

I argue against sodium restriction in acute heart failure. The line of reasoning is that:
(1) Current evidence suggests restriction is not helpful.
(2) And may be harmful.
(3) There is a solid pathophysiologic basis for this evidence
(1) Current evidence suggests restriction is not helpful.
(2) And may be harmful.
(3) There is a solid pathophysiologic basis for this evidence
Regarding evidence, the trials are small but generally consistent.
In 2013 Aliti showed no differences in change in weight or clinical congestion when a 800 mg/d sodium diet was compared with no restriction.
More thirst was seen in the restriction arm.
pubmed.ncbi.nlm.nih.gov
In 2013 Aliti showed no differences in change in weight or clinical congestion when a 800 mg/d sodium diet was compared with no restriction.
More thirst was seen in the restriction arm.
pubmed.ncbi.nlm.nih.gov



A similar study of HFpEF patients published in 2018 showed similar results (no difference in weight loss or change in congestion).
Again, the restriction arm was 800 mg/d.
pubmed.ncbi.nlm.nih.gov
Again, the restriction arm was 800 mg/d.
pubmed.ncbi.nlm.nih.gov
A 2019 study compared 3 g/day to 7 g/day in 44 adults with acute decompensated heart failure.
No difference in weight loss.
The 7 g/day arm had a greater change in BNP and shorter LOS.
pubmed.ncbi.nlm.nih.gov
No difference in weight loss.
The 7 g/day arm had a greater change in BNP and shorter LOS.
pubmed.ncbi.nlm.nih.gov

Why is there no benefit seen?
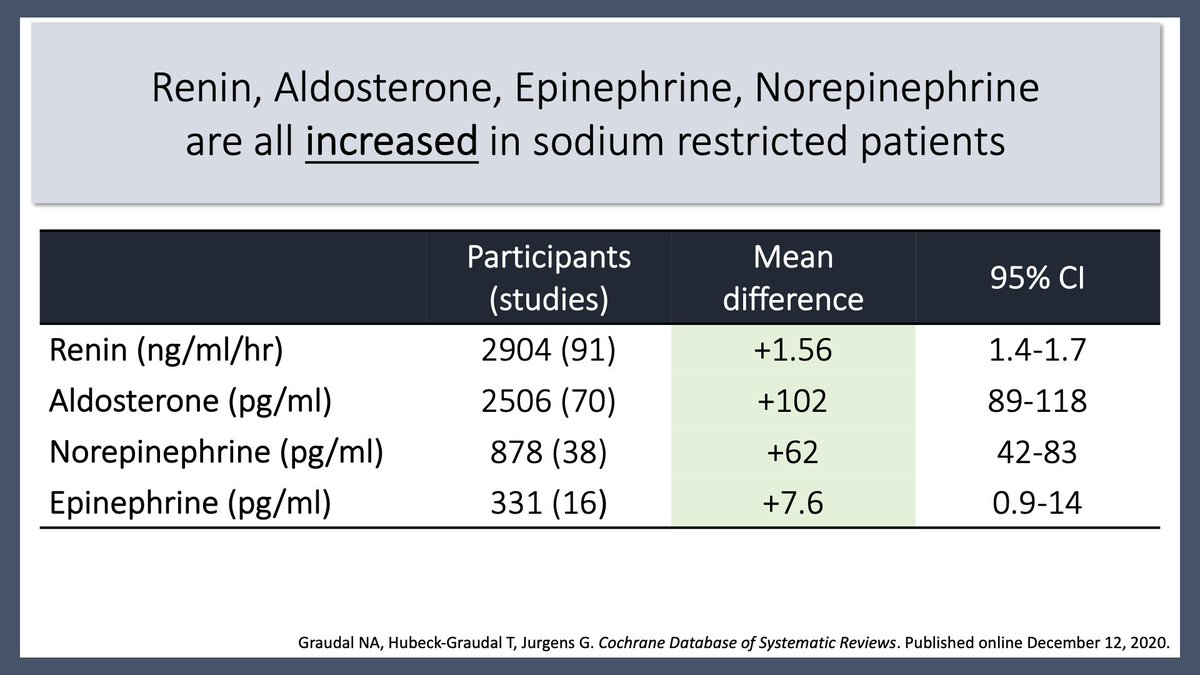
One reason may be that renin, aldosterone, epinephrine, and norepinephrine are all INCREASED in sodium-restricted patients.
pubmed.ncbi.nlm.nih.gov
One reason may be that renin, aldosterone, epinephrine, and norepinephrine are all INCREASED in sodium-restricted patients.
pubmed.ncbi.nlm.nih.gov

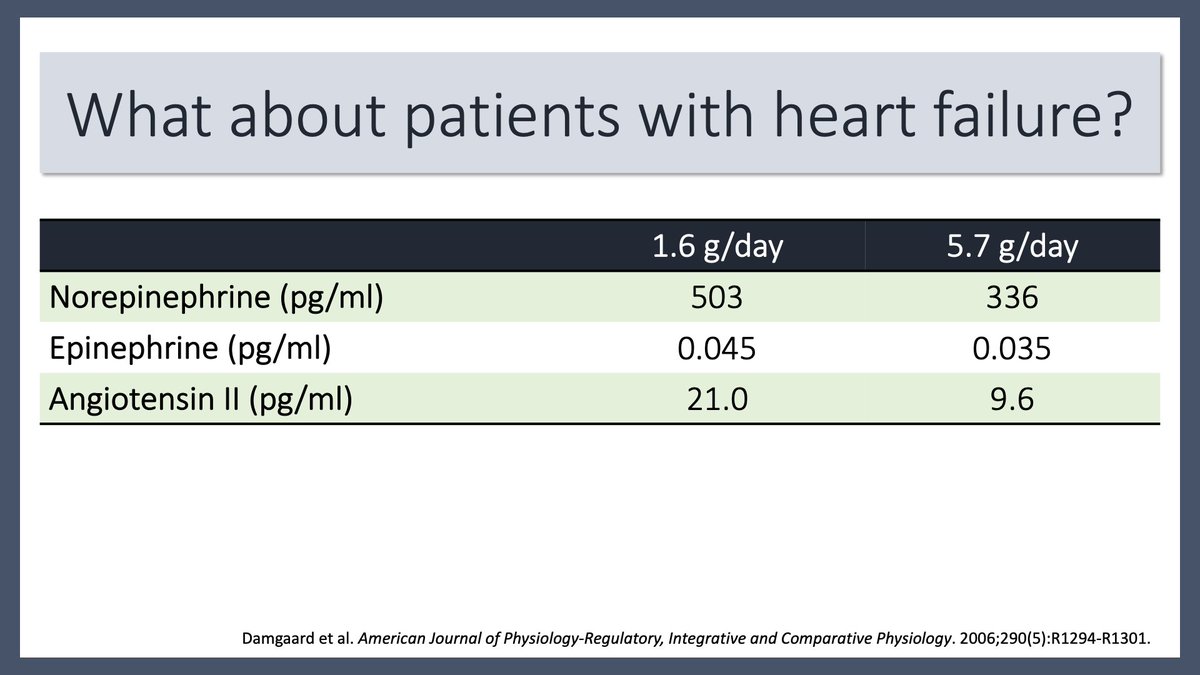
Elevations in norepinephrine and angiotensin II (ATII) are also seen in sodium-restricted patients with heart failure.
The rise in ATII may explain the increased thirst seen in the Aliti trial.
pubmed.ncbi.nlm.nih.gov
The rise in ATII may explain the increased thirst seen in the Aliti trial.
pubmed.ncbi.nlm.nih.gov

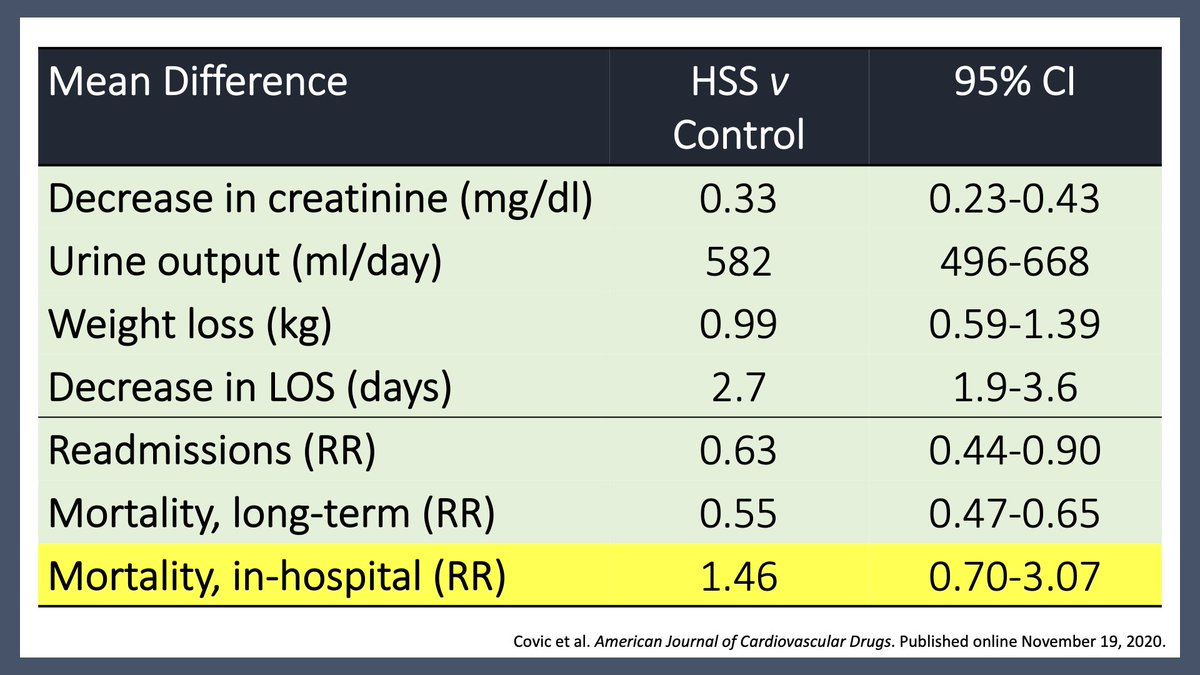
More striking, a meta-analysis of HYPERTONIC saline in acute heart failure found remarkably positive findings.
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
More recently, @ramontgo randomized 70 hospitalized patients with acute HF to 6 g/day of oral NaCl or placebo.
At 96 hours there were no differences in efficacy or safety endpoints, though serum sodium and BUN changes LESS in those supplemented.
pubmed.ncbi.nlm.nih.gov
At 96 hours there were no differences in efficacy or safety endpoints, though serum sodium and BUN changes LESS in those supplemented.
pubmed.ncbi.nlm.nih.gov

Taken together, there is no good data supporting sodium restriction in heart failure. If anything, the available data suggests that hypertonic saline administration may be beneficial.
جاري تحميل الاقتراحات...