

21 y/M
2018 - headache, LOW, low grade fever.Imaging had seller mass lesion for which referred to higher centre (didn't follow up).
2020 - Additionally, he developed polyuria/polydipsia, ED & intermittent episodes of hypoglycemia.
#Endotwitter
#Neurotwitter
#Hemetwitter
1/n
2018 - headache, LOW, low grade fever.Imaging had seller mass lesion for which referred to higher centre (didn't follow up).
2020 - Additionally, he developed polyuria/polydipsia, ED & intermittent episodes of hypoglycemia.
#Endotwitter
#Neurotwitter
#Hemetwitter
1/n
Heterogeneously enhancing lesion in infundibulum. (2018). 2/n
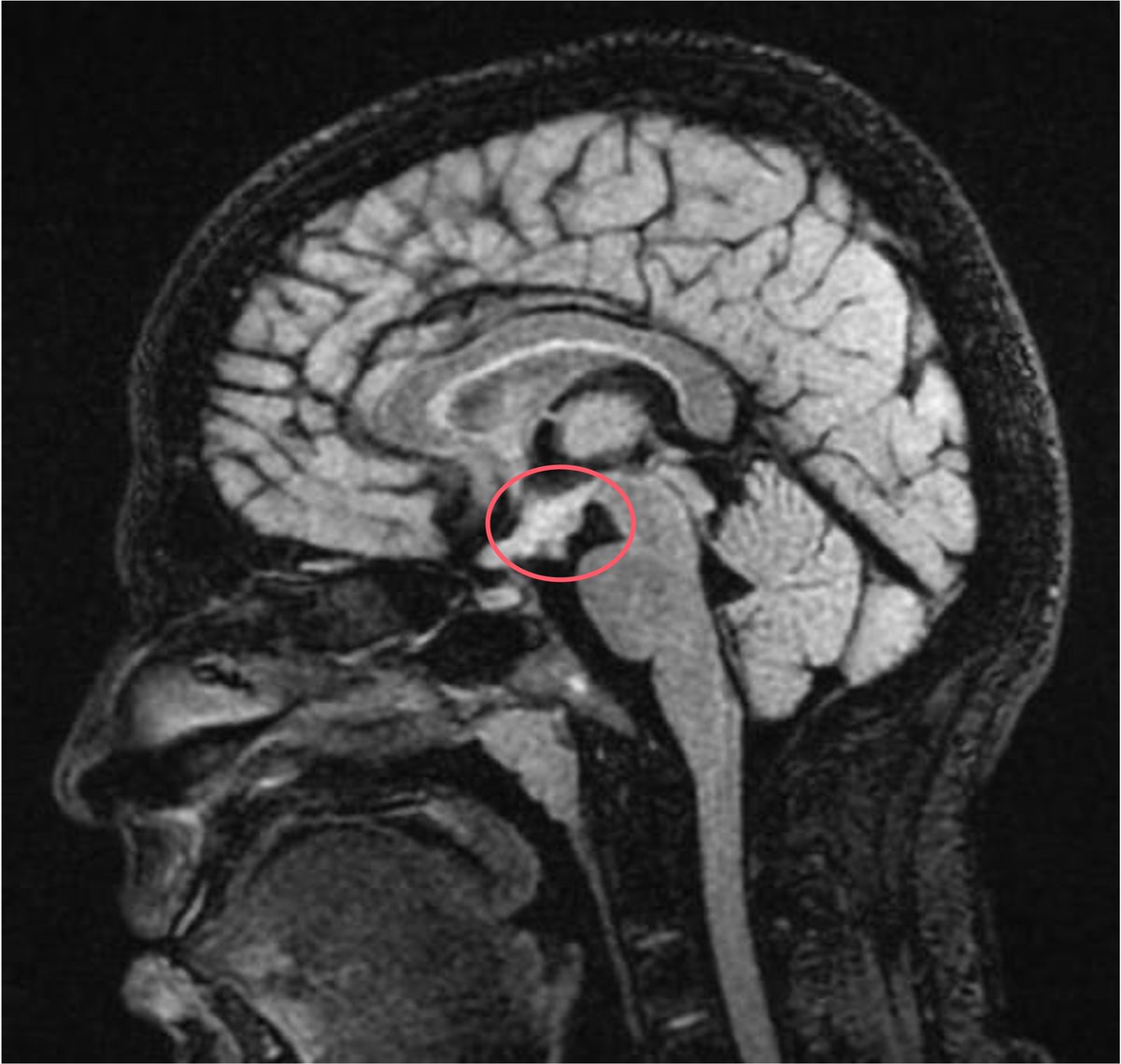
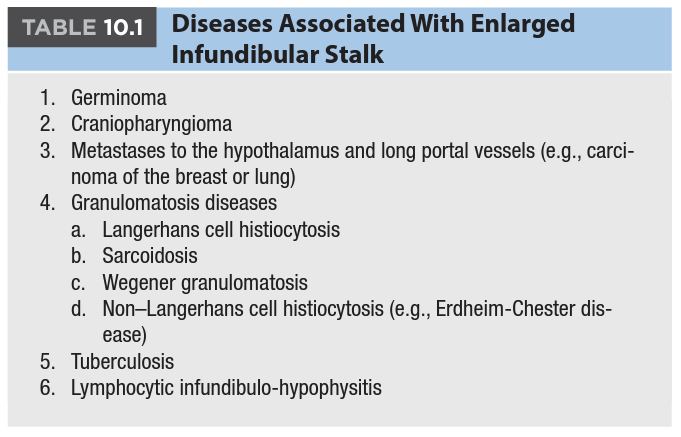
Causes of stalk thickening with such clinical history?
3/n
3/n
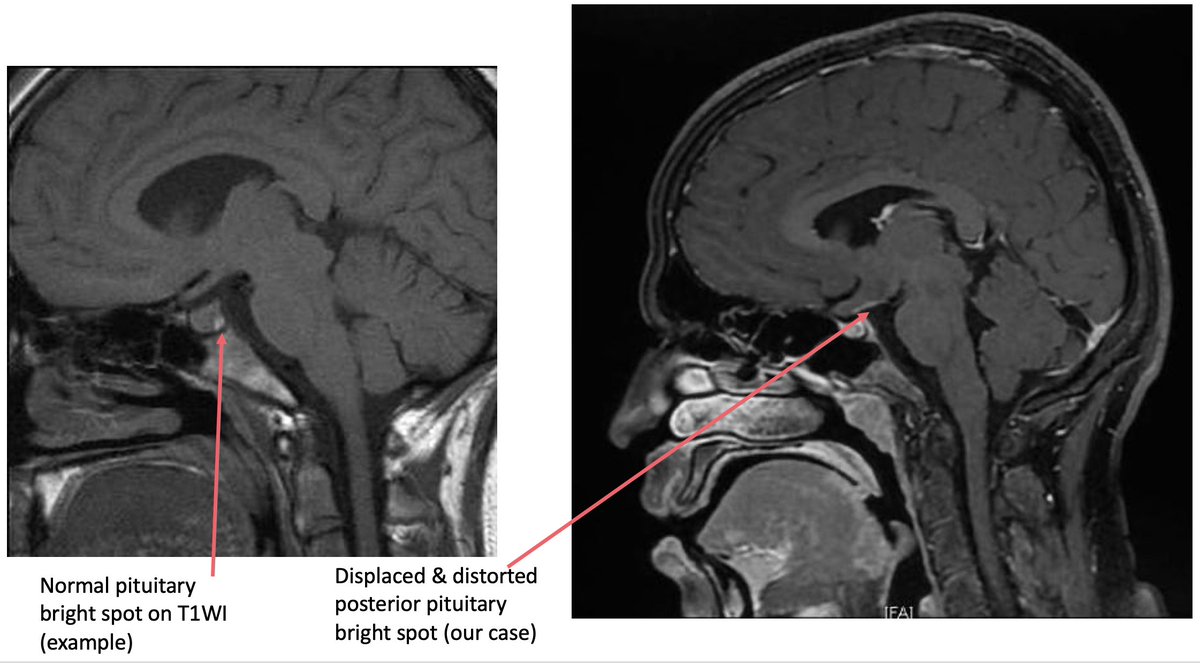
At the time of polyuria/polydipsia (osmotic causes ruled out, clinically diagnosed as CDI) (2020), following was the MRI finding - displaced & distorted pituitary bright spot (right).4/n
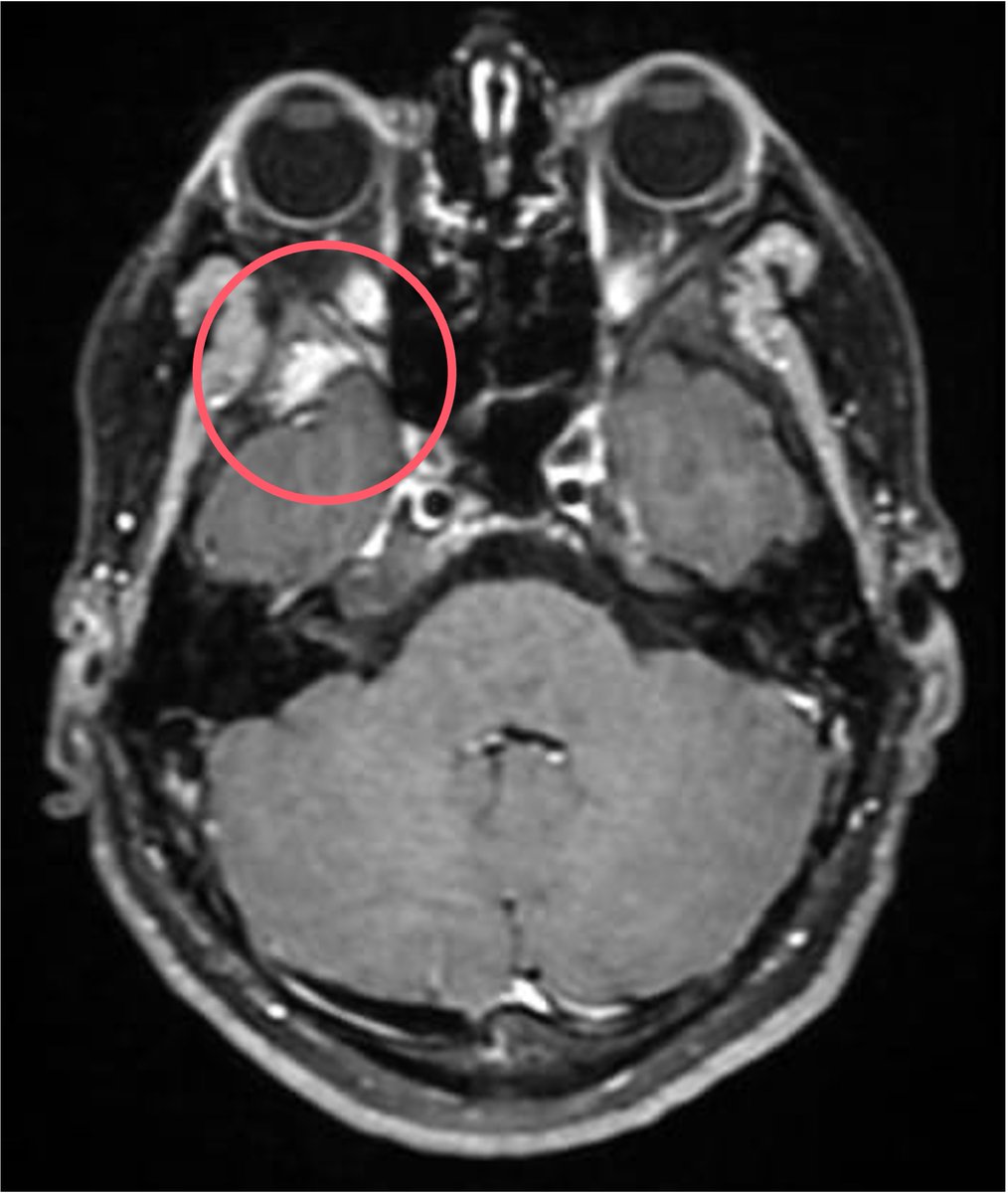
Coronal view (2020) showed right sphenoid bone involvement.
Diagnosis of LCH was suspected and was give Vinblastine + Prednisone (LCH III protocol) 5/n
Diagnosis of LCH was suspected and was give Vinblastine + Prednisone (LCH III protocol) 5/n
Following initial symptomatic relief, the patient again started having headache & worsening weight loss. Polyuria was controlled on dDAVP.
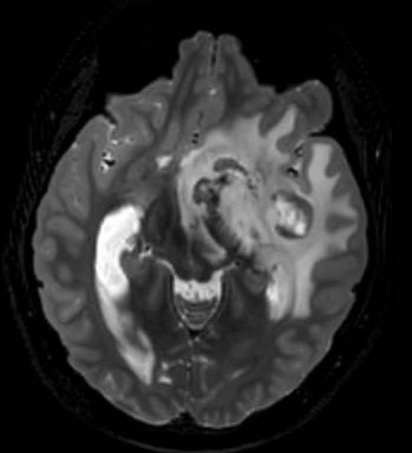
2022 - presented with right sided hemiparesis & right UL dystonia.
MRI - left gangiocapsular involvement with perilesional edema. 6/n
2022 - presented with right sided hemiparesis & right UL dystonia.
MRI - left gangiocapsular involvement with perilesional edema. 6/n
At this time, it was decided to biopsy the patient & left craniotomy was done for the same.
HPE & IHC revealed - primary CNS DLBCL (post GCB).
IHC negative for langerin, CD1a & S100.
He was put on R-CHOP and doing fine currently.
7/7
HPE & IHC revealed - primary CNS DLBCL (post GCB).
IHC negative for langerin, CD1a & S100.
He was put on R-CHOP and doing fine currently.
7/7
Loading suggestions...