

🦀 Approach to Lymphomas 🦀
Re-sharing this updated framework with some increased organization, new references, & more specific terminology.
Let's take this ride again!
Re-sharing this updated framework with some increased organization, new references, & more specific terminology.
Let's take this ride again!

🔬 Previously, a lymphoid neoplasm of the marrow/blood = leukemia, solid lymph node (LN) neoplasm = lymphoma
🔬 However, many "lymphomas" can evolve into "leukemia," & vice-versa
🔬 Now, the WHO classifies lymphoid neoplasms based on cell of origin
🔬 However, many "lymphomas" can evolve into "leukemia," & vice-versa
🔬 Now, the WHO classifies lymphoid neoplasms based on cell of origin
The WHO's 5th edition of lymphoid neoplasm classification is quite long.
In addition to what I'll call the "classic" lymphoid neoplasms (lymphomas), the latest list includes plasma cell neoplasms (eg plasma cell myeloma) & newly included diseases (eg IgG4-RD).
In addition to what I'll call the "classic" lymphoid neoplasms (lymphomas), the latest list includes plasma cell neoplasms (eg plasma cell myeloma) & newly included diseases (eg IgG4-RD).
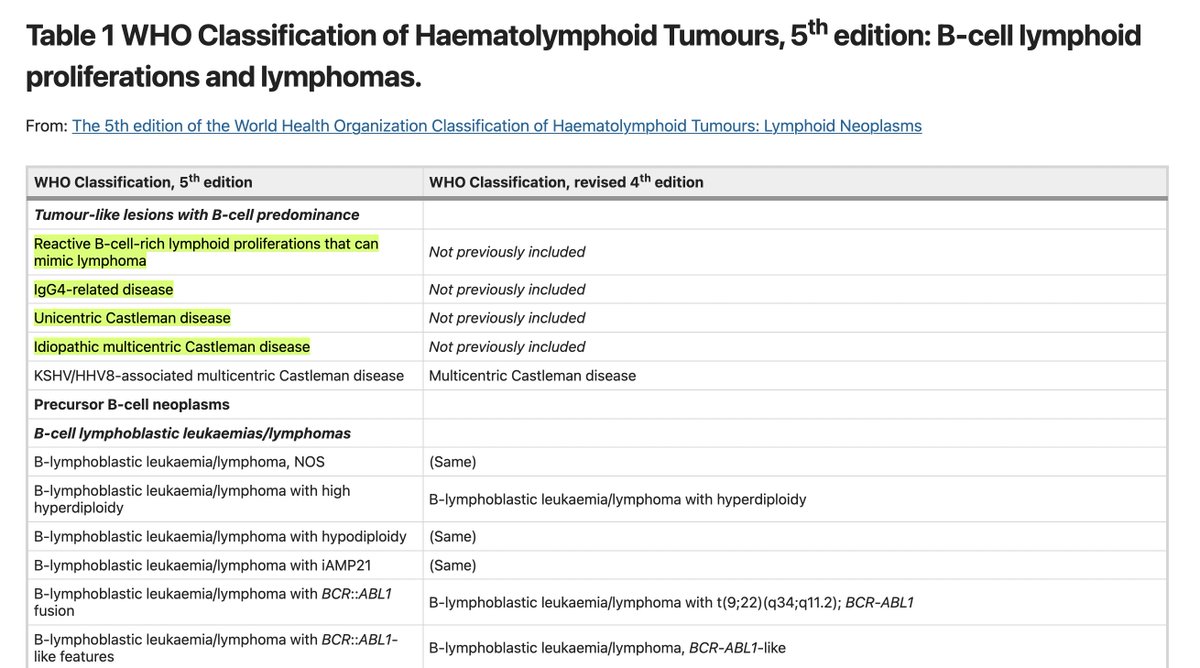
5th Edition of the WHO's Classification of Haematolymphoid Tumours is available here:
nature.com
nature.com
With that in mind, the following thread encompasses a diagnostic framework for lymphomas, which is the group of neoplasms that was stratified into Hodgkin vs. Non-Hodgkin subtypes by our med schools.
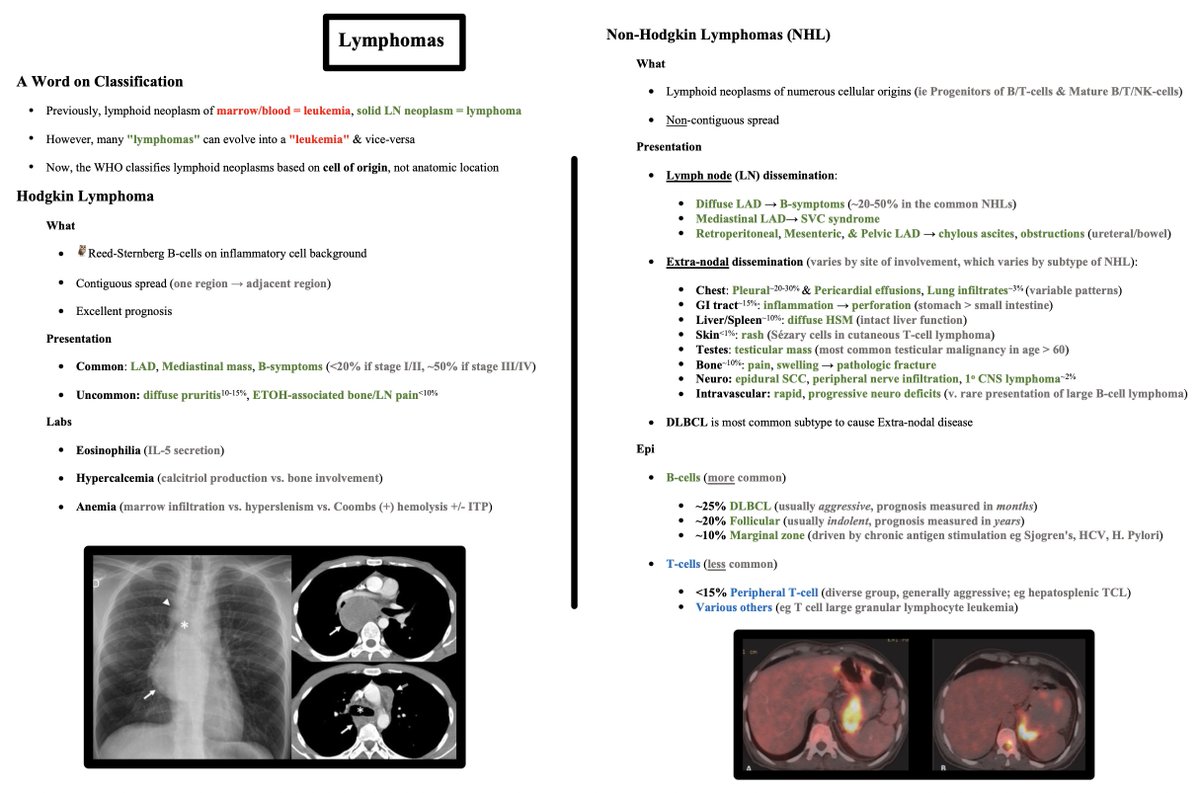
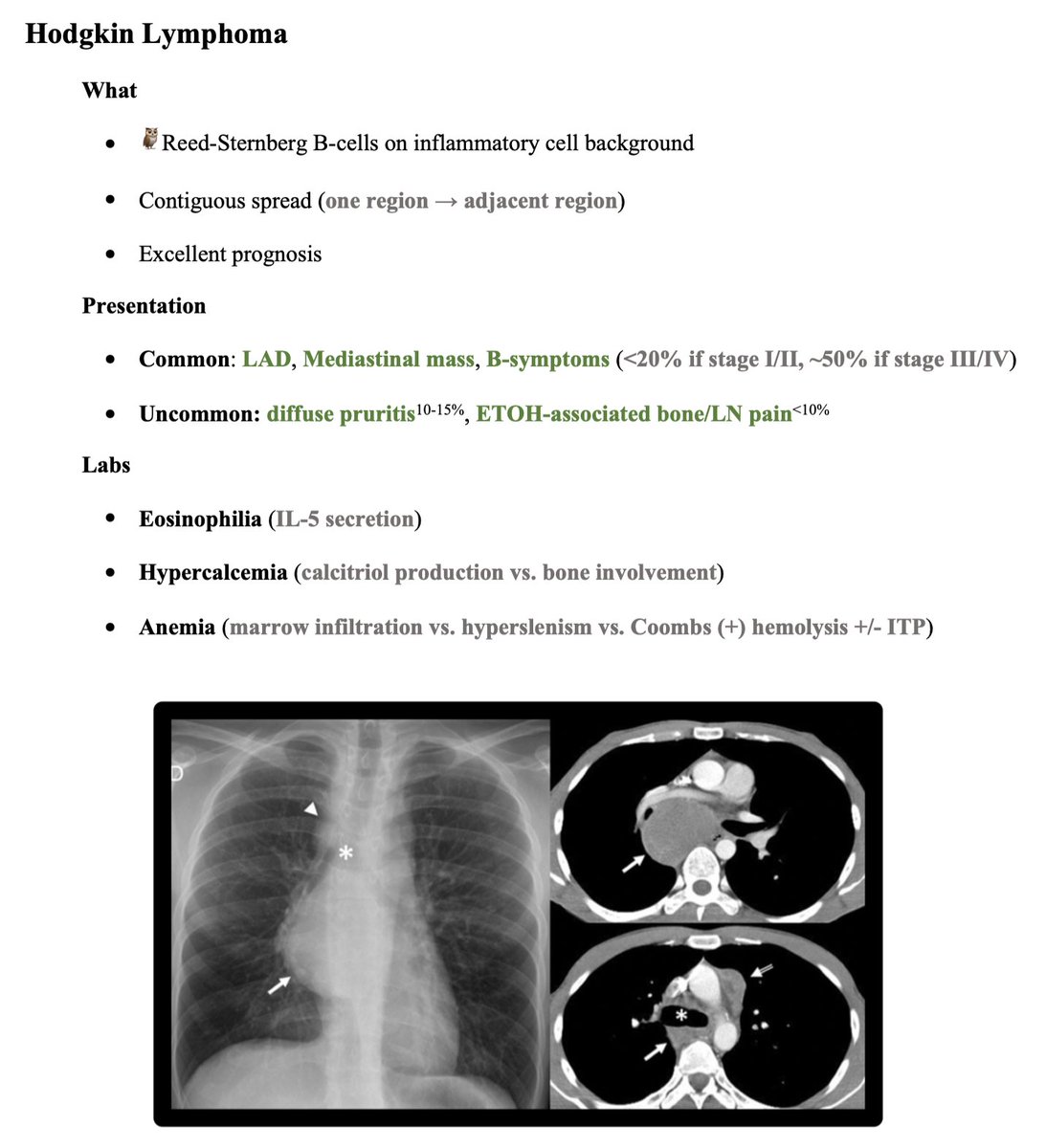
Hodgkin Lymphoma:
What?
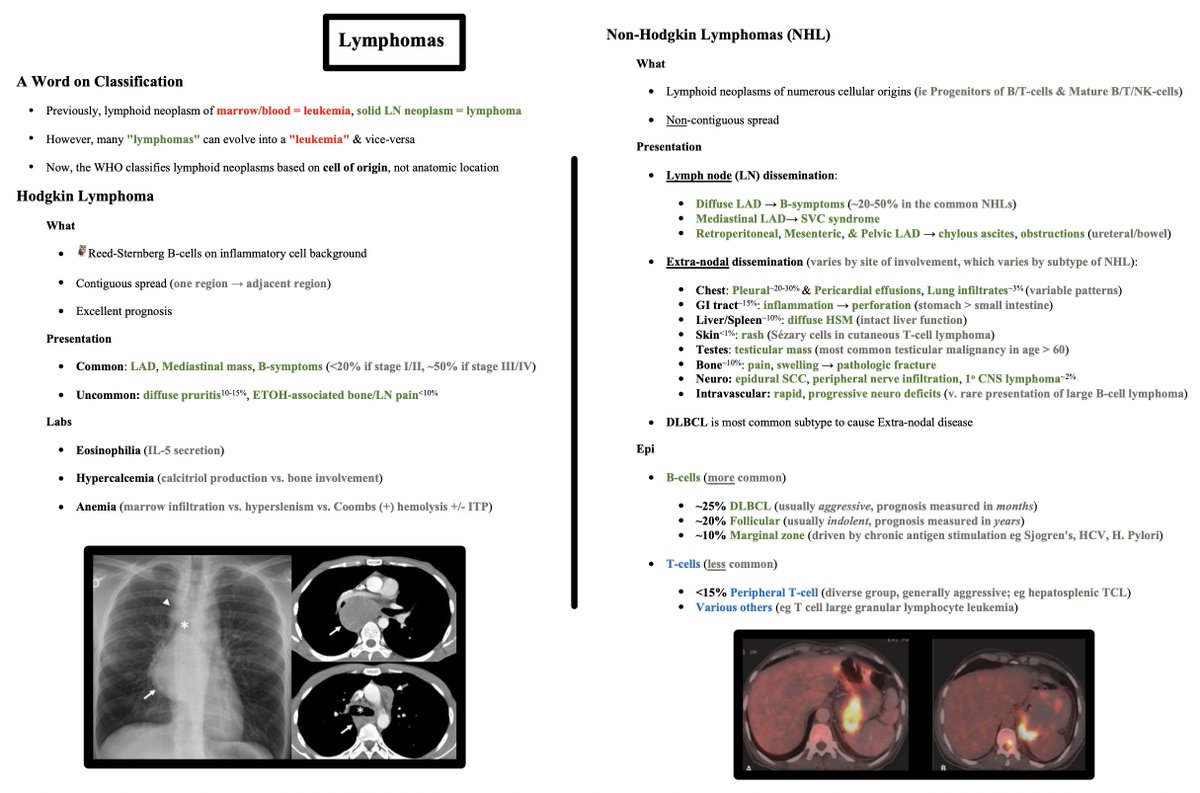
🦉 Reed-Sternberg B-cells
🦉 Contiguous LN spread
🦉 Excellent prognosis
Presentation?
🦉 Common: LAD, Mediastinal mass, B-symptoms (<20% if stage I/II, ~50% if stage III/IV)
🦉 Uncommon: diffuse pruritis (10-15%), ETOH-associated bone/ LN pain (<10%)
What?
🦉 Reed-Sternberg B-cells
🦉 Contiguous LN spread
🦉 Excellent prognosis
Presentation?
🦉 Common: LAD, Mediastinal mass, B-symptoms (<20% if stage I/II, ~50% if stage III/IV)
🦉 Uncommon: diffuse pruritis (10-15%), ETOH-associated bone/ LN pain (<10%)
Labs may show:
🦉 Eosinophilia (IL-5 secretion)
🦉 Hypercalcemia (calcitriol production vs. bone involvement)
🦉 Anemia (marrow infiltration vs. hypersplenism vs. Coombs (+) hemolysis +/- ITP)
🦉 Eosinophilia (IL-5 secretion)
🦉 Hypercalcemia (calcitriol production vs. bone involvement)
🦉 Anemia (marrow infiltration vs. hypersplenism vs. Coombs (+) hemolysis +/- ITP)
Non-Hodgkin Lymphomas (NHL) are where things always got confusing for me.
NHLs are confusing because they encompass neoplasms of numerous cellular origins, namely:
🦀 Progenitors of B/T-cells
🦀 Mature B/T/NK-cells
What do they have in common?
Non-contiguous spread
NHLs are confusing because they encompass neoplasms of numerous cellular origins, namely:
🦀 Progenitors of B/T-cells
🦀 Mature B/T/NK-cells
What do they have in common?
Non-contiguous spread
In a med school review of NHLs, this is when the lecturer would group the NHLs by degree of aggressiveness, PTLD vs. non-PTLD (@MatthewHoMD), or some other way.
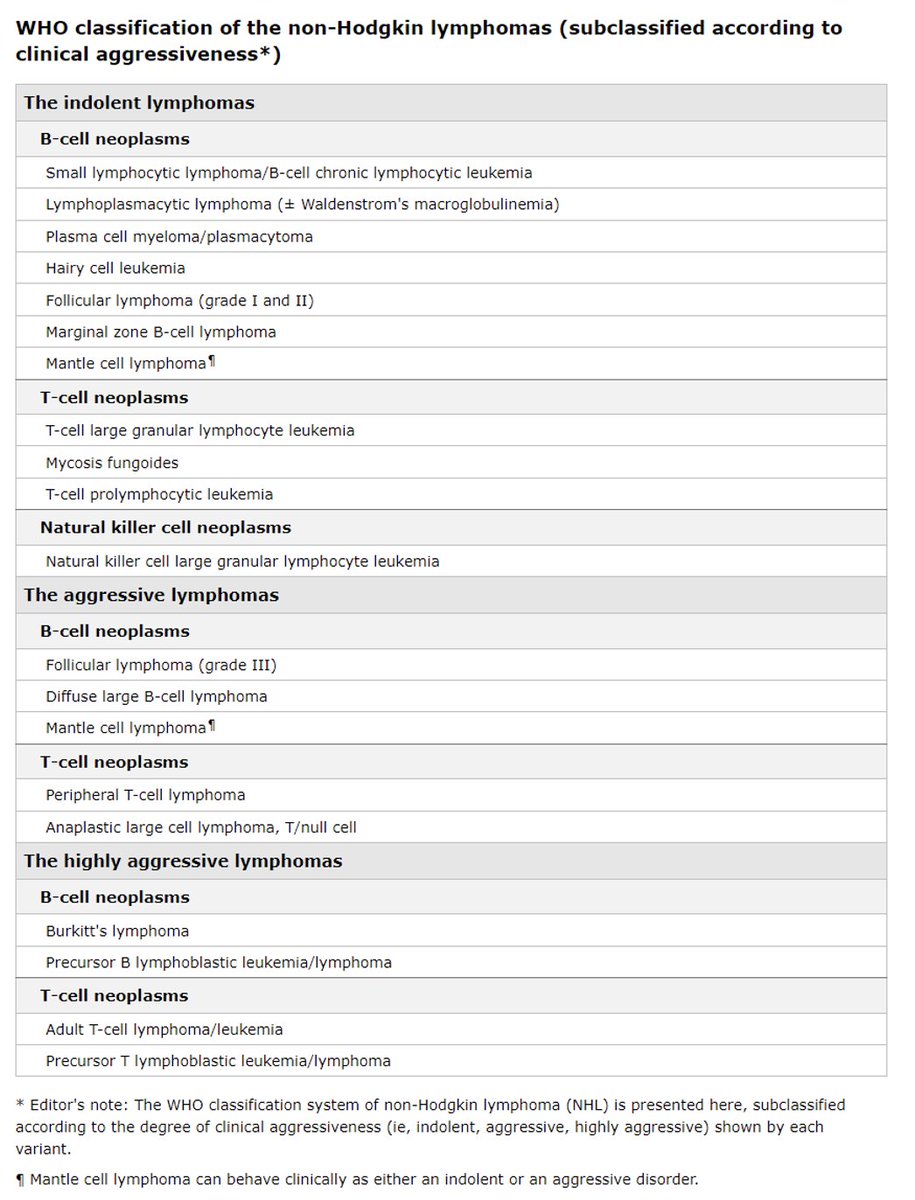
However, these types of groupings don't leave the diagnostician with a birds-eye view of the NHL landscape.
The goal of the following framework is to paint that picture so the diagnostician may spot one of these diseases using clinical signs & symptoms.
The goal of the following framework is to paint that picture so the diagnostician may spot one of these diseases using clinical signs & symptoms.
Signs & symptoms can be broken down into those related to LN dissemination vs. Extra-nodal dissemination.
Extra-nodal signs & symptoms varies by site of involvement, which varies by subtype of NHL.
📚 Note: DLBCL is most common subtype to cause Extra-nodal disease.
Extra-nodal signs & symptoms varies by site of involvement, which varies by subtype of NHL.
📚 Note: DLBCL is most common subtype to cause Extra-nodal disease.
LN dissemination leads to:
🟢 Diffuse LAD → B-symptoms
🟢 Mediastinal LAD → SVC syndrome
🟢 Retroperitoneal, Mesenteric, & Pelvic LAD → chylous ascites, obstructions (ureteral, bowel)
🟢 Diffuse LAD → B-symptoms
🟢 Mediastinal LAD → SVC syndrome
🟢 Retroperitoneal, Mesenteric, & Pelvic LAD → chylous ascites, obstructions (ureteral, bowel)
Extra-nodal signs & symptoms:
🫁 Chest: pleural & pericardial effusions, lung infiltrates (variable patterns)
🤮 GI tract: inflammation → perforation (stomach > small intestine eg colitis)
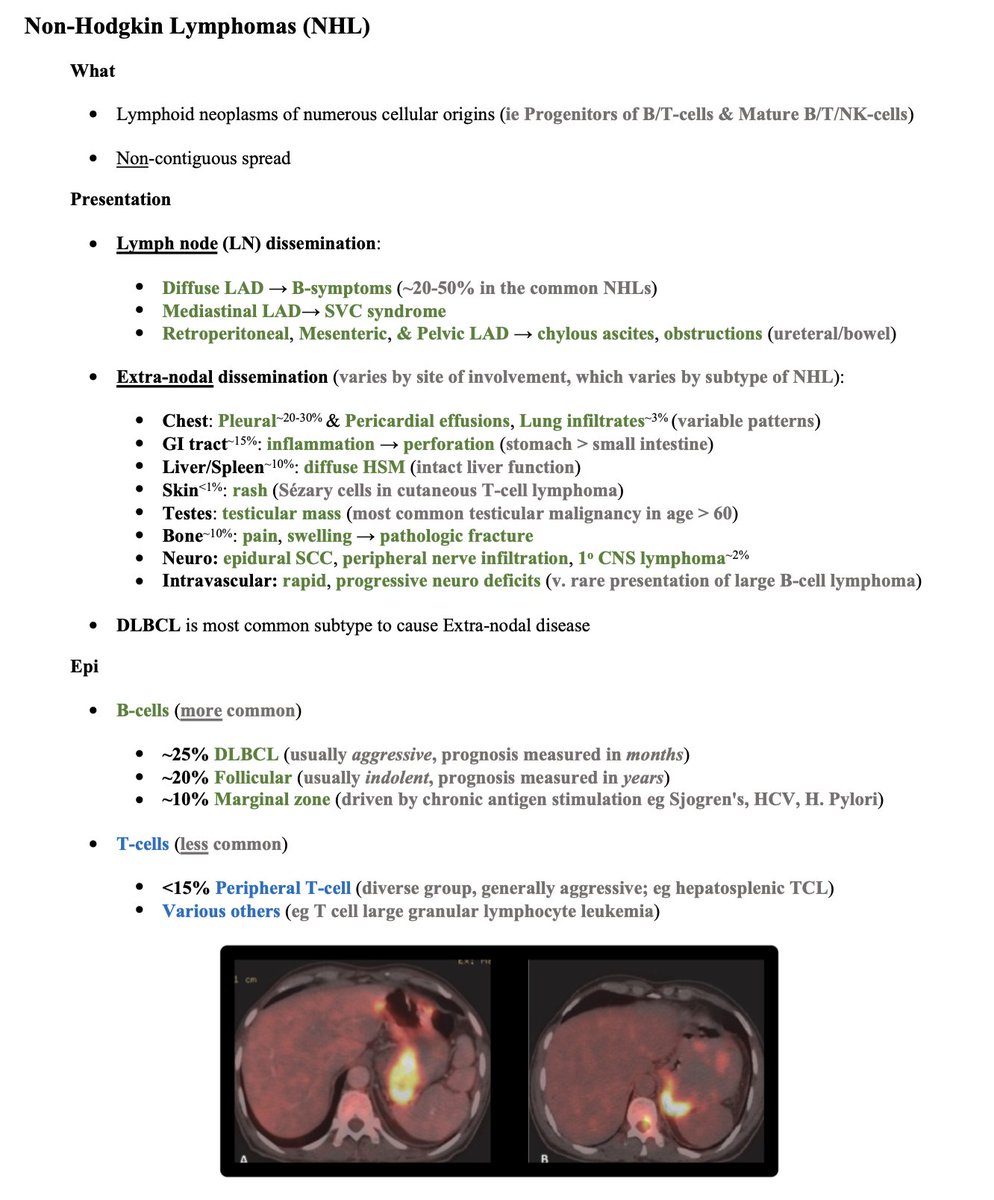
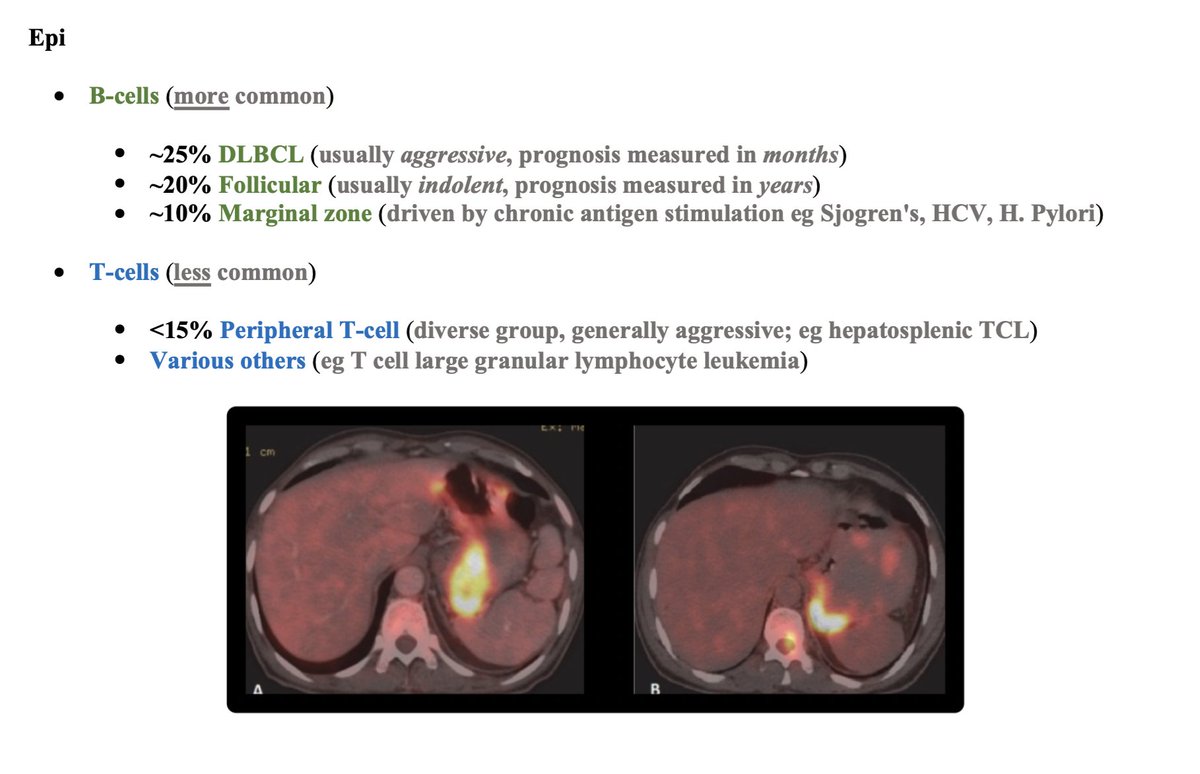
🟩 Liver/Spleen: diffuse hepatosplenomegaly (intact liver function)
🫁 Chest: pleural & pericardial effusions, lung infiltrates (variable patterns)
🤮 GI tract: inflammation → perforation (stomach > small intestine eg colitis)
🟩 Liver/Spleen: diffuse hepatosplenomegaly (intact liver function)
🧗 Skin: rash (Sezary cells in cutaneous T-cell lymphoma)
🍒 Testes: testicular mass (most common testicular malignancy in age > 60)
🦴 Bone: pain, swelling → pathologic fracture
🧠 Neuro: epidural SCC, peripheral nerve infiltration, primary CNS lymphoma
🍒 Testes: testicular mass (most common testicular malignancy in age > 60)
🦴 Bone: pain, swelling → pathologic fracture
🧠 Neuro: epidural SCC, peripheral nerve infiltration, primary CNS lymphoma
🩸 Intravascular: rapid, progressive neuro deficits (very rare presentation of large B-cell lymphoma)
Some very basic epidemiology is also helpful in framing NHLs.
Break it down into B-cell vs. T-cell subtypes
Break it down into B-cell vs. T-cell subtypes
🟢 B-cell subtypes = more common (~25% DLBCL, ~20% follicular, ~10% marginal)
🔵 T-cell subtypes = less common (<15% peripheral T cell, which is a diverse group of generally aggressive neoplasms)
🔵 T-cell subtypes = less common (<15% peripheral T cell, which is a diverse group of generally aggressive neoplasms)
🏁 Let me know how to make this framework better! Thanks for reading!
References:
1) nature.com
2) ncbi.nlm.nih.gov
3) #H2" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com
4) #H8" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com
5) ashpublications.org
1) nature.com
2) ncbi.nlm.nih.gov
3) #H2" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com
4) #H8" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com
5) ashpublications.org
Review of SVC Syndrome here:
@CharlesMilrod
@CharlesMilrod
جاري تحميل الاقتراحات...