

In most cases of zoster, pain/sensory symptoms precede the rash, often by many days.
So it's always worth considering zoster if there's pain in a unilateral distribution that's not clearly another syndrome.
But...
🧵1/10
So it's always worth considering zoster if there's pain in a unilateral distribution that's not clearly another syndrome.
But...
🧵1/10
Once you've considered it...
How do you further stratify suspicion, and decide whether to
- pursue more diagnostics for other processes vs. rely on time to bring diagnostic clarity
- treat zoster empirically
?
2/10
How do you further stratify suspicion, and decide whether to
- pursue more diagnostics for other processes vs. rely on time to bring diagnostic clarity
- treat zoster empirically
?
2/10
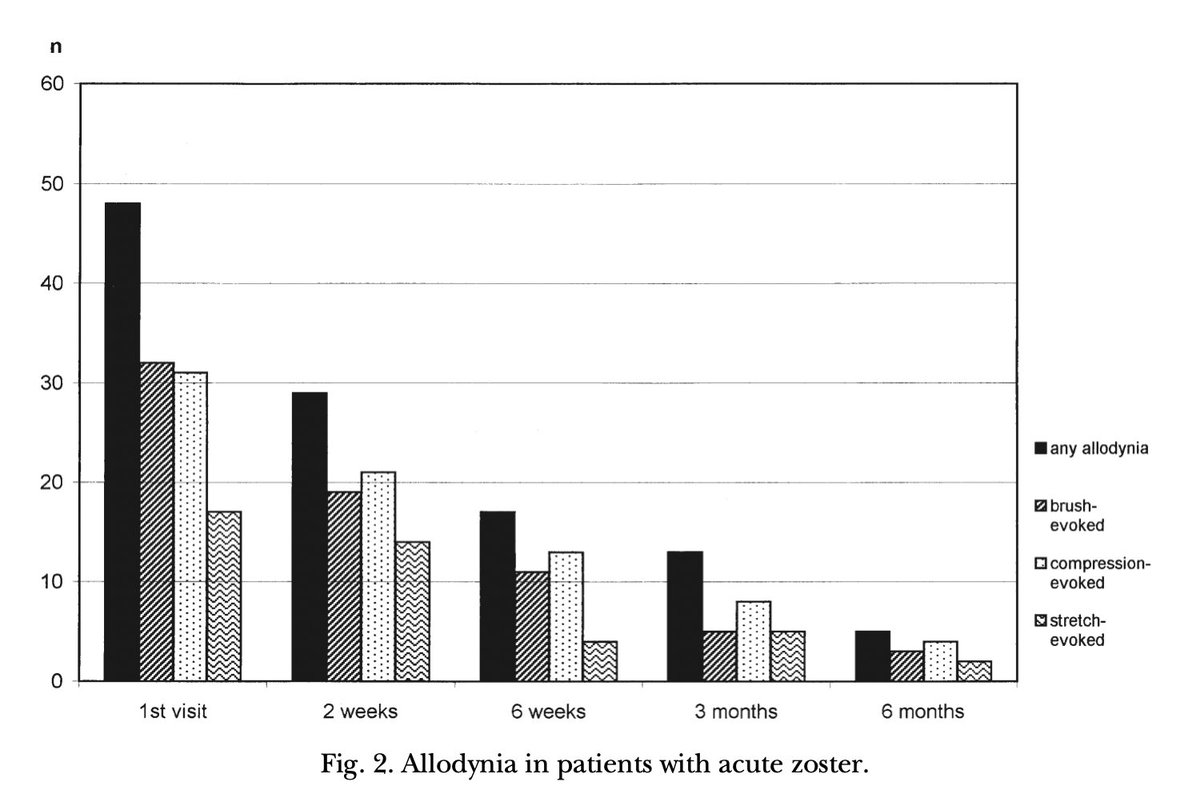
Something I've been doing intuitively is to test for cutaneous allodynia - pain due to a stimulus that normally does not cause pain, like brushing lightly on the skin
3/10
3/10
When present, I've taken this as a meaningful (specific-ish) finding
When absent, I've been more cautious, suspecting low or moderate sensitivity.
4/10
When absent, I've been more cautious, suspecting low or moderate sensitivity.
4/10
I've been trying to find some data to confirm/deny this, but having trouble. Help!
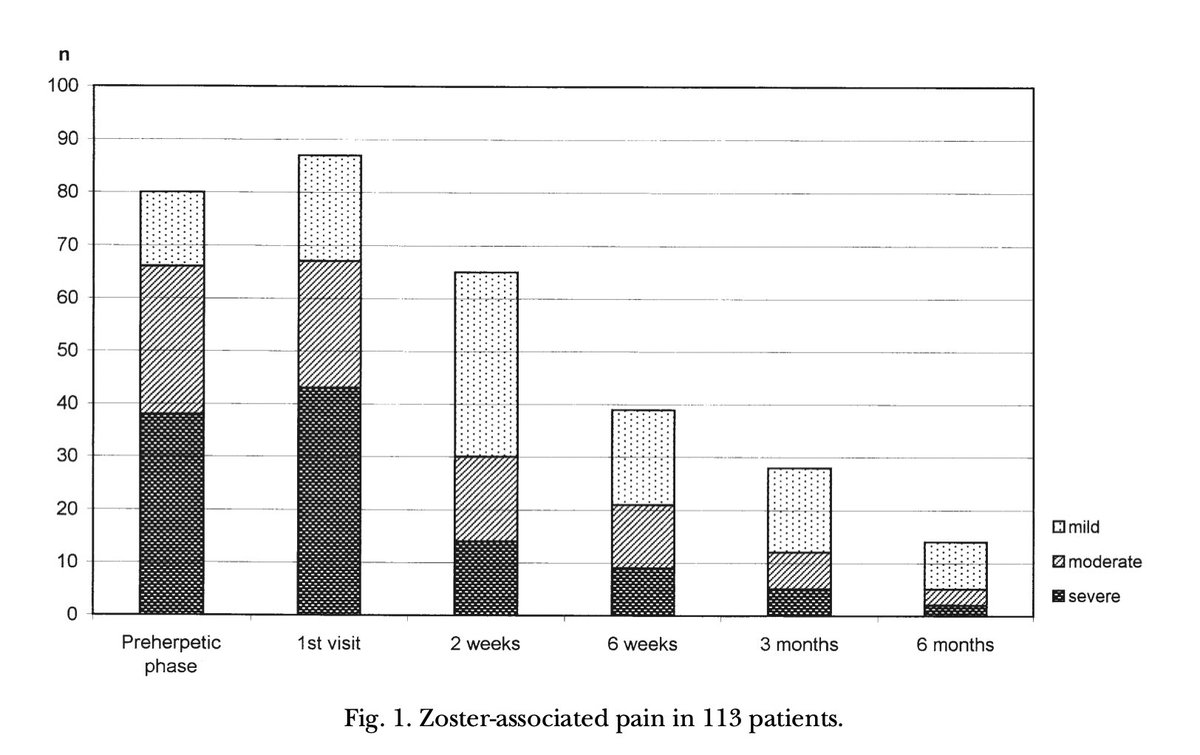
Best I found is this study of 113 patients with zoster *rash.*
tinyurl.com
5/10
Best I found is this study of 113 patients with zoster *rash.*
tinyurl.com
5/10
Only a minority had allodynia... so indeed, not reliably sensitive.
6/10
6/10
And while these were patients assessed in the herpetic (rash) and post-herpetic phases, I think ok to extrapolate given similar incidence/levels of pre-herpetic pain (by patient recall).
7/
7/
On the specificity side, I can't find good data, and this study certainly couldn't assess this.
In my experience, allodynia from other causes tends to be either from a known neuropathy in a predictable distribution...
8/10
In my experience, allodynia from other causes tends to be either from a known neuropathy in a predictable distribution...
8/10
Or diffuse.
Which, when acute, I've most commonly noticed in patients with gram-negative bacteremia.
Anyone else? @AvrahamCooperMD @RebeccaEBerger
But my guess is that lateralizing and limited (i.e. potentially dermatomal) cutaneous allodynia has few ddx @AaronLBerkowitz
9/
Which, when acute, I've most commonly noticed in patients with gram-negative bacteremia.
Anyone else? @AvrahamCooperMD @RebeccaEBerger
But my guess is that lateralizing and limited (i.e. potentially dermatomal) cutaneous allodynia has few ddx @AaronLBerkowitz
9/
Curious to hear experience from #medtwitter on this question and its application, i.e. tweet 2/
Tagging some outpatient docs who probably deal most often @PalamaraMcgrath @SuzanneKovenMD @adamcifu @PaulNWilliamz
10/10
Tagging some outpatient docs who probably deal most often @PalamaraMcgrath @SuzanneKovenMD @adamcifu @PaulNWilliamz
10/10
Loading suggestions...