

📢Tweetorial alert #NephTwitter
Autosomal dominant polycystic kidney disease (ADPKD) is estimated to affect 1:1000 individuals worldwide.
Diagnosis can be made by imaging 🩻 or genetic testing 🧬.
But what are the best prognostic indicators of severe disease?
Let's go...
Autosomal dominant polycystic kidney disease (ADPKD) is estimated to affect 1:1000 individuals worldwide.
Diagnosis can be made by imaging 🩻 or genetic testing 🧬.
But what are the best prognostic indicators of severe disease?
Let's go...
ADPKD outcomes are most closely correlated with:
ADPKD
The answer is choice 2.
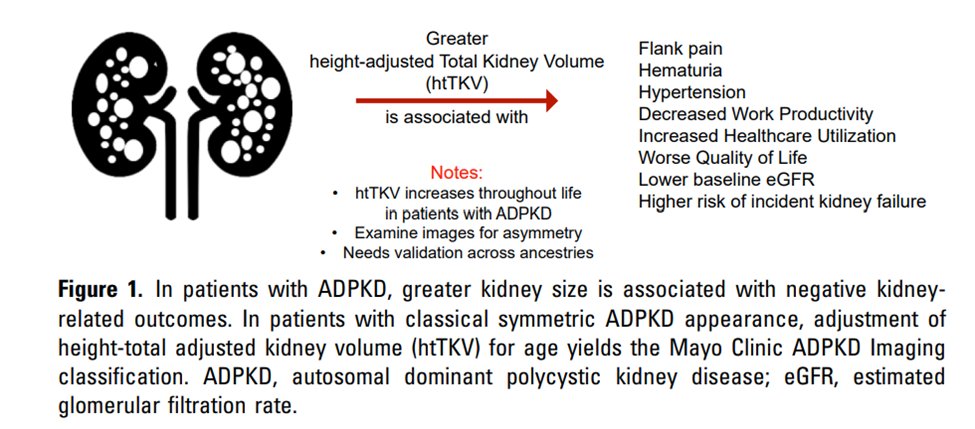
Height-adjusted total kidney volume (htTKV) is associated with ⬇️ eGFR, but also with:
Hematuria
Hypertension
Pain
⬆️health care utilization
⬇️work productivity
Worse patient-reported quality of life (QoL)
kireports.org
The answer is choice 2.
Height-adjusted total kidney volume (htTKV) is associated with ⬇️ eGFR, but also with:
Hematuria
Hypertension
Pain
⬆️health care utilization
⬇️work productivity
Worse patient-reported quality of life (QoL)
kireports.org

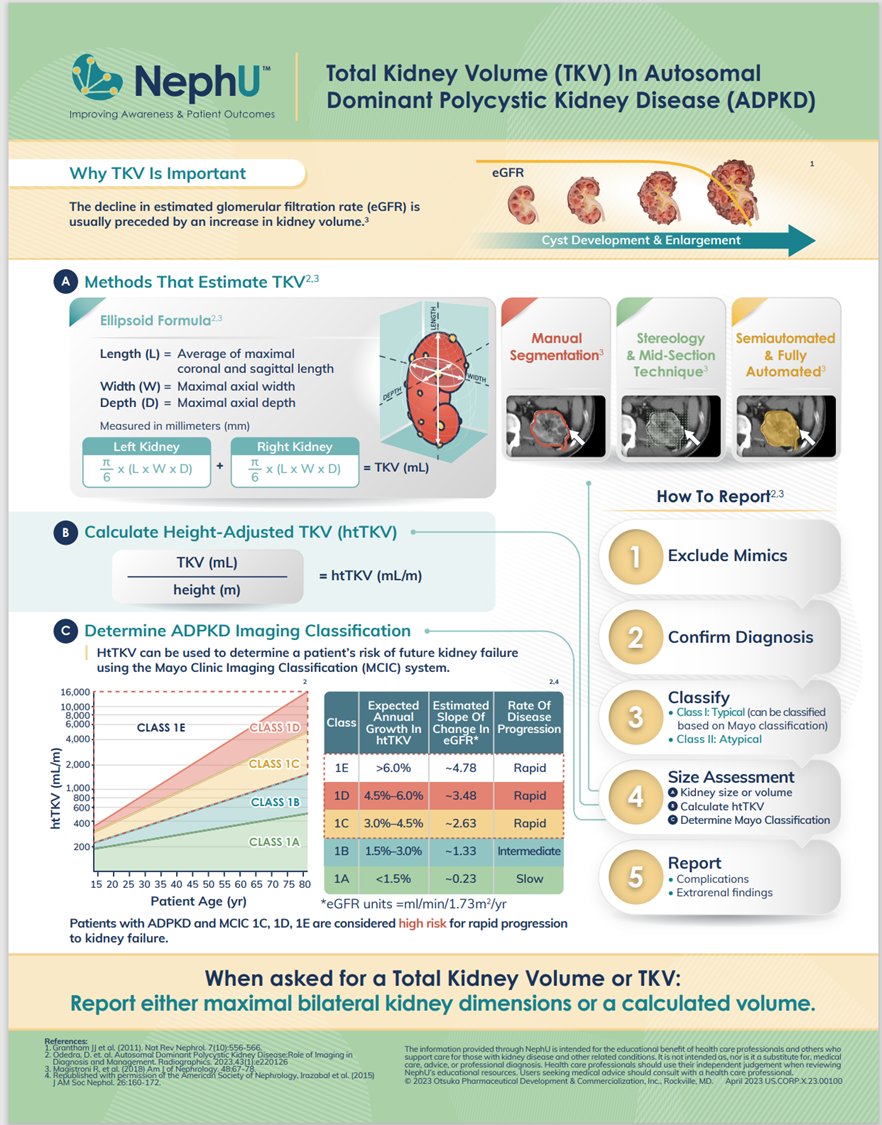
htTKV
Calculated from the patient's height and the height, width and depth measured on imaging (MRI preferred). The Mayo Clinic ADPKD imaging classifications (A-E) can be used to risk stratify patient's for developing ESKD.
qxmd.com
Calculated from the patient's height and the height, width and depth measured on imaging (MRI preferred). The Mayo Clinic ADPKD imaging classifications (A-E) can be used to risk stratify patient's for developing ESKD.
qxmd.com
Mayo Classification
Classes are based on htTKV growth/yr.
Pts tend to stay on trend lines & repeat imaging isn’t recommended unless there’s a significant change in disease course (eGFR).
However, there can be variability in htKTV due to imaging techniques. @NephUCommunity
Classes are based on htTKV growth/yr.
Pts tend to stay on trend lines & repeat imaging isn’t recommended unless there’s a significant change in disease course (eGFR).
However, there can be variability in htKTV due to imaging techniques. @NephUCommunity
ADPKD
Pts with ⬆️risk (Mayo class C-E) have ⬆️potential to benefit from treatment.
Tolvaptan slows the rate of htTKV, but the kidneys irrevocably continue to grow.
Let’s look at the studies 🎶: TEMPO, REPRISE and now OVERTURE.
VA by @drpriyajohn
kireports.org
Pts with ⬆️risk (Mayo class C-E) have ⬆️potential to benefit from treatment.
Tolvaptan slows the rate of htTKV, but the kidneys irrevocably continue to grow.
Let’s look at the studies 🎶: TEMPO, REPRISE and now OVERTURE.
VA by @drpriyajohn
kireports.org

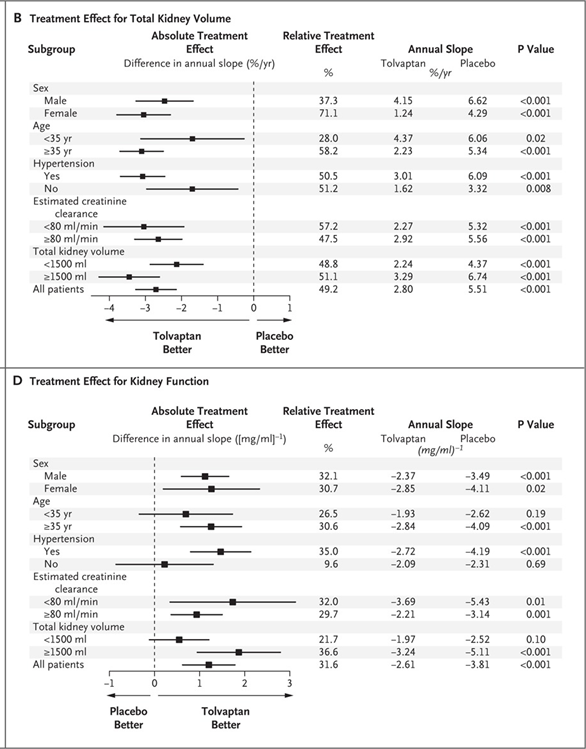
TEMPO 3:4
Tolvaptan slowed⬆️ in TKV & decline in eGFR vs placebo over a 3-year period in ADPKD. Higher discontinuation rate in the treatment arm due to adverse events. Risk of liver toxicity. Cost of medication can also be a barrier.
Fig 2 from paper:
nejm.org
Tolvaptan slowed⬆️ in TKV & decline in eGFR vs placebo over a 3-year period in ADPKD. Higher discontinuation rate in the treatment arm due to adverse events. Risk of liver toxicity. Cost of medication can also be a barrier.
Fig 2 from paper:
nejm.org

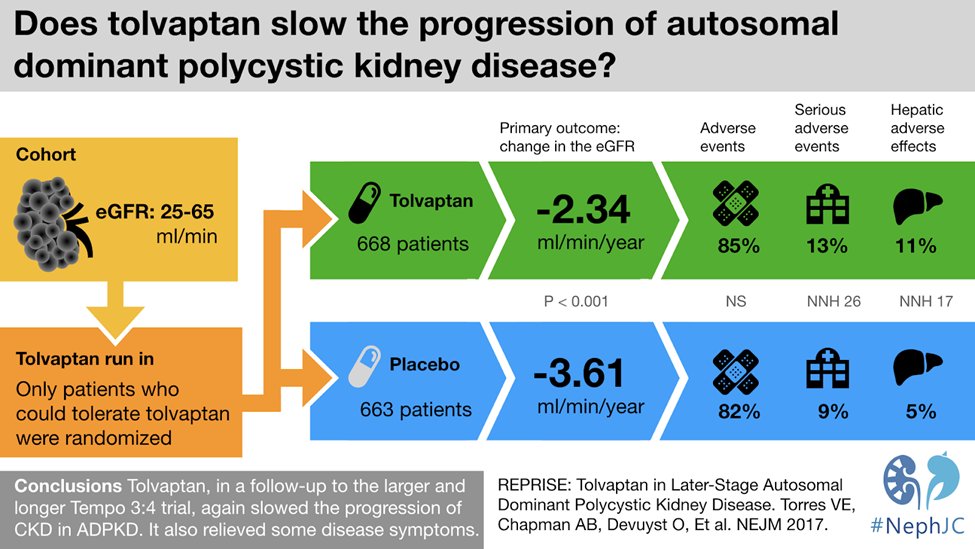
REPRISE
ADPKD with eGFR of 25- 44 ml/min.
⬇️eGFR −2.34 ml/min in tolvaptan group vs −3.61 ml/min in placebo group (difference, 1.27 ml/min/1.73 m2; 95% CI, 0.86 to 1.68; P<0.001).
Tolvaptan resulted in a slower decline than placebo in eGFR at 1-year.
nejm.org
ADPKD with eGFR of 25- 44 ml/min.
⬇️eGFR −2.34 ml/min in tolvaptan group vs −3.61 ml/min in placebo group (difference, 1.27 ml/min/1.73 m2; 95% CI, 0.86 to 1.68; P<0.001).
Tolvaptan resulted in a slower decline than placebo in eGFR at 1-year.
nejm.org

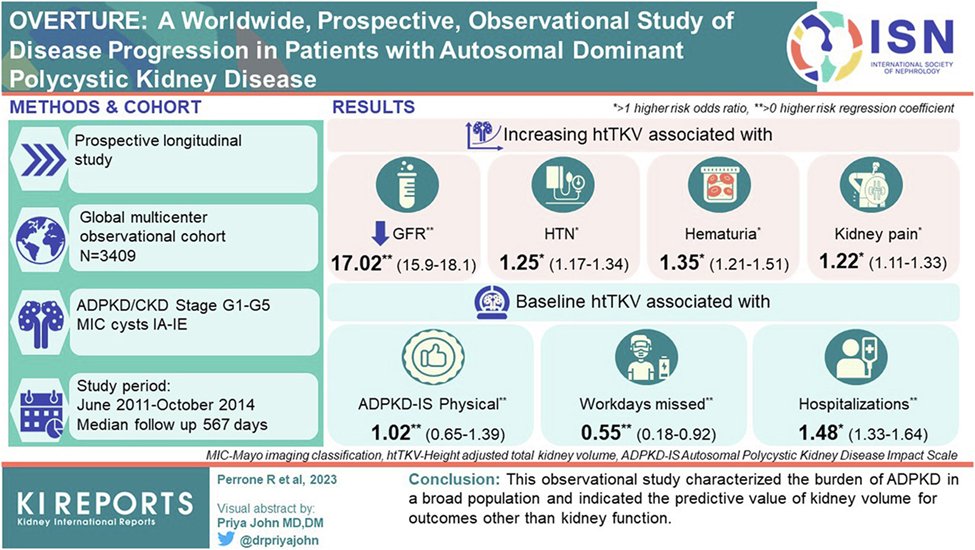
OVERTURE
3409 ADPKD pts, 285 sites, 20 countries!
Observational, longitudinal study.
1° objective was to investigate association of TKV with ADPKD-related outcomes.
2° objectives focused on disease-specific patient-reported outcomes, QoL, healthcare utilization & productivity.
3409 ADPKD pts, 285 sites, 20 countries!
Observational, longitudinal study.
1° objective was to investigate association of TKV with ADPKD-related outcomes.
2° objectives focused on disease-specific patient-reported outcomes, QoL, healthcare utilization & productivity.
OVERTURE
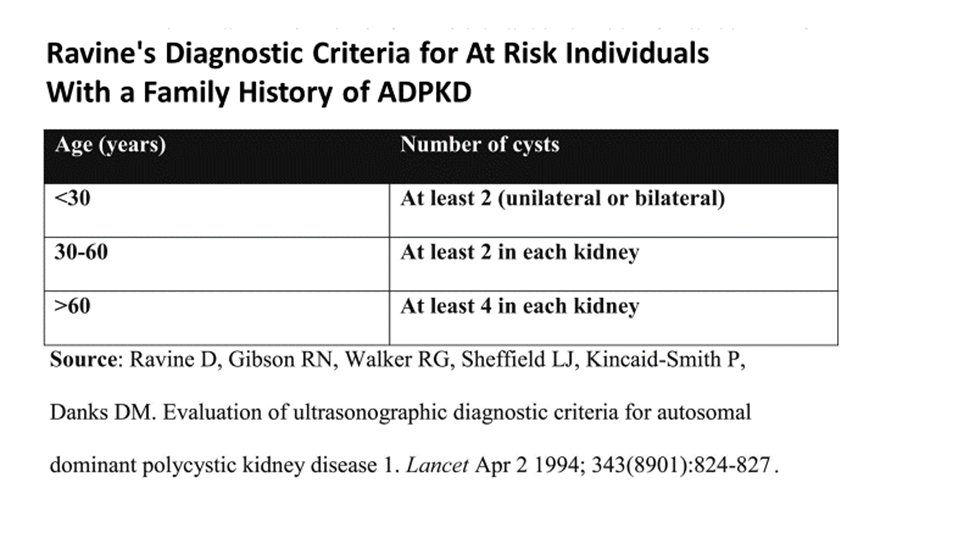
12-70 years old dx by modified Ravine criteria.
htTKV >300 ml/m height by ultrasound or >250 ml/m height by MRI (within 1 year prior to baseline).
Pts with current or expected treatment of ADPKD affecting TKV were excluded without the prior approval of the sponsor.
12-70 years old dx by modified Ravine criteria.
htTKV >300 ml/m height by ultrasound or >250 ml/m height by MRI (within 1 year prior to baseline).
Pts with current or expected treatment of ADPKD affecting TKV were excluded without the prior approval of the sponsor.
OVERTURE
Study visits took place at baseline, 6, 12 and 18 months, and every 6 months thereafter for up to 36 months.
Significant drop in kidney function was defined as dialysis, transplant or doubling of serum creatinine from baseline.
Study visits took place at baseline, 6, 12 and 18 months, and every 6 months thereafter for up to 36 months.
Significant drop in kidney function was defined as dialysis, transplant or doubling of serum creatinine from baseline.

OVERTURE
Enrolled patients: 422 in Asia Pacific, 1355 in Europe, 1373 in North America, and 259 in South America.
Median follow up 567 days.
84% completed a 12-month visit and MRI.
65% had Mayo Class C-E.
Mean eGFR at enrollment was 69 ml/min.
56% were female and 86% were white.
Enrolled patients: 422 in Asia Pacific, 1355 in Europe, 1373 in North America, and 259 in South America.
Median follow up 567 days.
84% completed a 12-month visit and MRI.
65% had Mayo Class C-E.
Mean eGFR at enrollment was 69 ml/min.
56% were female and 86% were white.

OVERTURE
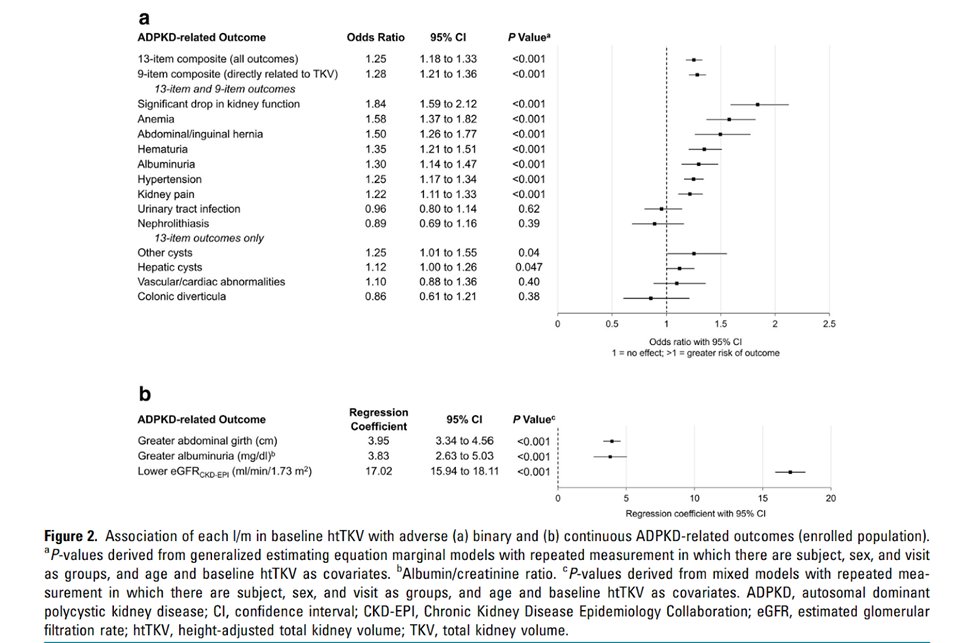
Higher baseline measured htTKV was associated with worse ADPKD-related clinical outcomes in almost all measures (Fig 2a).
Higher htTKV was also associated with worse continuous clinical outcomes (Fig 2b): abdominal girth, albumin-to-creatinine ratio & eGFR.
Higher baseline measured htTKV was associated with worse ADPKD-related clinical outcomes in almost all measures (Fig 2a).
Higher htTKV was also associated with worse continuous clinical outcomes (Fig 2b): abdominal girth, albumin-to-creatinine ratio & eGFR.
OVERTURE
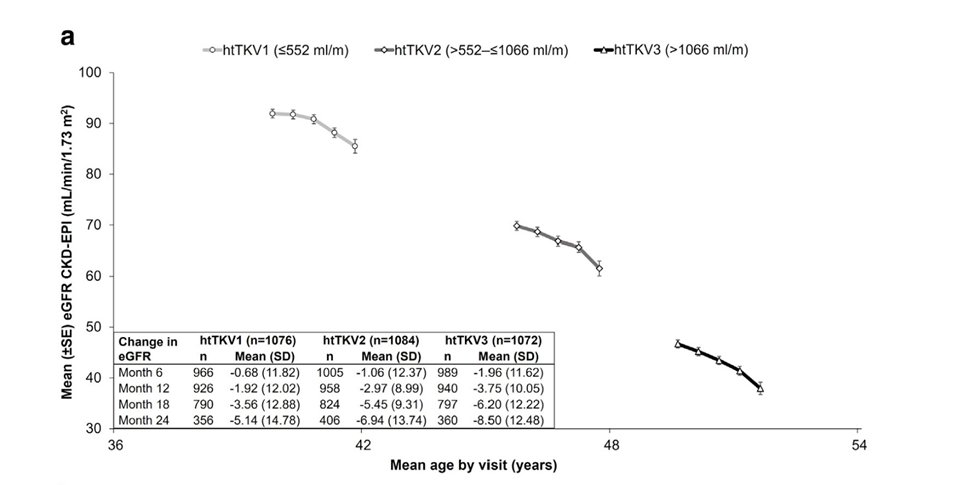
Mean(SD) TKV growth was 6.2% (7.9) from baseline to 12 months.
Δ mean baseline eGFR by baseline htTKV tertile:
1st (≤ 552 ml/m): 91.9 ml/min, mean(SD) -1.9 (12) ml/min/yr eGFR
2nd (>552 to ≤1066 ml/m): 69.8 ml/min , -3.0 (9.0)
3rd (>1066 ml/m): 46.7 ml/min, -3.8 (10.1)
Mean(SD) TKV growth was 6.2% (7.9) from baseline to 12 months.
Δ mean baseline eGFR by baseline htTKV tertile:
1st (≤ 552 ml/m): 91.9 ml/min, mean(SD) -1.9 (12) ml/min/yr eGFR
2nd (>552 to ≤1066 ml/m): 69.8 ml/min , -3.0 (9.0)
3rd (>1066 ml/m): 46.7 ml/min, -3.8 (10.1)
OVERTURE
eGFR decline (over 24 months) associated with:
Higher htKTV
Lower eGFR baseline
Higher Mayo Classification (E>>B)
High htKTV was also associated with worse scores on multiple measures of patient-reported QoL, productivity, physical function & healthcare utilization.
eGFR decline (over 24 months) associated with:
Higher htKTV
Lower eGFR baseline
Higher Mayo Classification (E>>B)
High htKTV was also associated with worse scores on multiple measures of patient-reported QoL, productivity, physical function & healthcare utilization.
Limitations
Short follow up: 1-year for TKV & up to 3 years for other outcomes.
Study population was largely in early stages of CKD.
Predominantly European ancestry, with only 3% Black or African-American pts.
Few class 2 (atypical, unilateral) Mayo class pts.
Short follow up: 1-year for TKV & up to 3 years for other outcomes.
Study population was largely in early stages of CKD.
Predominantly European ancestry, with only 3% Black or African-American pts.
Few class 2 (atypical, unilateral) Mayo class pts.
OVERTURE
Data were consistent with the CRISP cohort. The OVERTURE data extended the CRISP findings from a young, high eGFR population, to a global cross-section of pts with ADPKD at different ages and stages of CKD.
journals.lww.com
Data were consistent with the CRISP cohort. The OVERTURE data extended the CRISP findings from a young, high eGFR population, to a global cross-section of pts with ADPKD at different ages and stages of CKD.
journals.lww.com

OVERTURE
It should be noted, the relationship of htTKV to eGFR decline was attenuated in subjects at low risk of rapid progression (Mayo class 1A–1B). This finding is consistent with data from the Mayo Clinic that htTKV has an inverse correlation with pt age at ESKD.
It should be noted, the relationship of htTKV to eGFR decline was attenuated in subjects at low risk of rapid progression (Mayo class 1A–1B). This finding is consistent with data from the Mayo Clinic that htTKV has an inverse correlation with pt age at ESKD.
OVERTURE
Where cystic expansion appears to be the predominant factor in declining eGFR among rapidly progressing patients, other factors such as vascular disease and interstitial fibrosis, may play a greater role in declining eGFR in patients who progress slowly.
Where cystic expansion appears to be the predominant factor in declining eGFR among rapidly progressing patients, other factors such as vascular disease and interstitial fibrosis, may play a greater role in declining eGFR in patients who progress slowly.
FIN
This has been @brian_rifkin with another KI Reports tweetorial. Thanks @sophia_kidney @NephroSeeker.
Thanks to authors: @doberdhan, @persimmonblue, @ABCrenalarena
Want more?
You can read the commentary on this study from @MattLanktree
kireports.org
This has been @brian_rifkin with another KI Reports tweetorial. Thanks @sophia_kidney @NephroSeeker.
Thanks to authors: @doberdhan, @persimmonblue, @ABCrenalarena
Want more?
You can read the commentary on this study from @MattLanktree
kireports.org
Loading suggestions...