglycorrhachia, but culture negative….🤔🤔🤔
✨ Is this a malignant neoplastic process?
🔥 Is this sarcoid?
8/
In favor of malignancy:
Further history reveals she’s had daily fevers and chills for over 3 weeks.
But, multiple CSF evaluations fail to show a clonal population and imaging reveals hepatosplenomegaly.... but no lymphadenopathy.
Manual diff & serum flow cytometry...nothing
In favor of malignancy:
Further history reveals she’s had daily fevers and chills for over 3 weeks.
But, multiple CSF evaluations fail to show a clonal population and imaging reveals hepatosplenomegaly.... but no lymphadenopathy.
Manual diff & serum flow cytometry...nothing
9/
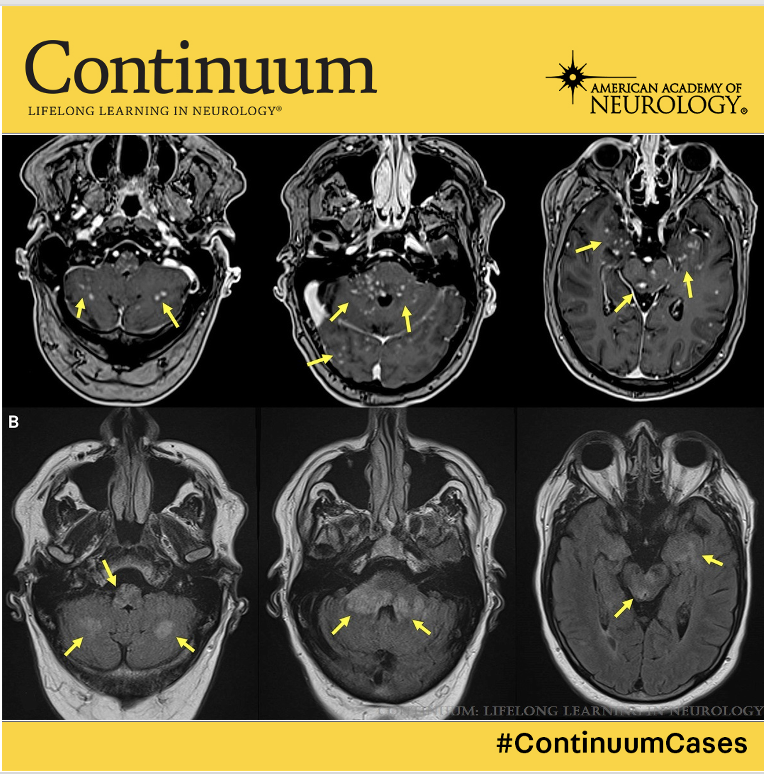
For sarcoid: no lymphadenopathy and the distribution of meningeal enhancement is highly atypical for sarcoid meningitis, which is often pachymeningitis or leptomeningitis at the basal cisterns, or this scattershot nodular pattern:
For sarcoid: no lymphadenopathy and the distribution of meningeal enhancement is highly atypical for sarcoid meningitis, which is often pachymeningitis or leptomeningitis at the basal cisterns, or this scattershot nodular pattern:
10/
What else can cause aseptic meningitis with hypoglycorrhachia??
All drugs are stopped.
The cyclic fever persists... and with it the evanescent “salmon-colored” rash continues.
What else can cause aseptic meningitis with hypoglycorrhachia??
All drugs are stopped.
The cyclic fever persists... and with it the evanescent “salmon-colored” rash continues.
11/
She complains of worsening joint pain.
More lab testing reveals:
👆 An elevated ferritin (600)
👉mild transaminitis.
She complains of worsening joint pain.
More lab testing reveals:
👆 An elevated ferritin (600)
👉mild transaminitis.
12/
What *IS* this?
What *IS* this?
13/
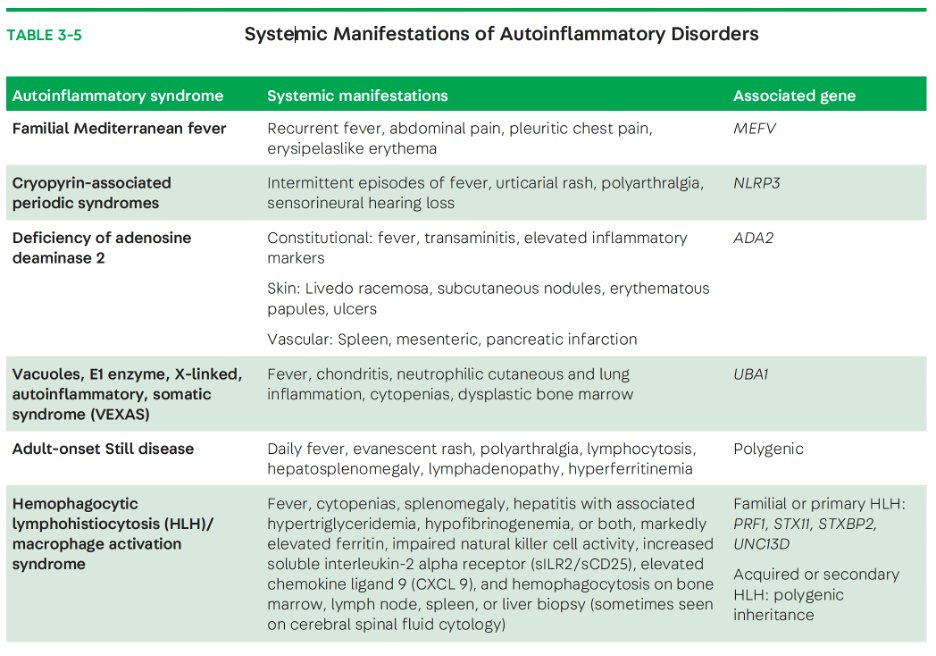
Honestly, all of these could be good thoughts, and fall into the bucket of Autoinflammatory Disorders.
Some have an associated gene and are inherited. Others are acquired.
Many of these conditions are associated with aseptic meningitis.
Honestly, all of these could be good thoughts, and fall into the bucket of Autoinflammatory Disorders.
Some have an associated gene and are inherited. Others are acquired.
Many of these conditions are associated with aseptic meningitis.
14/
Adult Onset Stills (AOS), HLH and VEXAS are all acquired autoinflammatory syndromes.
AOS is characterized by
- Daily fevers
- Evanescent rash
- Elevated inflammatory markers
- Hyperferritinemia
Adult Onset Stills (AOS), HLH and VEXAS are all acquired autoinflammatory syndromes.
AOS is characterized by
- Daily fevers
- Evanescent rash
- Elevated inflammatory markers
- Hyperferritinemia
15/
Neurologic manifestations accompany less than 10% of cases. But may be aseptic meningitis, encephalitis, & ischemic stroke.
Ultimately, the patient was diagnosed with AOS and tx'ed w/ steroids.
There is mounting evidence for anakinra and IL-6 inhibitors like tocilizumab.
Neurologic manifestations accompany less than 10% of cases. But may be aseptic meningitis, encephalitis, & ischemic stroke.
Ultimately, the patient was diagnosed with AOS and tx'ed w/ steroids.
There is mounting evidence for anakinra and IL-6 inhibitors like tocilizumab.
16/
This case emphasizes the need to consider acquired and familial systemic auto-inflammatory syndromes. These cases are 🦓 & their diagnosis can be a challenge!!
This case emphasizes the need to consider acquired and familial systemic auto-inflammatory syndromes. These cases are 🦓 & their diagnosis can be a challenge!!
17/
They are often associated with high inflammatory markers and may be found when the workup for infectious and neoplastic processes is unrevealing.
They are often associated with high inflammatory markers and may be found when the workup for infectious and neoplastic processes is unrevealing.
18/
There is a great discussion about HLH and VEXAS in this article of @continuumAAN by Dr. Toledo. This is the FREE article!! There is no excuse not to check it out!!
journals.lww.com
There is a great discussion about HLH and VEXAS in this article of @continuumAAN by Dr. Toledo. This is the FREE article!! There is no excuse not to check it out!!
journals.lww.com
19/
Truly, I think this would have been a very challenging diagnosis to make... would love to hear what others would have considered @Capt_Ammonia @CajalButterfly @sigman_md @rkchoi @AaronLBerkowitz @PulmCrit @LyellJ @bobvarkey @JimSiegler @namorrismd @drdangayach
Truly, I think this would have been a very challenging diagnosis to make... would love to hear what others would have considered @Capt_Ammonia @CajalButterfly @sigman_md @rkchoi @AaronLBerkowitz @PulmCrit @LyellJ @bobvarkey @JimSiegler @namorrismd @drdangayach
Loading suggestions...