

🧵TIA/minor stroke case🚑🧠
88F presents to ED w/ 30 min of R hand/arm weakness, w/o associated symptoms.
CT/CTA- no signs of early ischemic change and no significant vascular abnormality.
Appropriately started on DAPT, discharged from ED with referral to rapid TIA clinic.
88F presents to ED w/ 30 min of R hand/arm weakness, w/o associated symptoms.
CT/CTA- no signs of early ischemic change and no significant vascular abnormality.
Appropriately started on DAPT, discharged from ED with referral to rapid TIA clinic.
Seen in clinic 2 days later and has remained asymptomatic on DAPT.
- MRI brain, echo and holter monitor arranged.
- Plan for DAPT x 3 weeks then ASA.
- MRI brain, echo and holter monitor arranged.
- Plan for DAPT x 3 weeks then ASA.
MRI below (SWI sequence; DWI- top right labelled). DWI negative.
There has been interval development of right frontal ICH on DAPT not seen on initial CT.
Cardiac w/u negative.
How can you explain everything?
There has been interval development of right frontal ICH on DAPT not seen on initial CT.
Cardiac w/u negative.
How can you explain everything?
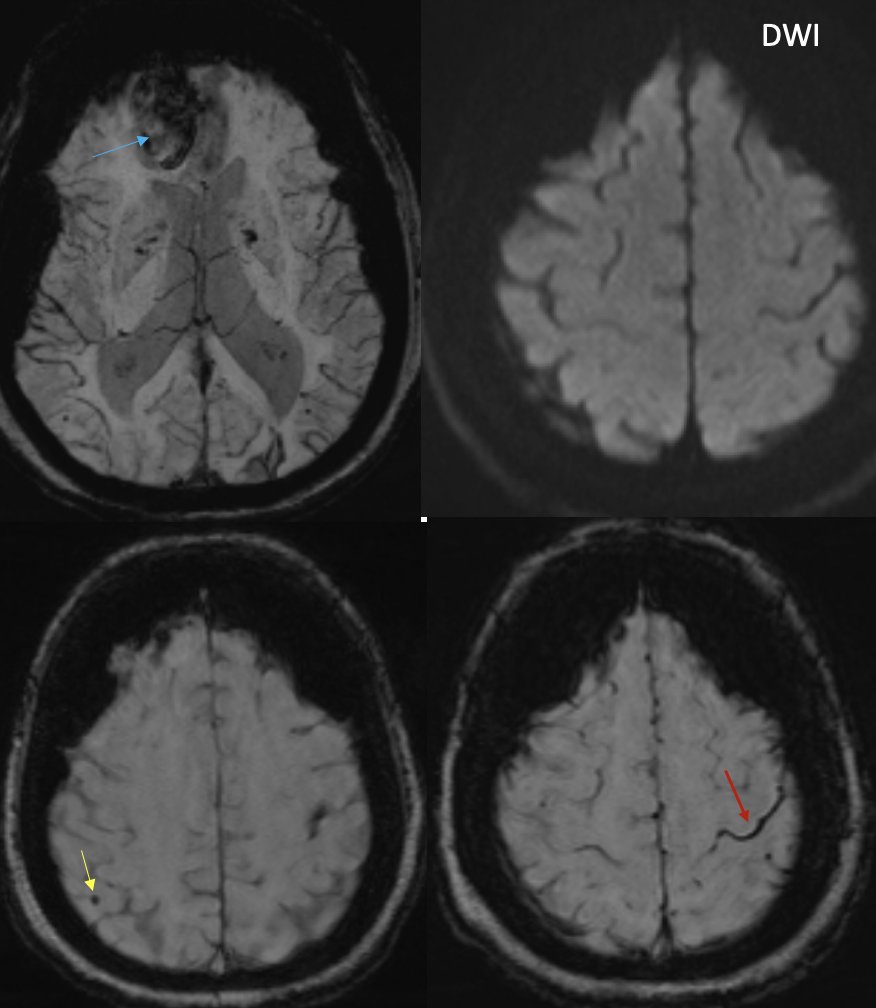
dx: Probable CAA, with CAA-related TFNE secondary to cortical superficial siderosis 🎢🩸(overlaying left central sulcus likely explaining transient R hand symptoms from cortical spreading depression)
cSS= red arrow
cortical MCB = yellow arrow
cortical R frontal ICH= blue arrow
cSS= red arrow
cortical MCB = yellow arrow
cortical R frontal ICH= blue arrow
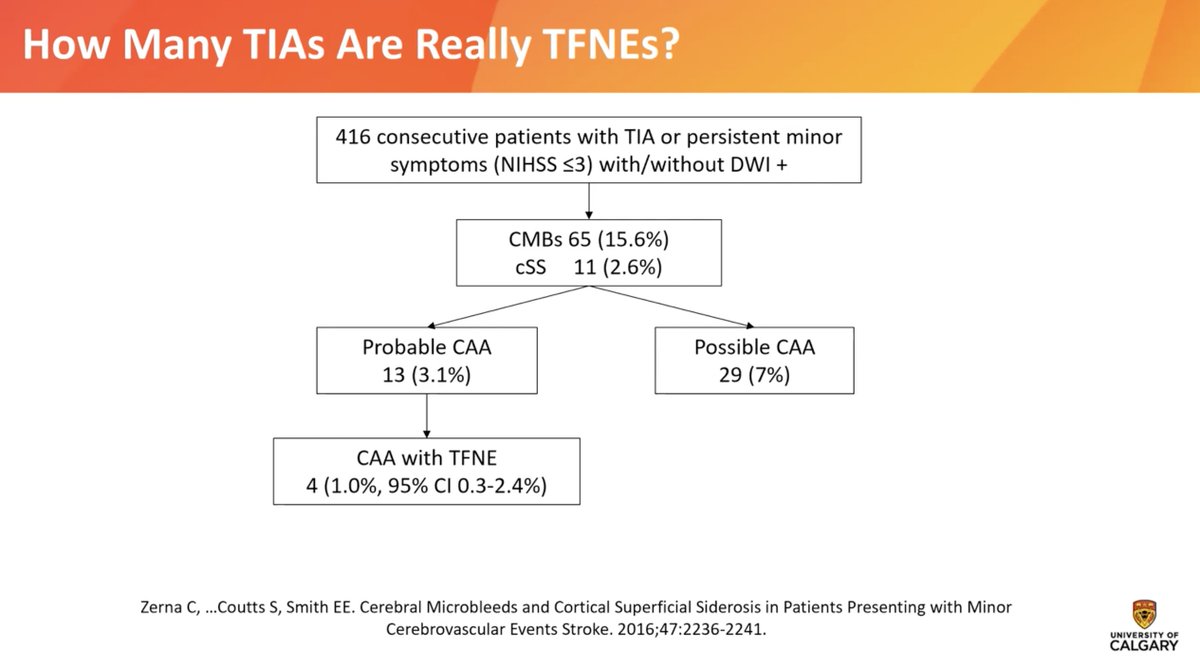
This likely occurs in ~1% of 'TIAs'. Slide below from @VCI_EricSmith
Management:
- stop DAPT (no cardiac indication)
- Aggressive BP control to ~ 120/80mmHg.
#neurotwitter #stroke #MedEd #neurology
- stop DAPT (no cardiac indication)
- Aggressive BP control to ~ 120/80mmHg.
#neurotwitter #stroke #MedEd #neurology
Loading suggestions...