
1) Welcome to our #accredited #tweetorial risk-guided, staged/sequential management of patients with Stage 3-4 #CKD in the context of #DM, by the interprofessional team. I am Carlo Trinidad MD, @hellokidneyMD, from Villaflor Memorial Hospital 🇵🇭. #Nephtwitter #Medtwitter #FOAMed

2) This #accredited #tweetorial series on #kidneydisease #CKD is supported by an independent educational grant from the Boehringer Ingelheim/Lilly Alliance. It is not intended for US- or UK-based based HCPs. Accreditation statement & faculty disclosures at cardiometabolic-ce.com
3) This activity is accredited for #physicians #physicianassociates #nurses #NPs #pharmacists. Prior programs in this series, still eligible for CE/#CME, can be accessed at cardiometabolic-ce.com. Please FOLLOW US for ongoing #accredited education, delivered wholly on Twitter!
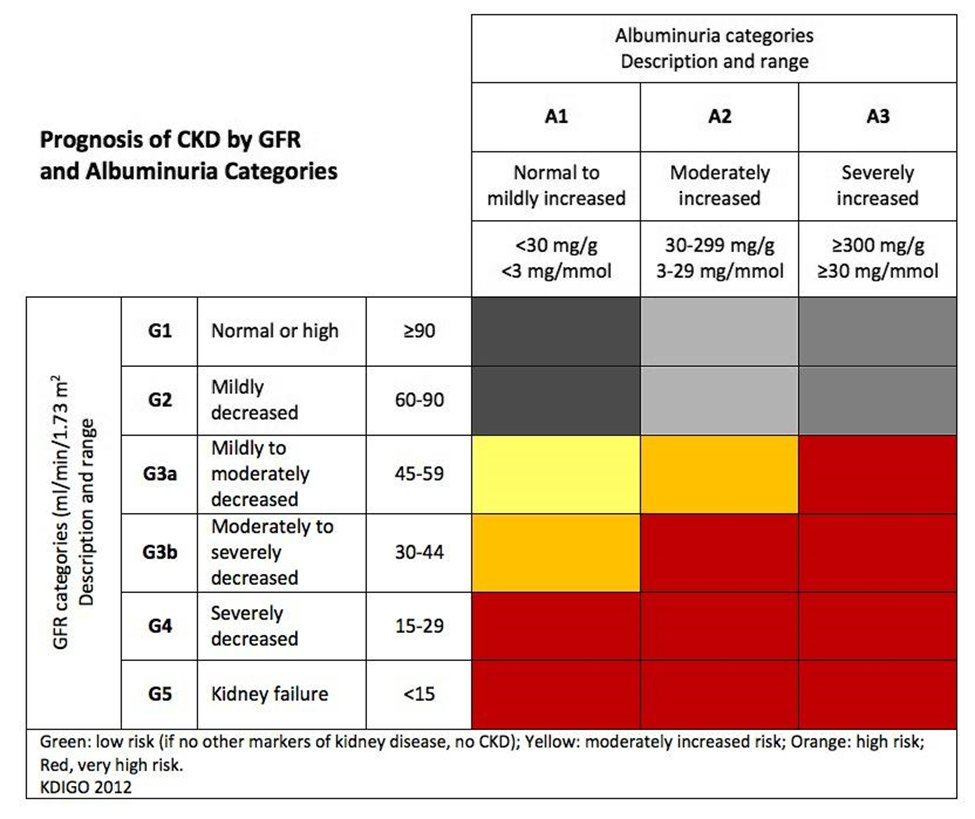
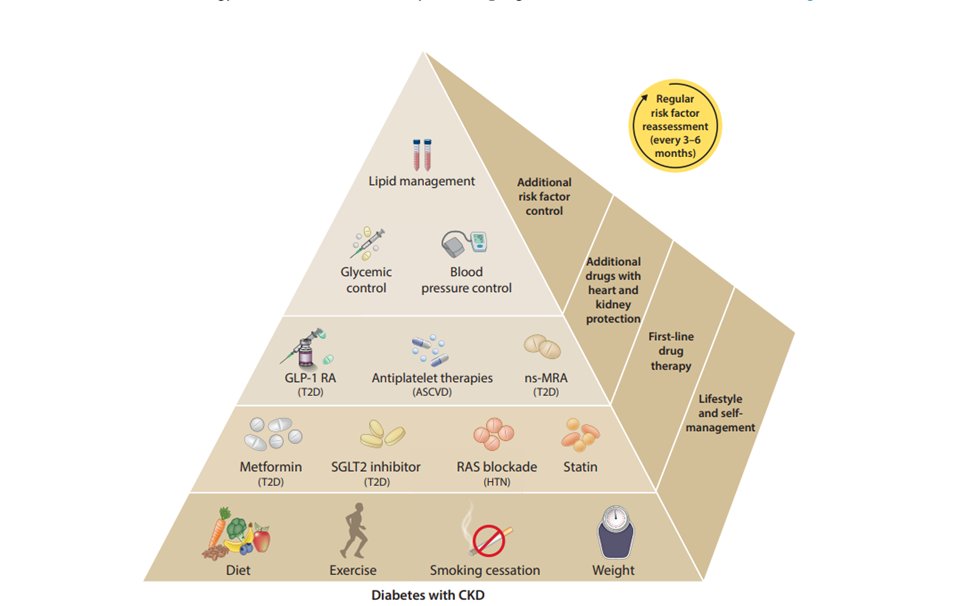
4) In this #tweetorial, we will be highlighting the current evidence for a multi-disciplinary approach in slowing #CKD progression in patients with #T2D (G3aA1 - G4A3).
7) You saw a 47/F with T2D in the clinic with BPs ranging from 140-160/80-100. Her #UACR was at 1200 mg/g. You would start which medication to control her BP?
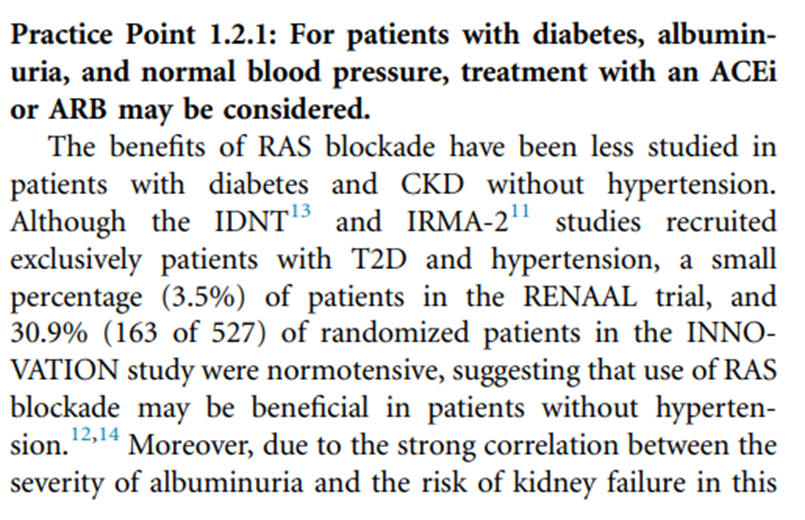
13) The right answer is C. @goKDIGO updated its guidelines in 2021 w/ a new target of SBP <120 mmHg, regardless of #proteinuria status (2B). This is based on data from #SPRINT, which showed ⬇️CV outcomes w/ intensive treatment.
🔓kdigo.org
🔓kdigo.org
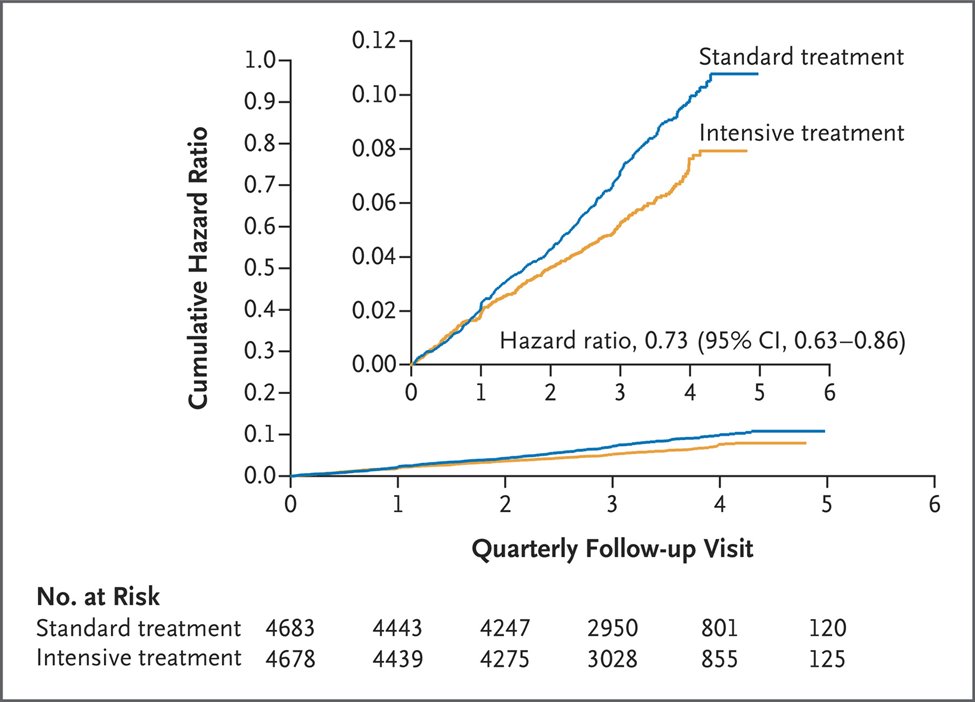
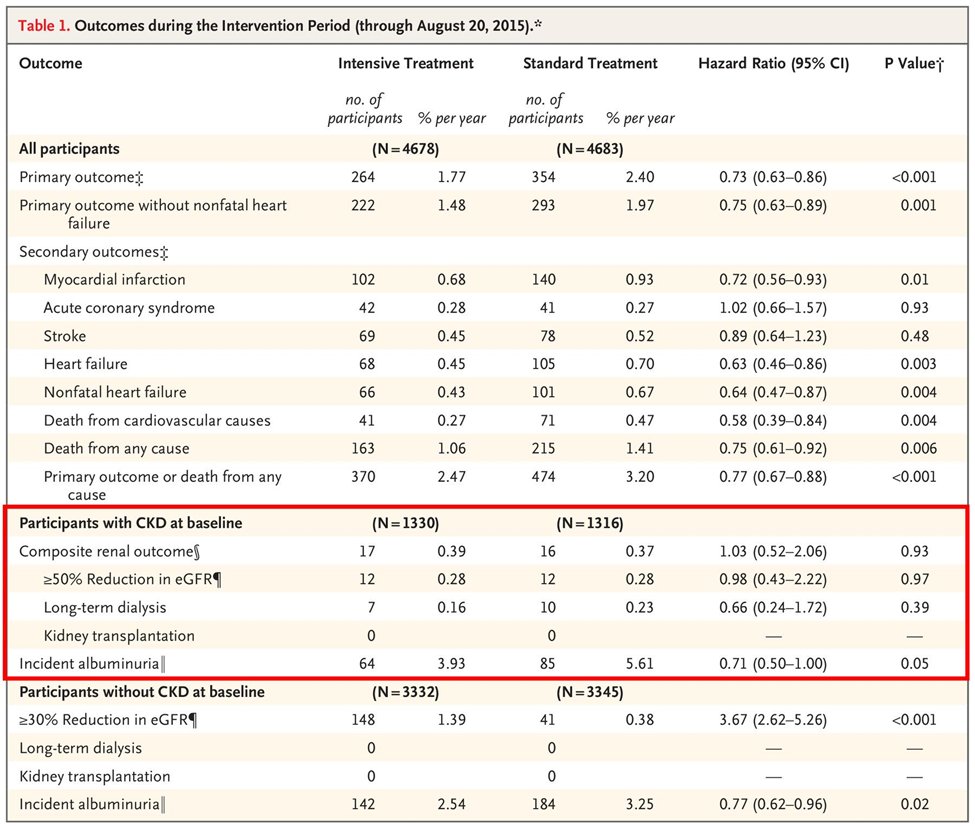
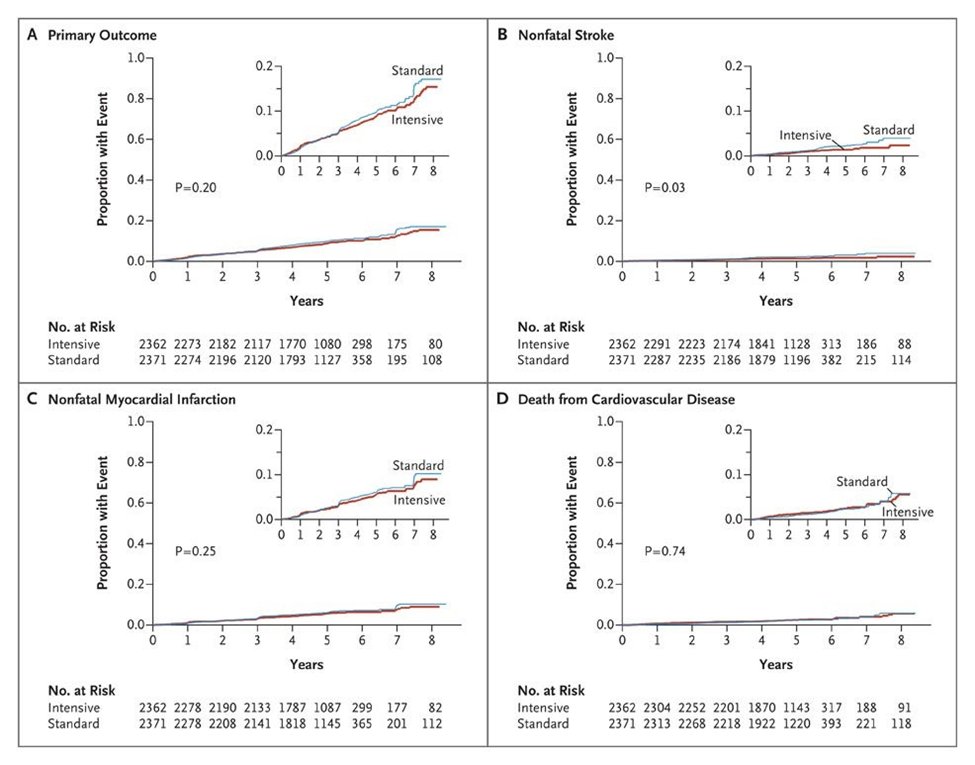
17) The current recommendation of @goKDIGO of <120 mmHg SBP comes from the combination analysis of both #SPRINT and #ACCORD data.
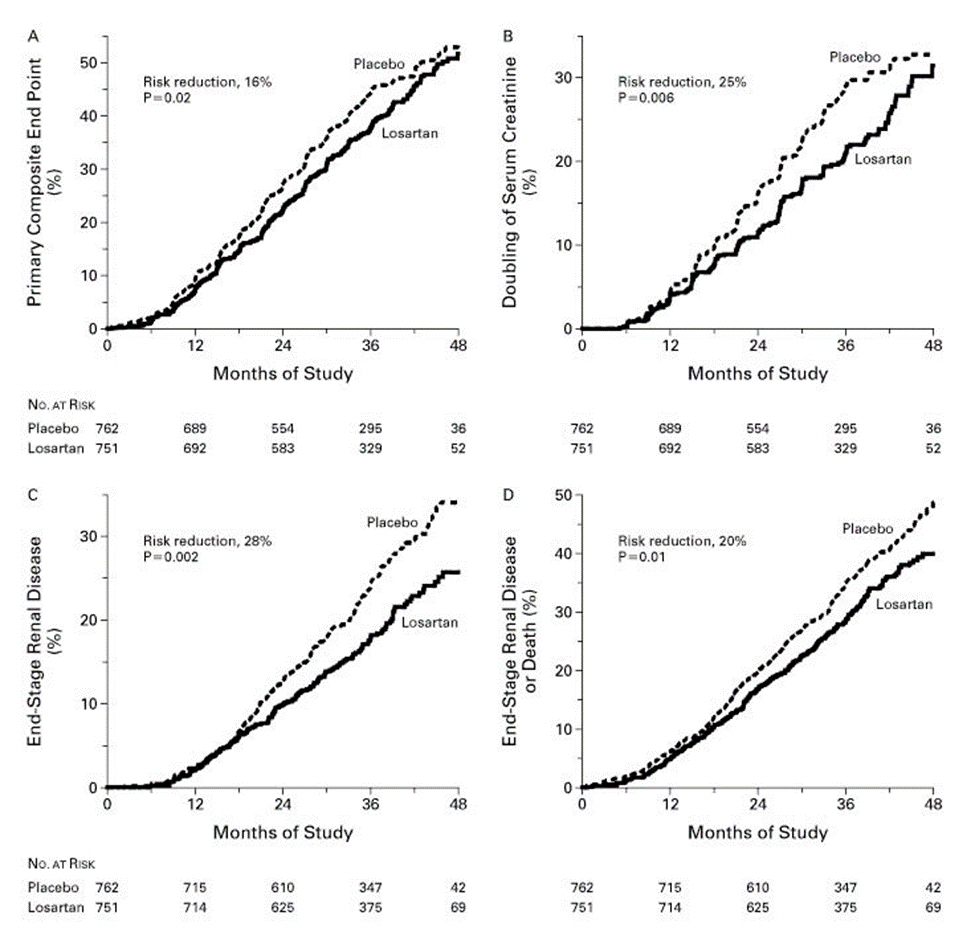
✅ Recommended for T2D and CKD
⛔ No evidence for #renoprotection
⬇️ #CV outcomes
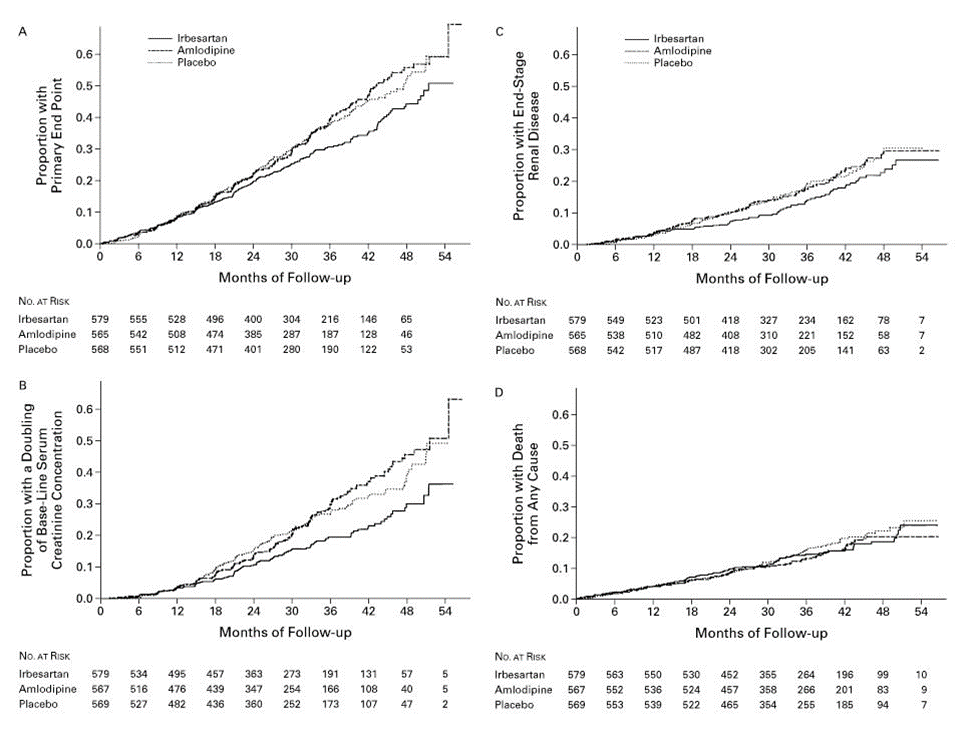
✅ Recommended for T2D and CKD
⛔ No evidence for #renoprotection
⬇️ #CV outcomes
18) A ⬆️in serum #creatinine should not cause an immediate cessation of #ACEi or #ARBs. It is important to review other causes of #AKI and concomitant drugs that can ⬆️creatinine. Reduce dose or stop if mitigation strategies are ineffective.
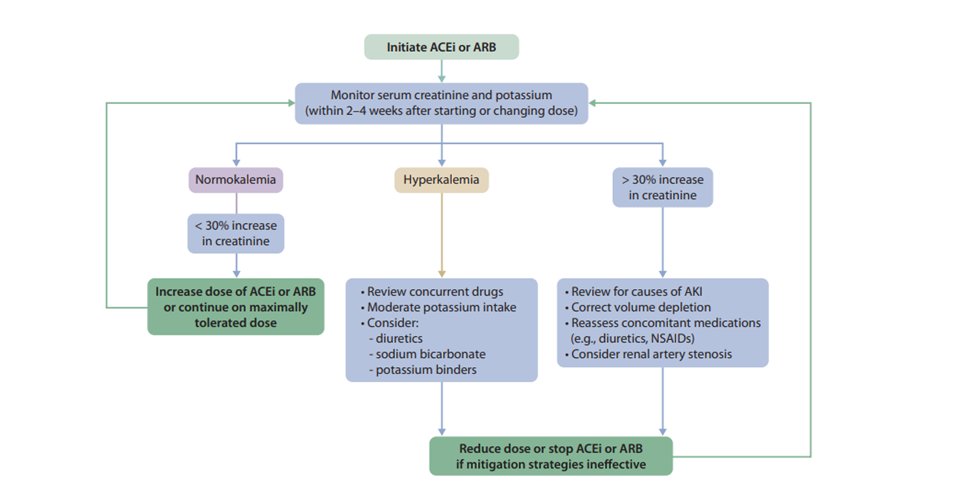
19a) #Hyperkalemia is a known effect of #RAS blockade with ACEi or ARB. Stopping these drugs can ⬆️ CV events, so mitigation of hyperK is important. Strategies include:
✅moderation of K intake
✅avoid drugs that ⬆️K
✅use diuretics
✅use sodium bicarbonate
✅use K binders
✅moderation of K intake
✅avoid drugs that ⬆️K
✅use diuretics
✅use sodium bicarbonate
✅use K binders
20) That’s all for part 1. Be sure to come back TOMORROW for part 2 and the rest of our discussion on #renoprotection in patients with #CKD Stage 3-4.
👏 @brian_rifkin @AgarwalRajivMD @nephronus @edgarvlermamd @sophia_kidney @ChristosArgyrop @medtweetorials @nephondemand
👏 @brian_rifkin @AgarwalRajivMD @nephronus @edgarvlermamd @sophia_kidney @ChristosArgyrop @medtweetorials @nephondemand
Loading suggestions...