
My talk at #ApExPathshala on #AcidBase had some new (to me information) on urine anion gap. I want to share it but to get there we need to discuss renal acid handling. #Tweetorial #Physiology #Electrolytes 1/11

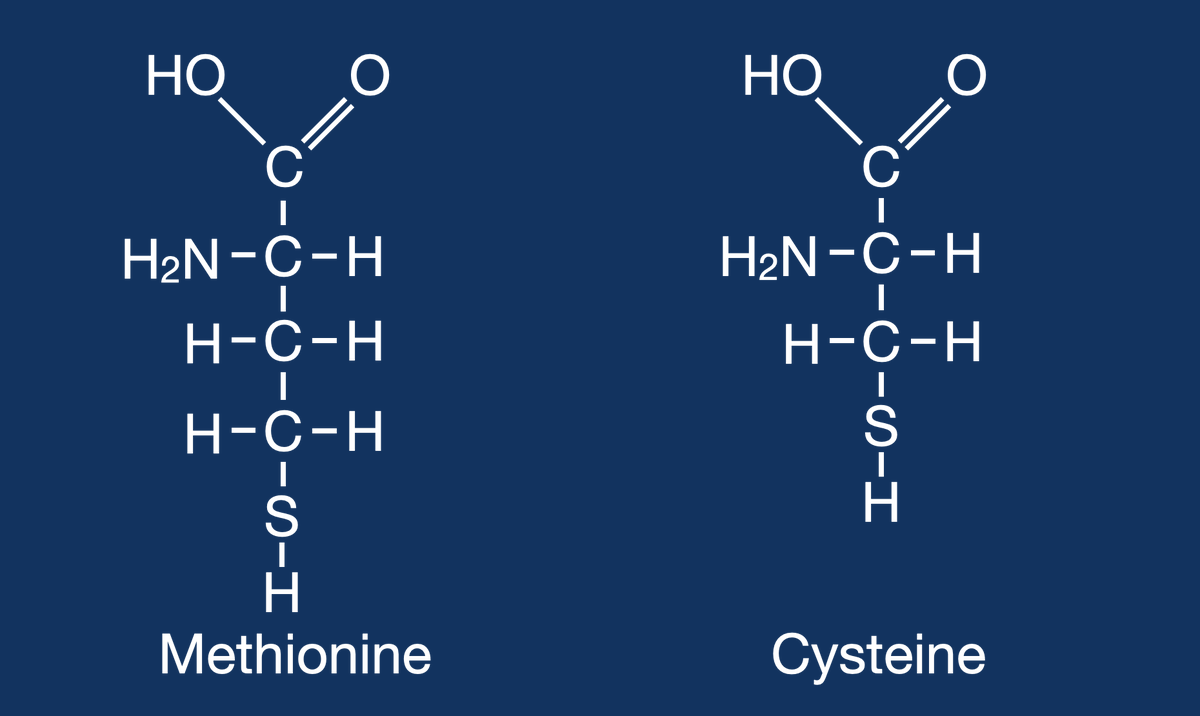
Metabolizing proteins, specifically the sulfur containing amino acids, methionine and cysteine, generates hydrogen sulfide (H2S). This acid cannot be cleared by the lungs. #OnlyTheKidneys can clear this acid. 2/11
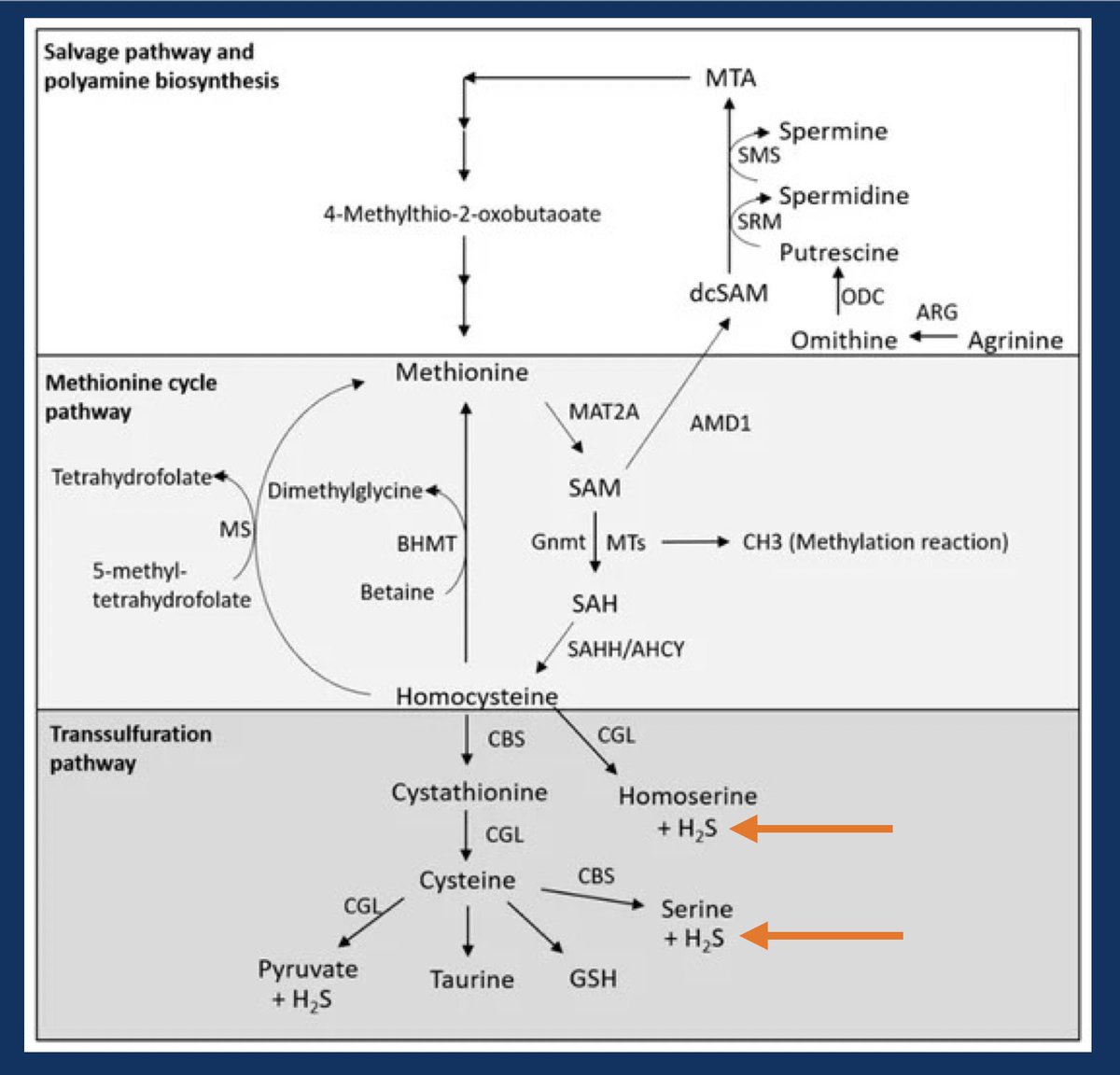
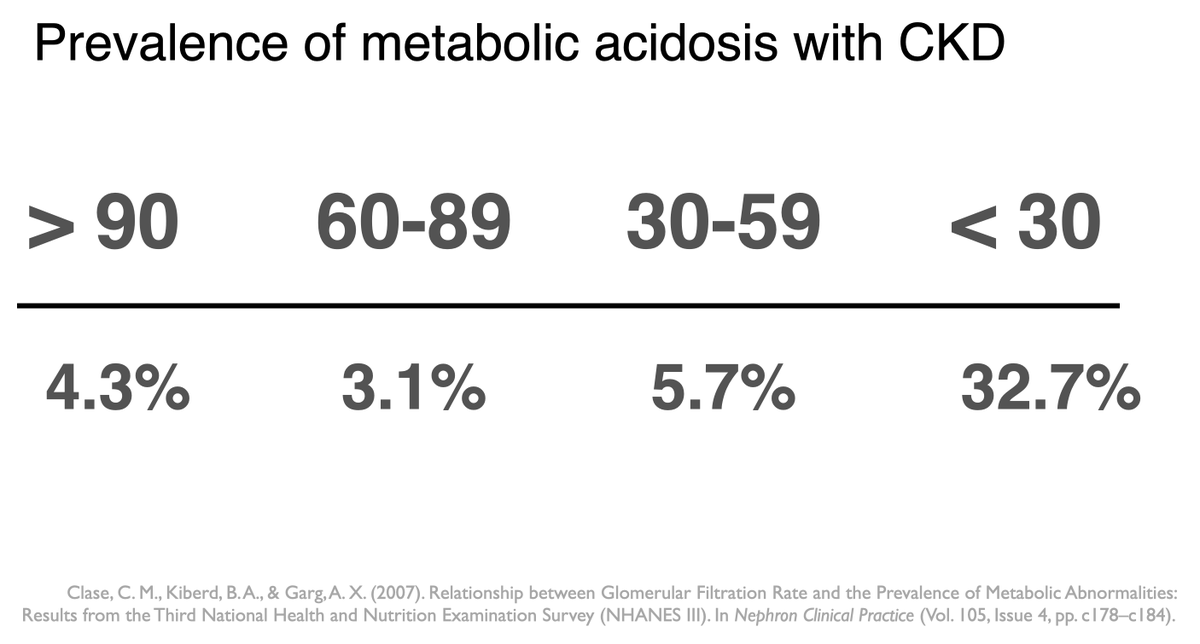
This acid load, generated by normal metabolism that must be excreted by the kidneys is the daily acid load. When patients with advanced CKD develop progressive metabolic acidosis it is because they are failing to clear the daily acid load. 3/11
On a “western diet” (I.e. carnivorous diet) it is about 50-100 mEq of acid (H+ ions) a day. 4/11
Boy it would be easy if we could excrete this as free hydrogen ions, alas that would require a urine pH of around 1 (50 mEq H+ in 2 liters of urine). At a minimal urine pH of 4.5, we would need to make 1200 liters of urine a day to clear the daily acid load. 5/11
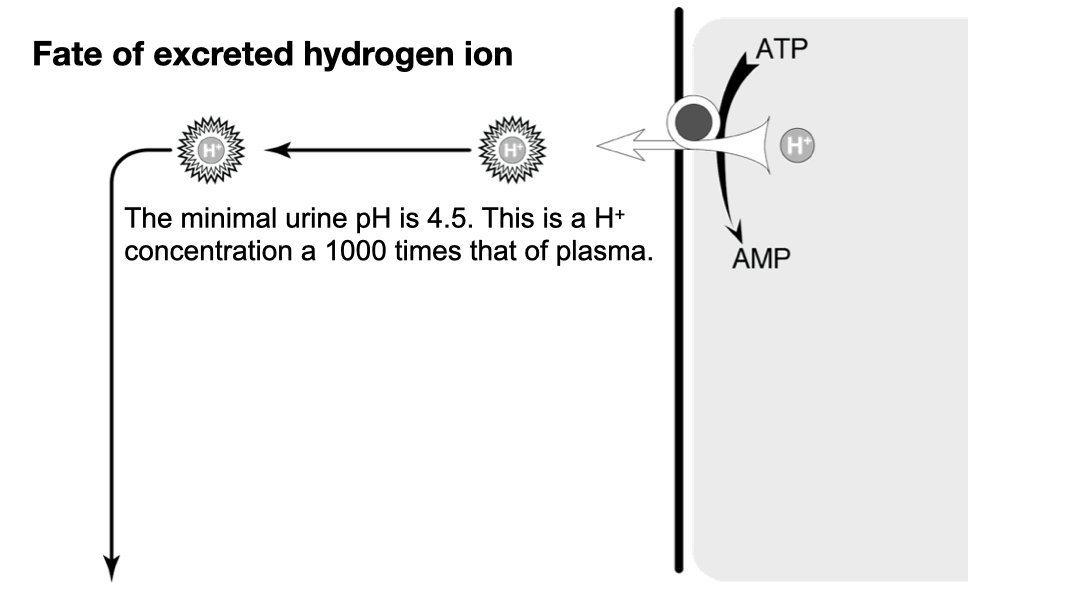
So the kidney has to smuggle the hydrogen out as something other than free hydrogen. There are two solutions to this:
1) Titratable Acid
2) Ammonium (NH4+)
6/11
1) Titratable Acid
2) Ammonium (NH4+)
6/11
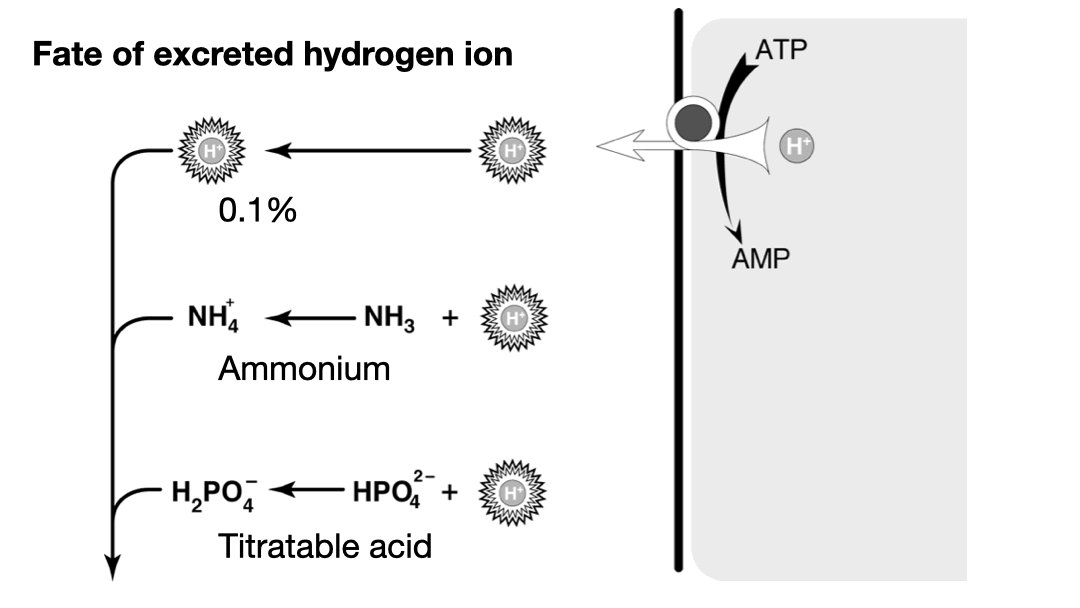
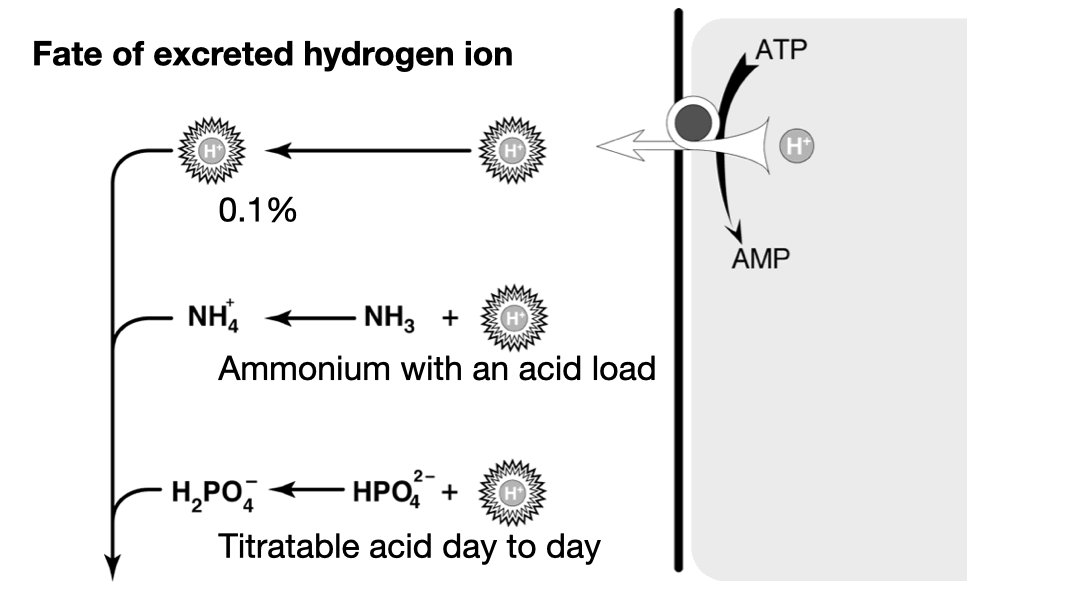
Titratable acid is just H2PO4–. Most of the daily acid load is excreted this way. The problem is that it is fixed by phosphate intake. We cannot manufacture new phosphate when we encounter a large acid load, so we cannot ramp up titratable acid to deal with an acid load.** 7/11
**Actually that is not entirely true. In addition to the serum bicarbonate, the bones are called upon to buffer an acid load. And as they are dissolved buffering acid (not an ideal state) they release phosphate which clears the acid from the body. pubmed.ncbi.nlm.nih.gov 8/11

So when faced with a large acid load we call on system two: ammonium. The physiologists have two models for how this works. In one the production of NH4 from glycine produces two bicarbonate, the other urinary NH3 accepts a hydrogen ion to form NH4. 9/11
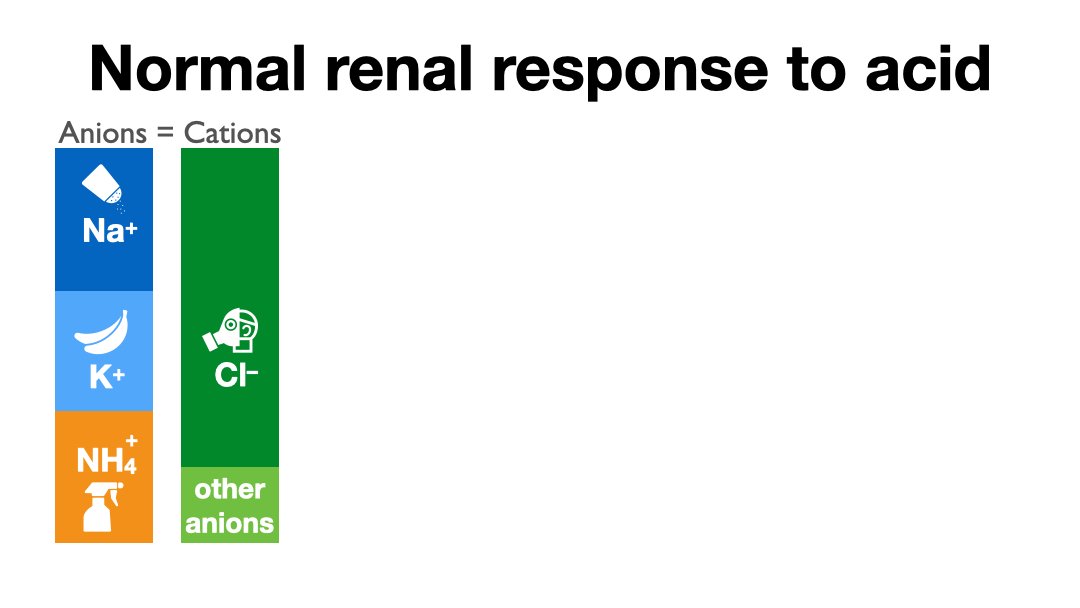
We’ll let the physiologists argue over these two models, for our purpose the only thing you need to know is that a healthy renal response to acidosis is an increase in urinary ammonium to excrete the excess daily acid load. 10/11
The problem comes from the fact that when you order a urine ammonium the lab tells you to pound sand. Even though they can use the same instrument as for serum ammonia. Because the lab won't measure urine NH4 we have substituted the anion gap.
To be continued...
11/11
To be continued...
11/11
Okay, before we move on to part two, let’s review,
The kidneys excrete 50-100 mEq of H+ ions every day, “The daily acid load”
1/15
The kidneys excrete 50-100 mEq of H+ ions every day, “The daily acid load”
1/15
Most of the daily acid load is excreted as H2PO4–, AKA titratable acid
An insignificant < 1% is excreted as free hydrogen (we measure this as urine pH)
And most importantly, for our purposes, in the face of an acid load, that excess acid is excreted as NH4+
2/15
An insignificant < 1% is excreted as free hydrogen (we measure this as urine pH)
And most importantly, for our purposes, in the face of an acid load, that excess acid is excreted as NH4+
2/15
Clinical labs generally refuse to measure urinary ammonium so doctors have been forced to scramble to find ways to “estimate” urinary ammonium.
3/15
3/15
In 1986, electrolyte legend, Mitch Halperin, published this paper which discovered an amazingly tight correlation between urinary anion gap and urinary ammonium.
4/15
4/15
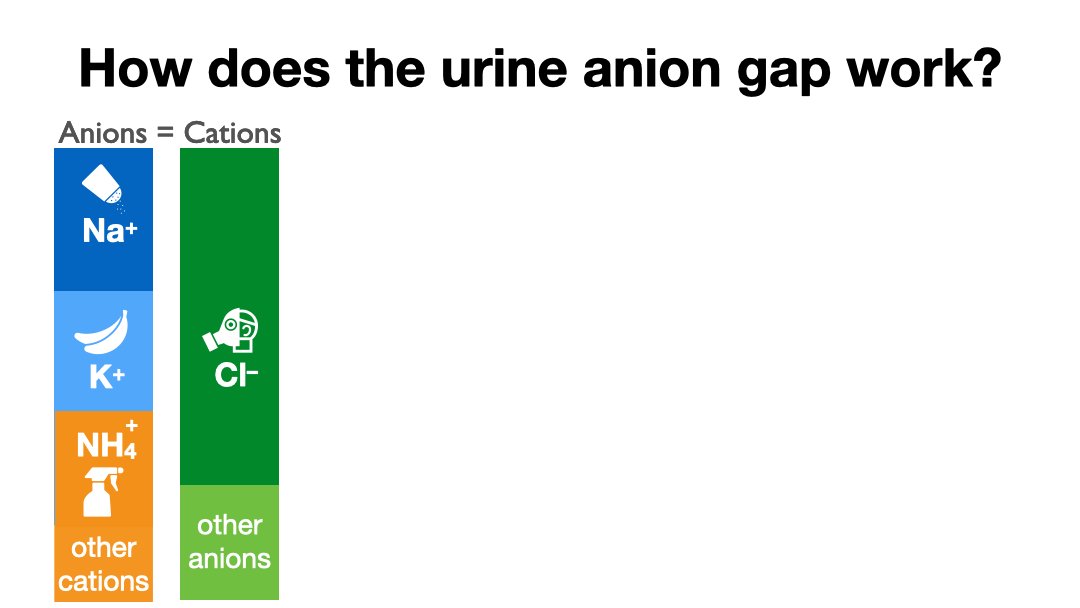
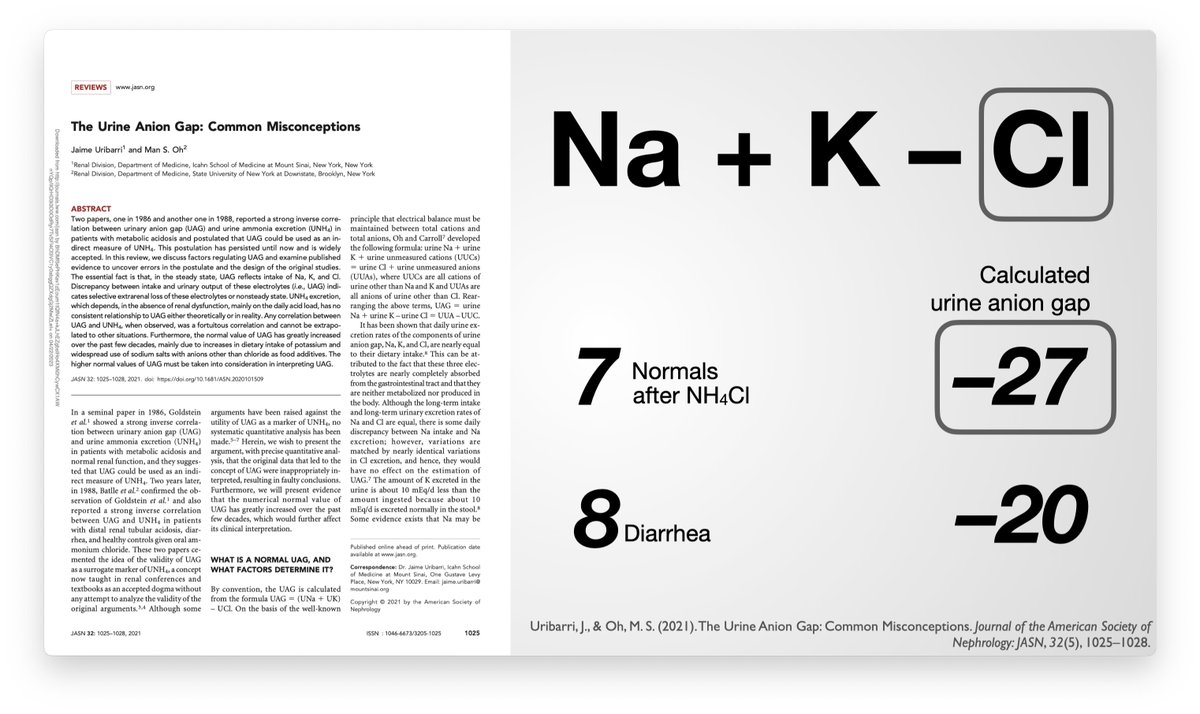
The urine anion gap uses Na, K and Cl to calculate the unmeasured anions minus the unmeasured cations (which includes NH4). Then we define this difference as the urinary anion gap which largely correlated with urinary ammonium.
5/15
5/15
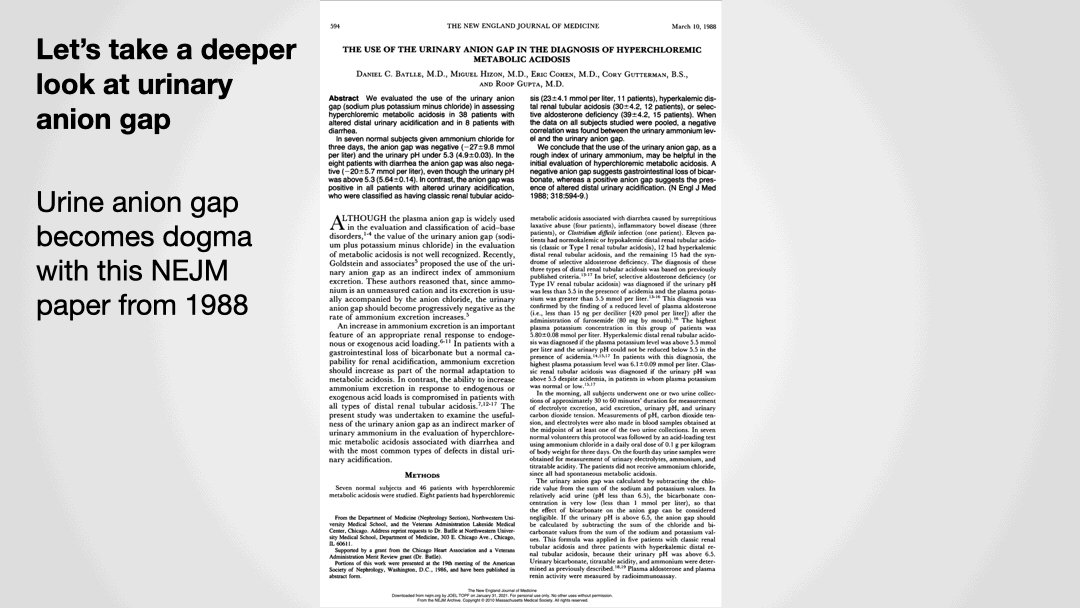
Discoveries are made in Am J Med Sci, but standard of care changes with NEJM. And sure enough, 2 years later, NEJM published this “proof” of the urinary anion gap. Amazing that the NEJM used to publish 60 person physiology studies 😍
6/15
6/15
So for forty years this schema ruled the nephrology wards.
Patients with non-anion gap metabolic acidosis would have urine electrolytes checked in order to see if their kidneys were responding appropriately
7/15
Patients with non-anion gap metabolic acidosis would have urine electrolytes checked in order to see if their kidneys were responding appropriately
7/15
A negative urine anion gap indicated urinary NH4 and a healthy renal response. Think about diarrhea as the cause of metabolic acidosis
A positive urinary anion gap indicated a kidney unable to excrete excess ammonium and suggested distal of hyperkalemic (type 1 or 4) RTA
8/15
A positive urinary anion gap indicated a kidney unable to excrete excess ammonium and suggested distal of hyperkalemic (type 1 or 4) RTA
8/15
But a few years ago Dr. Uribarre began making noises that this whole urinary anion gap went against fundamental laws of nature. Namely that urinary Na, K, and Cl are not there to merely balance charges but that their urinary excretion is dependent on dietary intake
9/15
9/15
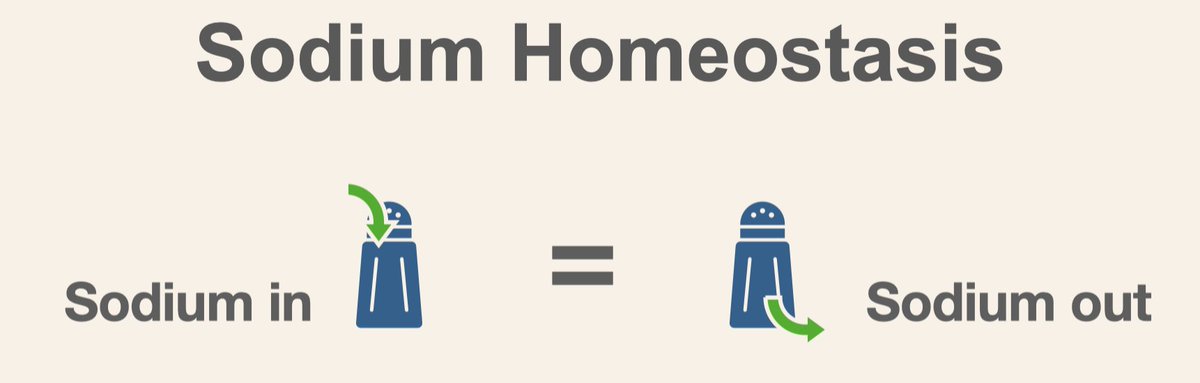
Urine sodium equals dietary sodium. The same goes for potassium and chloride. Spot samples may vary for a short period of time but eventually must reflect dietary intake.
10/15
10/15
Uribarre further points out that diarrhea patients would have volume depletion (due to extra-renal sodium losses) and as a result would lower urine Na, possibly explaining the negative gap.
11/15
11/15
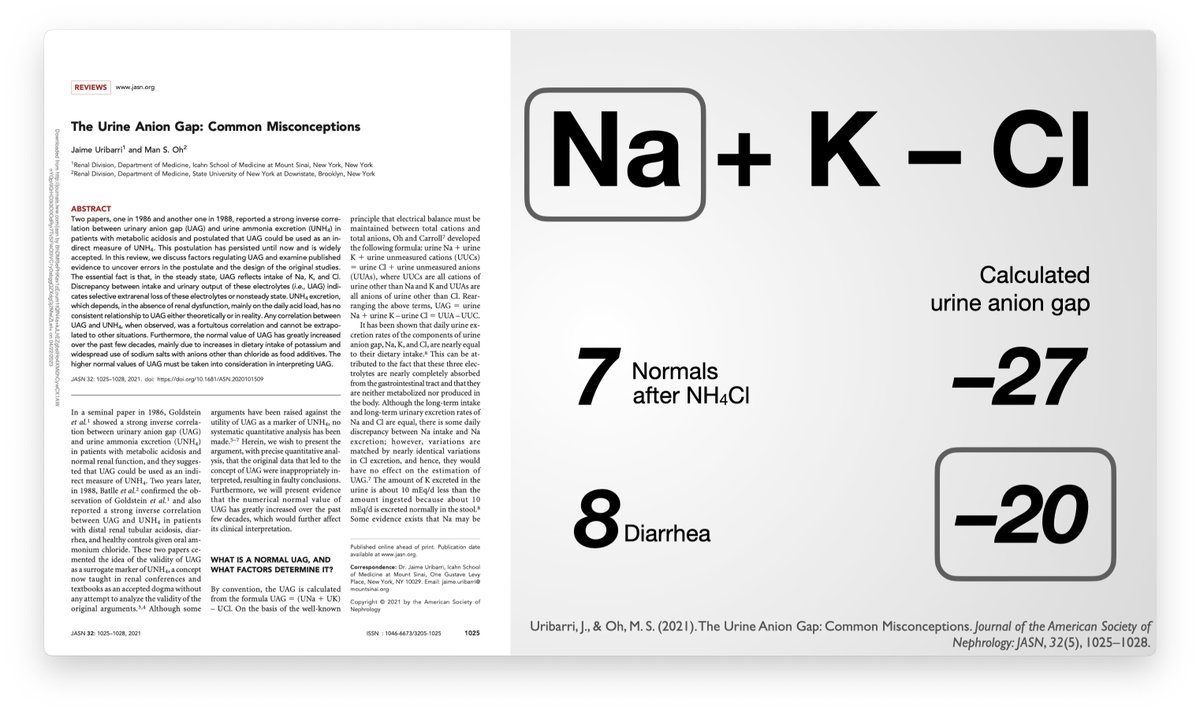
Similarly the healthy controls ion Batlle’s study, were loaded with oral NH3Cl (to induce non-anion gap metabolic acidosis with healthy kidneys). The excess chloride would make the urinary anion gap negative.
12/15
12/15
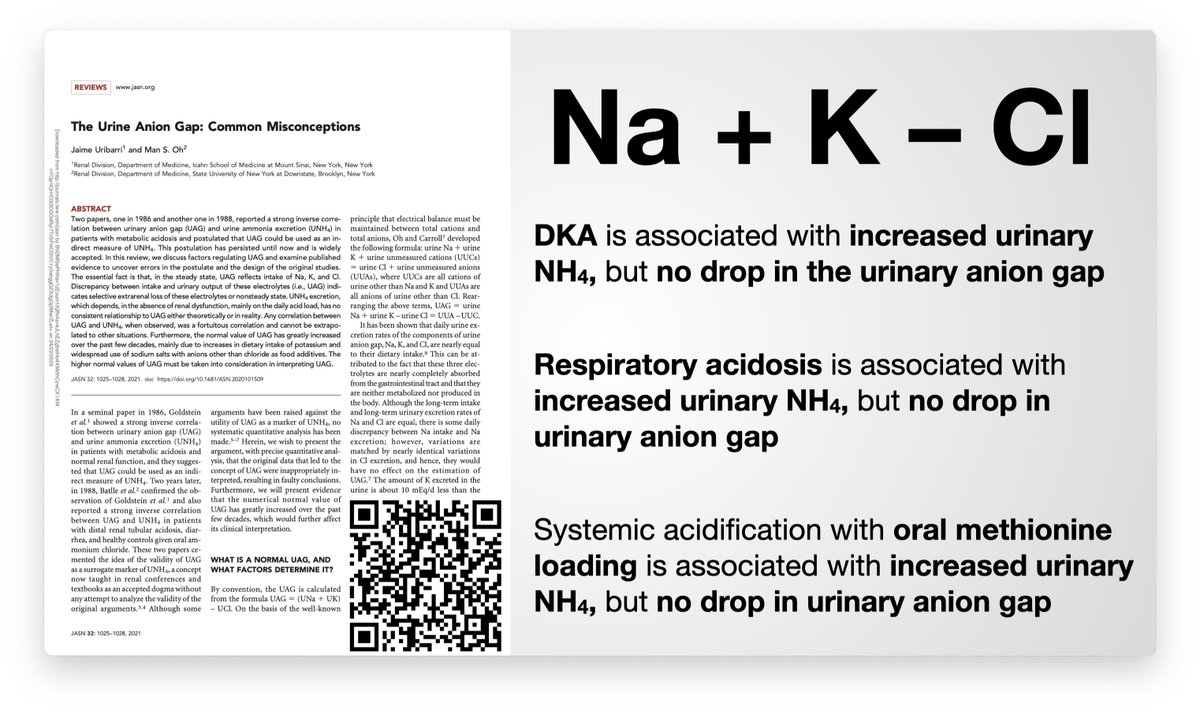
Additionally, DKA, respiratory acidosis, and systemic acidification all result in increased urine ammonium without making the urine anion gap more negative. (refs here: pbfluids.com)
13/15
13/15
But the coup de gras for urine anion gap came from the stoners. LithoLink, a dedicated, commercial, kidney stone lab measures both urine electrolytes and urine ammonium. Asplin provided the data on a 1,000 non-stone formers, and 24,000 stone formers. No Relationship. None at all.
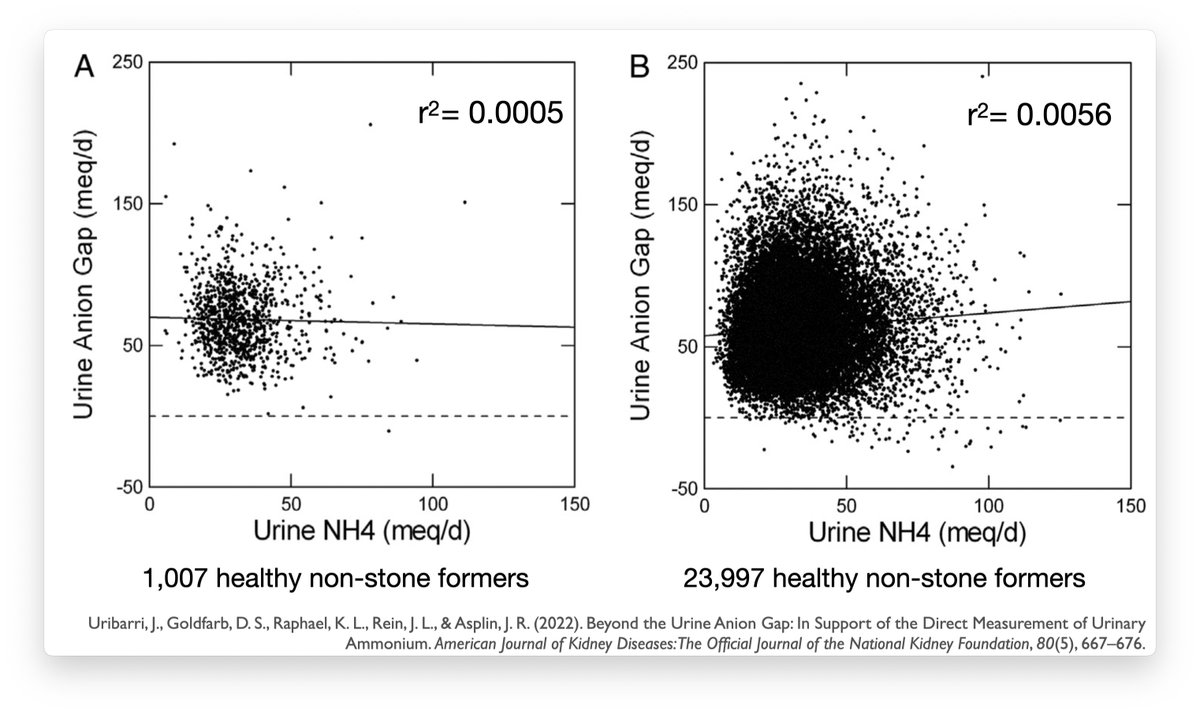
Summary: urinary anion gap is not a good measure of urine ammonium and should be abandoned.
If you need to know the urinary ammonium, measure the urinary ammonium.
15/15
If you need to know the urinary ammonium, measure the urinary ammonium.
15/15
Loading suggestions...