

🫁💧 Pleural Effusion Schema 💧🫁
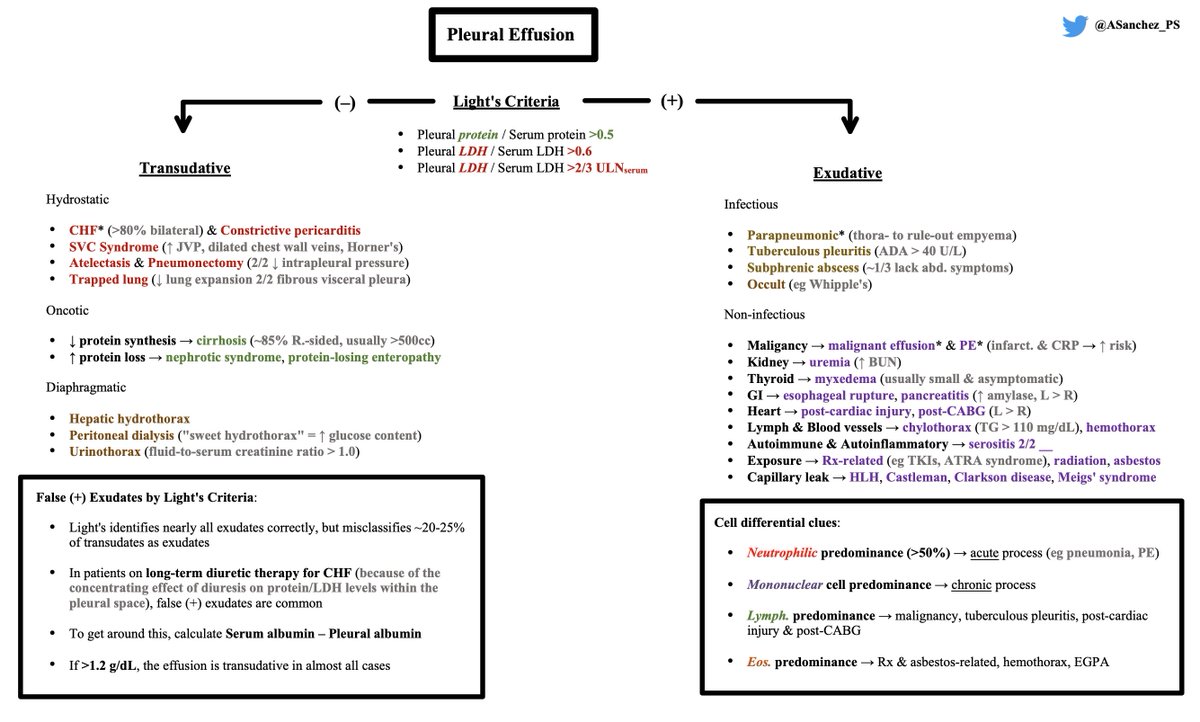
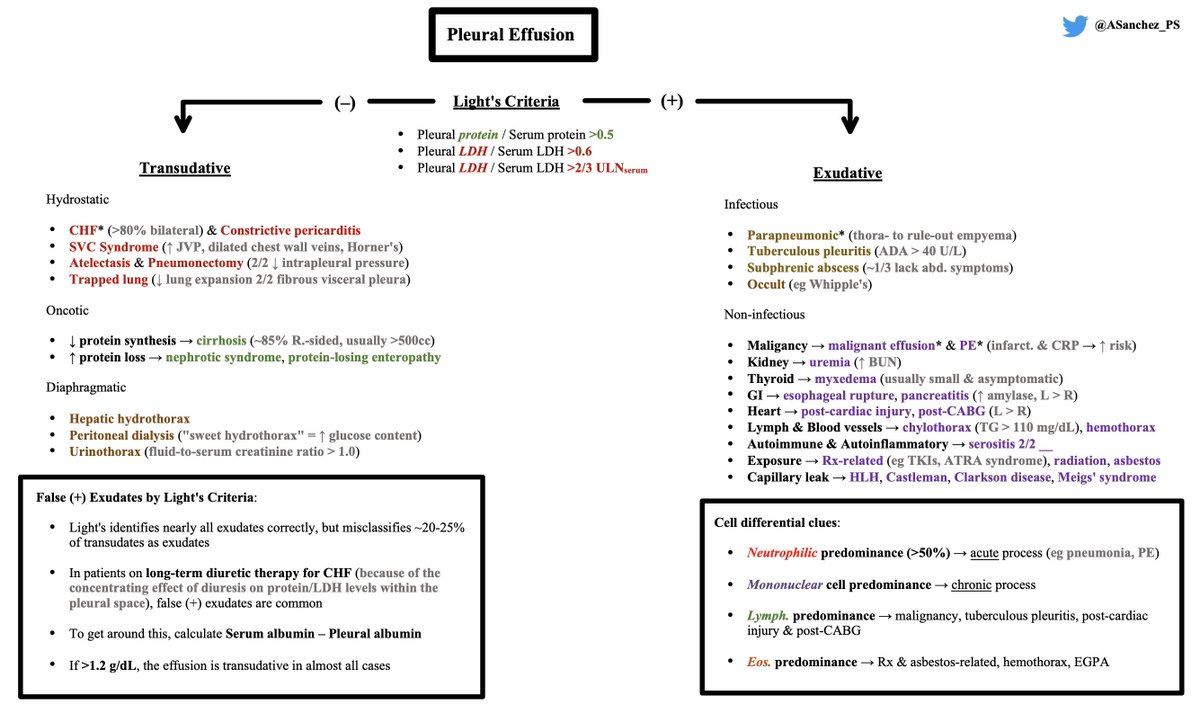
1) Thoracentesis → Calculate Light's criteria (Note: ~20-25% of true transudates are misclassified)
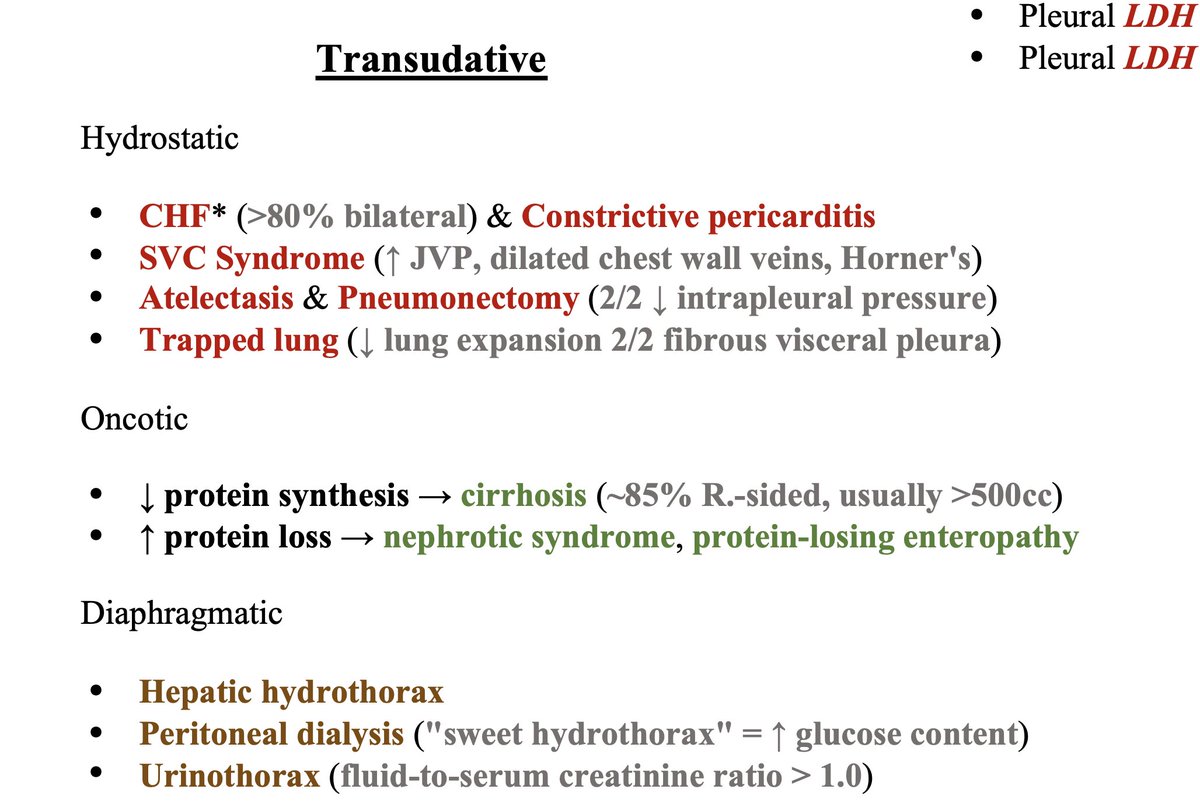
2) Stratify transudative DDx by Starling equation (Hydrostatic, Oncotic etiologies) & Diaphragm-related etiologies
3) Exudative DDx = longer!
1) Thoracentesis → Calculate Light's criteria (Note: ~20-25% of true transudates are misclassified)
2) Stratify transudative DDx by Starling equation (Hydrostatic, Oncotic etiologies) & Diaphragm-related etiologies
3) Exudative DDx = longer!
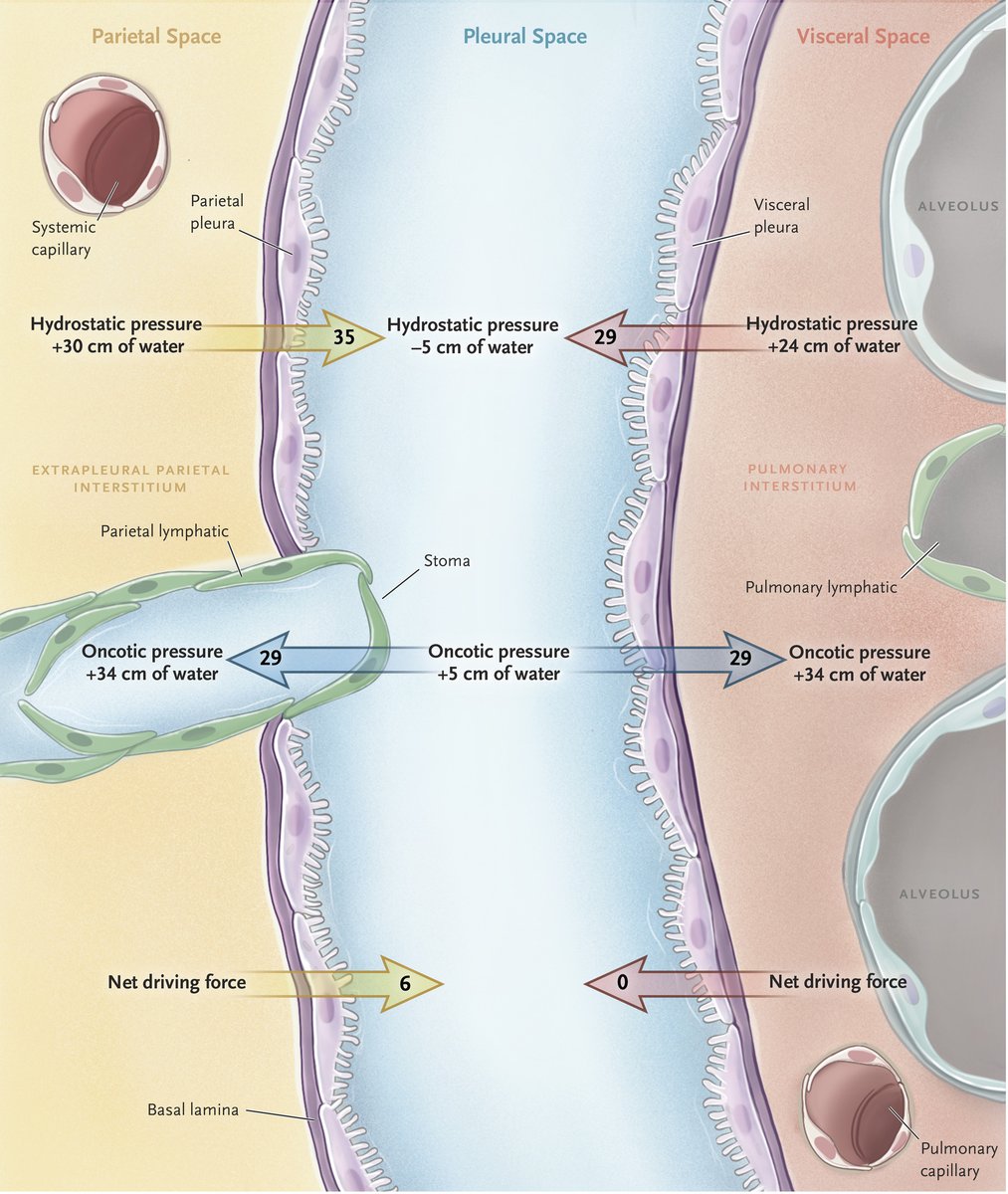
B/c hydrostatic pressures are higher on the parietal pleura than on the visceral pleura & the oncotic pressures are equivalent, pleural fluid is primarily produced from the parietal pleura. The lymphatic vessels on the parietal pleura are responsible for pleural fluid resorption.
💧 Of the transudative effusions, decompensated CHF is the most common
💧 Oncotic issues can be due to ↓ protein synthesis (cirrhosis) & ↑ protein loss (nephrotic syndrome, protein-losing enteropathy)
💧 Other etiologies have unique pathophys. & lab signatures (see below)
💧 Oncotic issues can be due to ↓ protein synthesis (cirrhosis) & ↑ protein loss (nephrotic syndrome, protein-losing enteropathy)
💧 Other etiologies have unique pathophys. & lab signatures (see below)
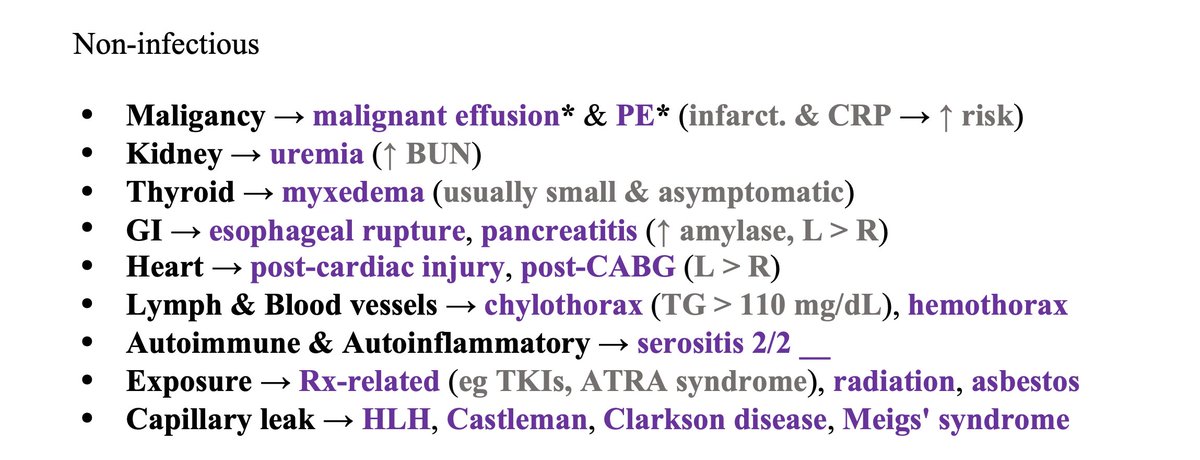
Exudative effusions = infectious vs. non-infectious
- Mechanism #1: ↑ capillary permeability
- Mechanism #2: Lymphatic obstruction
- Mechanism #1: ↑ capillary permeability
- Mechanism #2: Lymphatic obstruction
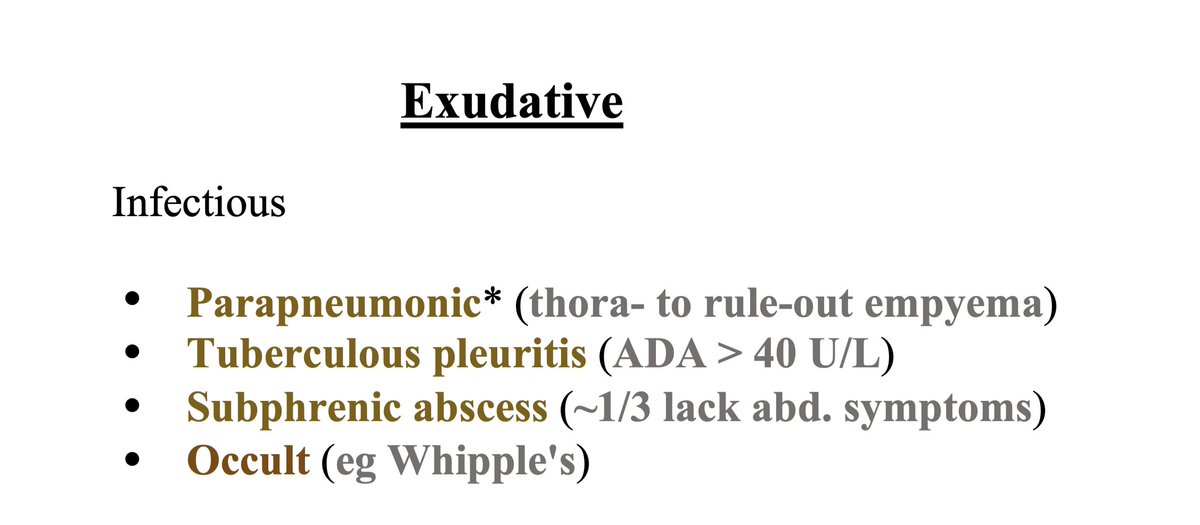
Infectious exudates:
🦠 If pneumonia, must perform thora- to rule-out complicated parapneumonic effusion. The following findings can be seen:
- Frank pus
- (+) Gram stain/culture
- pH < 7.2
- Glucose < 60 mg/dL
- Loculated, thick parietal pleura
🦠 If pneumonia, must perform thora- to rule-out complicated parapneumonic effusion. The following findings can be seen:
- Frank pus
- (+) Gram stain/culture
- pH < 7.2
- Glucose < 60 mg/dL
- Loculated, thick parietal pleura
🦠 Subphrenic abscess (abdominal etiology) often has pulmonary-predominant symptoms (~1/3 lack abdominal symptoms)
🦠 Occult disseminated infection may be something to consider if effusions subtle & history consistent (eg serositis of Whipple's)
🦠 Occult disseminated infection may be something to consider if effusions subtle & history consistent (eg serositis of Whipple's)
Non-infectious exudative DDx is where the list gets super long.
Grouping these diagnoses by organ system & other buckets is helpful!
🔥 Malignant effusion & PE are grouped because "unprovoked" PE in a young person should prompt consideration of malignancy screening
Grouping these diagnoses by organ system & other buckets is helpful!
🔥 Malignant effusion & PE are grouped because "unprovoked" PE in a young person should prompt consideration of malignancy screening
Final pearls:
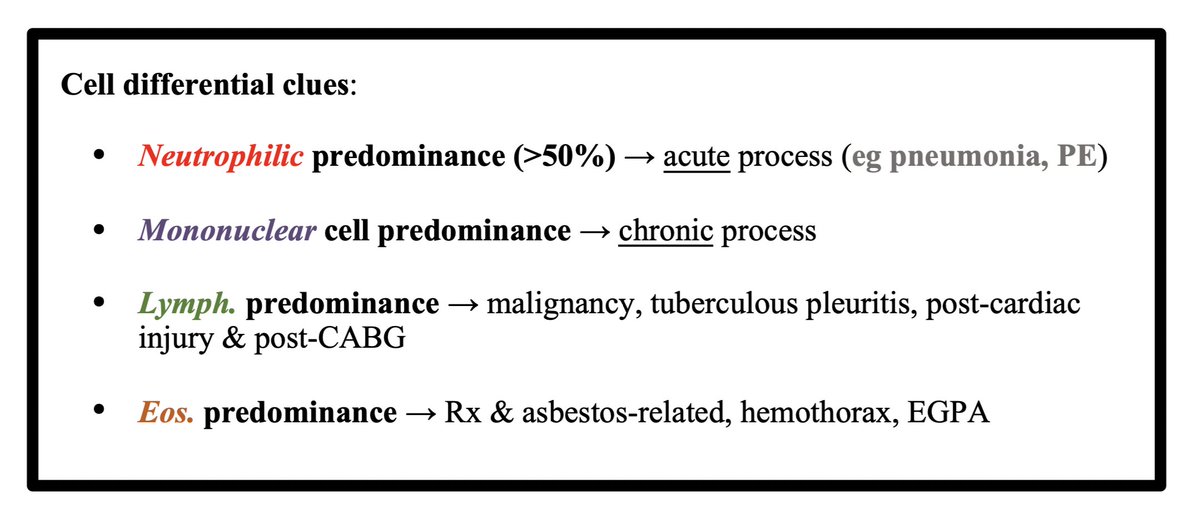
⚪ Cell differential of the pleural fluid may provide a hint
⚪ If suspicion for false (+) exudate, calculate Serum albumin – Pleural albumin (if > 1.2, the effusion is transudative in almost all cases)
⚪ Asterisks in the one-pager denote the most common causes
⚪ Cell differential of the pleural fluid may provide a hint
⚪ If suspicion for false (+) exudate, calculate Serum albumin – Pleural albumin (if > 1.2, the effusion is transudative in almost all cases)
⚪ Asterisks in the one-pager denote the most common causes

Summary:
🏁 Transudative DDx = hydrostatic, oncotic, & diaphragmatic etiologies
🏁 Exudative DDx = infectious or non-infectious
🏁 Stratify non-infectious exudates by organ system & other helpful buckets
🏁 Transudative DDx = hydrostatic, oncotic, & diaphragmatic etiologies
🏁 Exudative DDx = infectious or non-infectious
🏁 Stratify non-infectious exudates by organ system & other helpful buckets
References:
1) @AndreMansoor (Whose pleural effusion DDx is available in the book Frameworks for IM. This schema is heavily adapted from that DDx.)
2) nejm.org
3) #c8" target="_blank" rel="noopener" onclick="event.stopPropagation()">emedicine.medscape.com
4) sciencedirect.com
1) @AndreMansoor (Whose pleural effusion DDx is available in the book Frameworks for IM. This schema is heavily adapted from that DDx.)
2) nejm.org
3) #c8" target="_blank" rel="noopener" onclick="event.stopPropagation()">emedicine.medscape.com
4) sciencedirect.com
Awesome summary of helpful fluid results:
جاري تحميل الاقتراحات...