

We have an effective toolkit to help many people living with IBD.
When deployed early in the disease course we can achieve deep and sustained remission for many patients.
The following strategy [👇] is not perfect, but is cost-effective and can be adopted widely.
NEW thread 🧵
When deployed early in the disease course we can achieve deep and sustained remission for many patients.
The following strategy [👇] is not perfect, but is cost-effective and can be adopted widely.
NEW thread 🧵
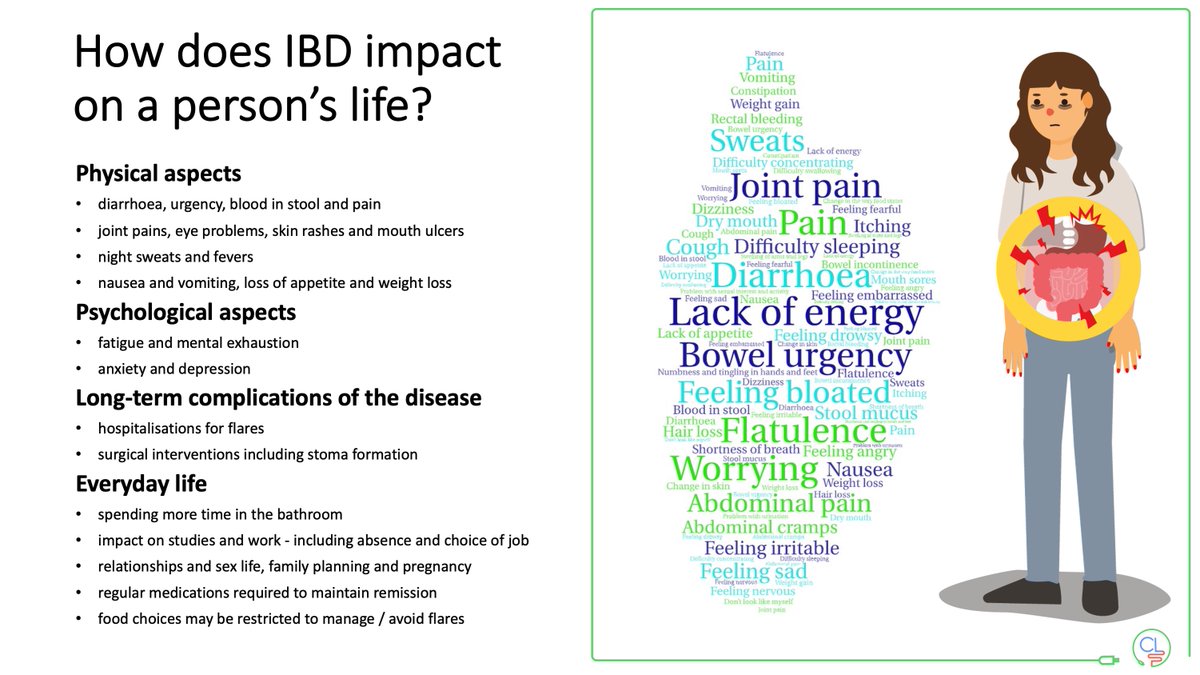
Crohn's disease and ulcerative colitis can have a significant impact on a person's life:
• physically
• psychologically
• complications of disease and drugs
• aspects of everyday life from work to relationships
• physically
• psychologically
• complications of disease and drugs
• aspects of everyday life from work to relationships
Early effective therapy should aim for healing beyond the gut.
The figure shows
• tight control of intestinal inflammation AND
• tight control of psychosocial aspects
Read the wonderful review by @drlauriekeefer and @DrAilsaHart in @AGA_Gastro
gastrojournal.org
The figure shows
• tight control of intestinal inflammation AND
• tight control of psychosocial aspects
Read the wonderful review by @drlauriekeefer and @DrAilsaHart in @AGA_Gastro
gastrojournal.org


@drlauriekeefer @DrAilsaHart @AGA_Gastro We can break the therapeutic ceiling using tools already to hand:
• Early diagnosis
• Risk stratification
• Improved care delivery
• Improved target-driven management
• Non-invasive monitoring (calpro and IUS)
• Early diagnosis
• Risk stratification
• Improved care delivery
• Improved target-driven management
• Non-invasive monitoring (calpro and IUS)

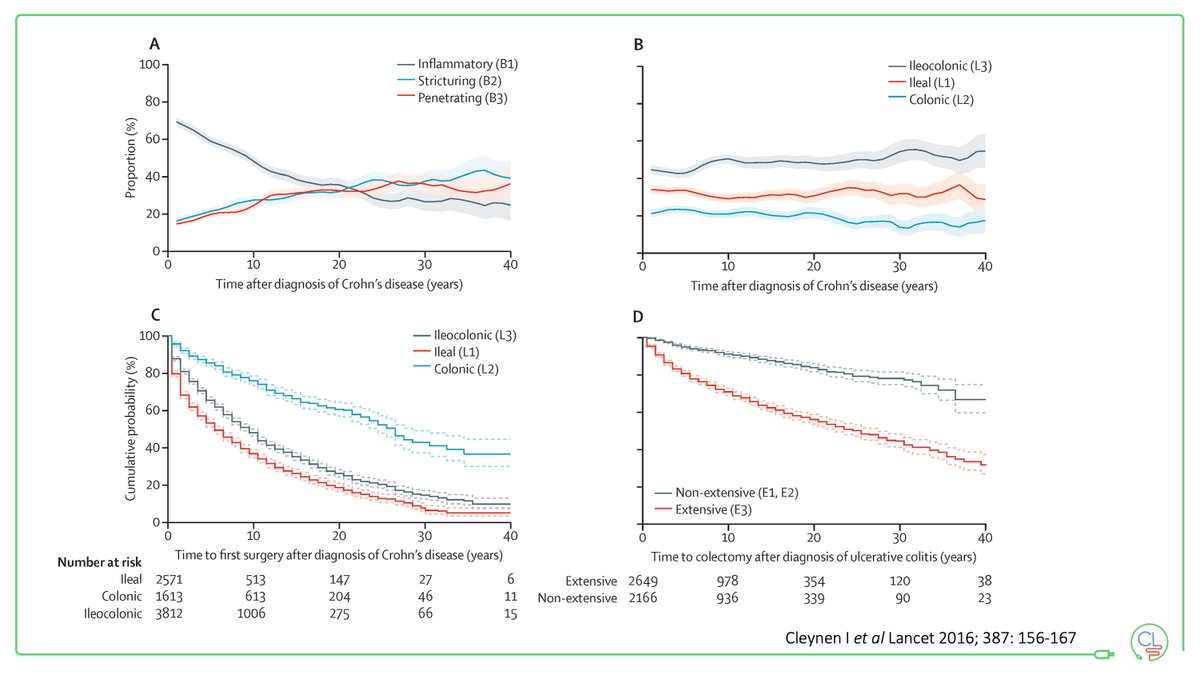
@drlauriekeefer @DrAilsaHart @AGA_Gastro In early Crohn's disease inflammation is predominant.
Many patients will progress over time to a stricturing or fistulising phenotype.
Disease location typically remains stable over time.
The inflammatory window of opportunity is when our treatments are most effective.
Many patients will progress over time to a stricturing or fistulising phenotype.
Disease location typically remains stable over time.
The inflammatory window of opportunity is when our treatments are most effective.
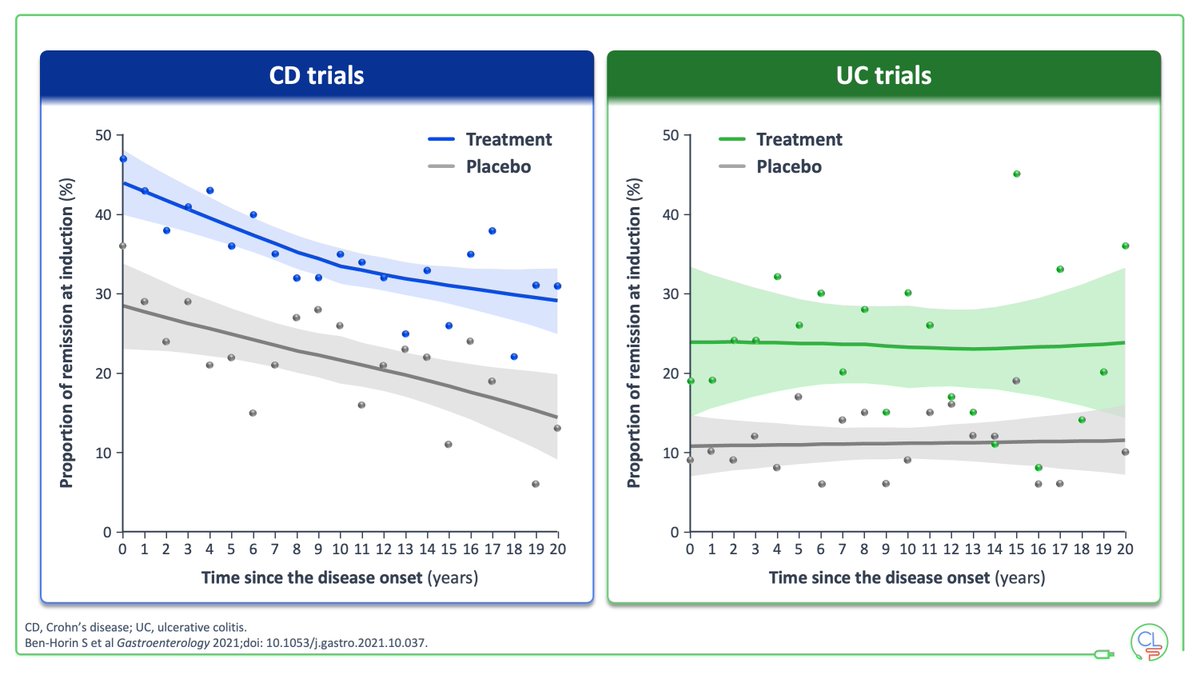
@drlauriekeefer @DrAilsaHart @AGA_Gastro The data from phase 3 RCTs is IBD show a discordant effect of disease during on outcomes in CD and UC
In Crohn's disease early advanced therapy is more effective
In UC this effect is not seen. Early effective control of flares is key here.
In Crohn's disease early advanced therapy is more effective
In UC this effect is not seen. Early effective control of flares is key here.
@drlauriekeefer @DrAilsaHart @AGA_Gastro It is important to have a robust treatment strategy
• what is the target?
• how will you know if you get there?
• what is your treatment optimisation strategy?
• what is the target?
• how will you know if you get there?
• what is your treatment optimisation strategy?

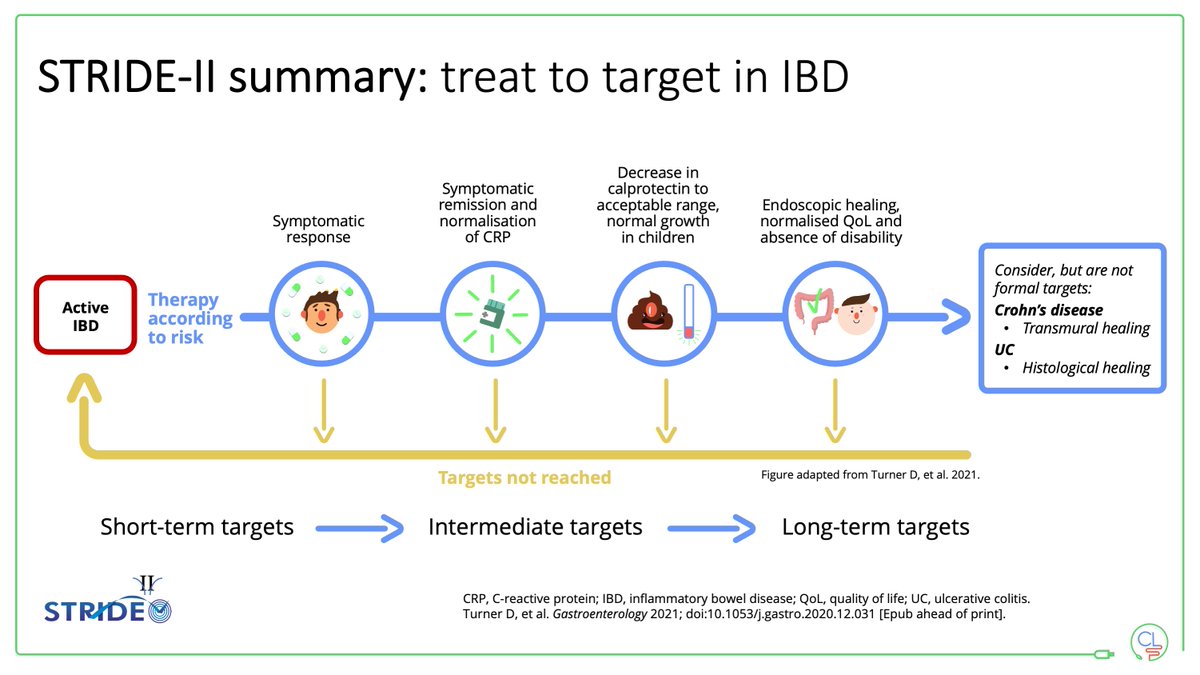
@drlauriekeefer @DrAilsaHart @AGA_Gastro STRIDE-2: Treat-to-target with short- mid- and long-term targets
Note additions from STRIDE-1
• formalises use of calprotectin
• normalisation of growth in children
• normalised quality of life and absence of disability
Transmural & histological healing - not yet ? STRIDE-3
Note additions from STRIDE-1
• formalises use of calprotectin
• normalisation of growth in children
• normalised quality of life and absence of disability
Transmural & histological healing - not yet ? STRIDE-3
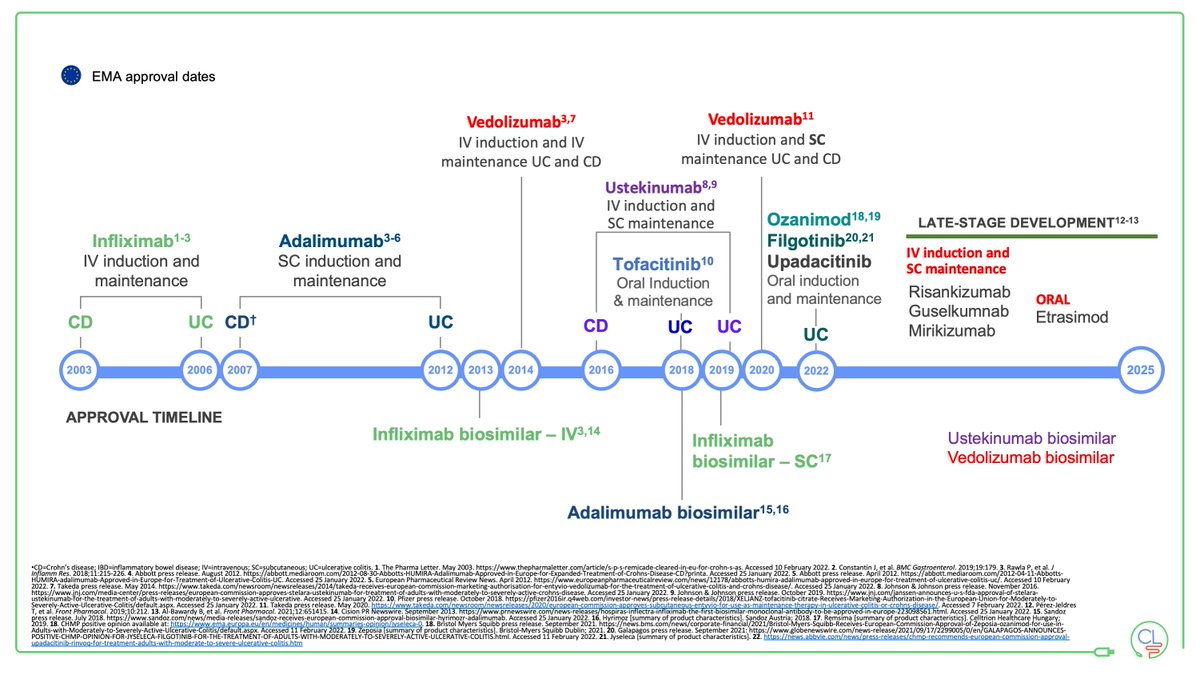
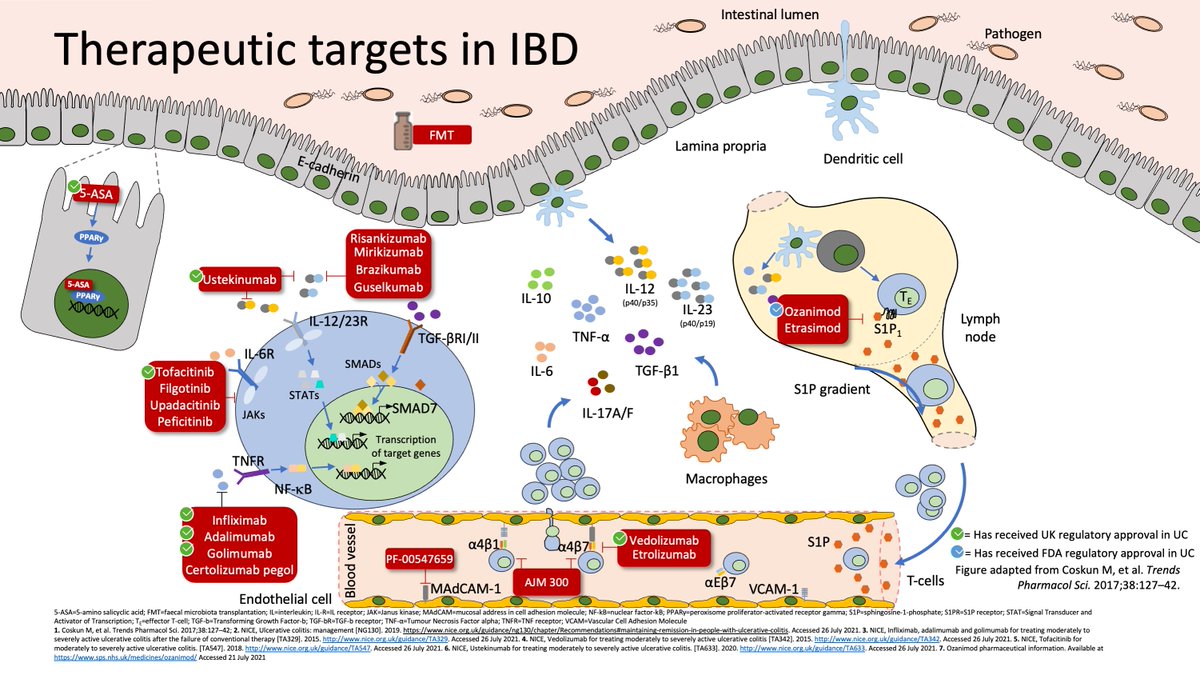
@drlauriekeefer @DrAilsaHart @AGA_Gastro The therapeutic toolkit is in healthy shape
• Advanced therapy is affordable to all with biosimilar anti-TNF
• Biosimilar VEDO & USTE within 2y
• Small molecules are here at an attractive price point
• Combinations of therapies here soon to smash that therapeutic ceiling
• Advanced therapy is affordable to all with biosimilar anti-TNF
• Biosimilar VEDO & USTE within 2y
• Small molecules are here at an attractive price point
• Combinations of therapies here soon to smash that therapeutic ceiling
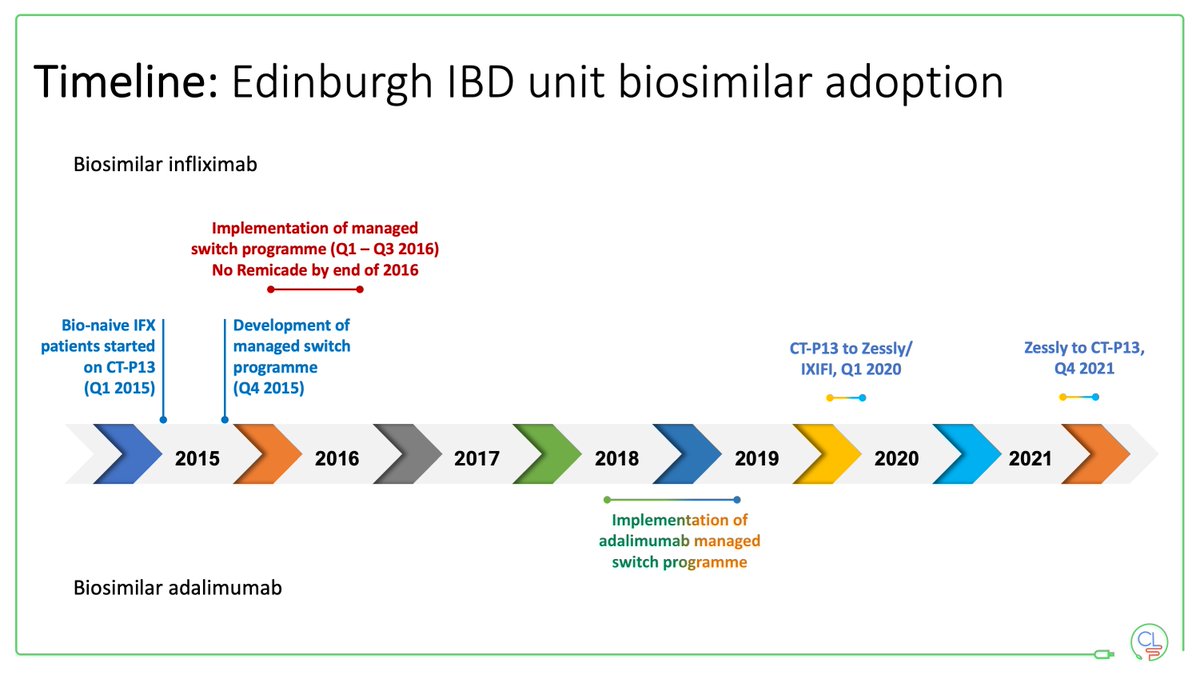
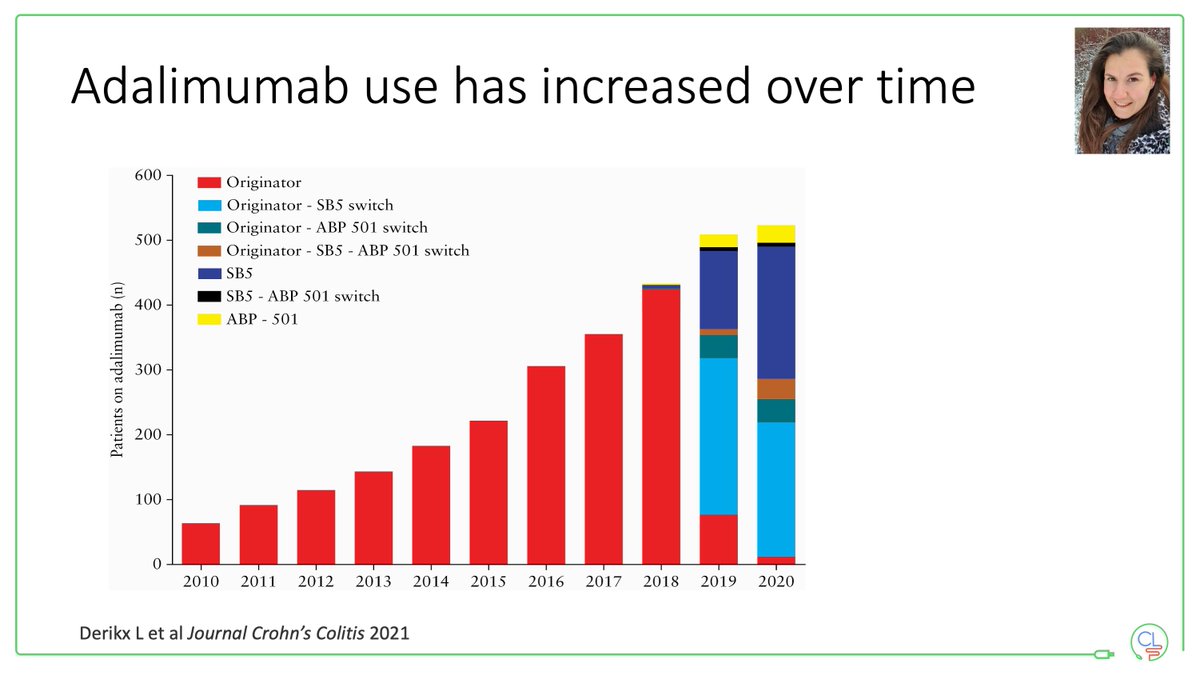
@drlauriekeefer @DrAilsaHart @AGA_Gastro We have been using biosimilars for >7y
This has transformed our access to effective therapy:
• anti-TNF based strategy early in Crohn's disease
• expedient management of flares in UC
• dose optimisation of IFX & ADA
Plus reinvestment into service & access to new molecules
This has transformed our access to effective therapy:
• anti-TNF based strategy early in Crohn's disease
• expedient management of flares in UC
• dose optimisation of IFX & ADA
Plus reinvestment into service & access to new molecules
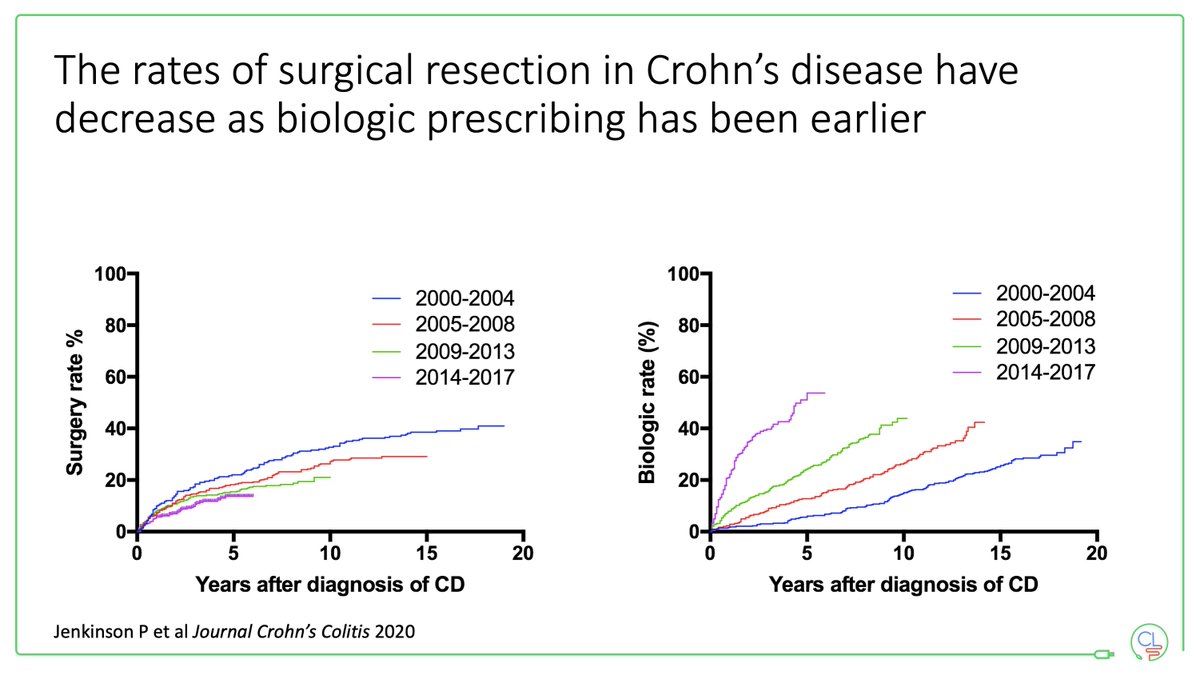
@drlauriekeefer @DrAilsaHart @AGA_Gastro In Crohn's disease we have seen a major change in the positioning of biologics
In 2000-2004 patients "earned their right to a biologic" late in the disease course
In 2014-2017 you can see the shape of the curve change - top-down therapy
Surgical rates have dropped over time
In 2000-2004 patients "earned their right to a biologic" late in the disease course
In 2014-2017 you can see the shape of the curve change - top-down therapy
Surgical rates have dropped over time
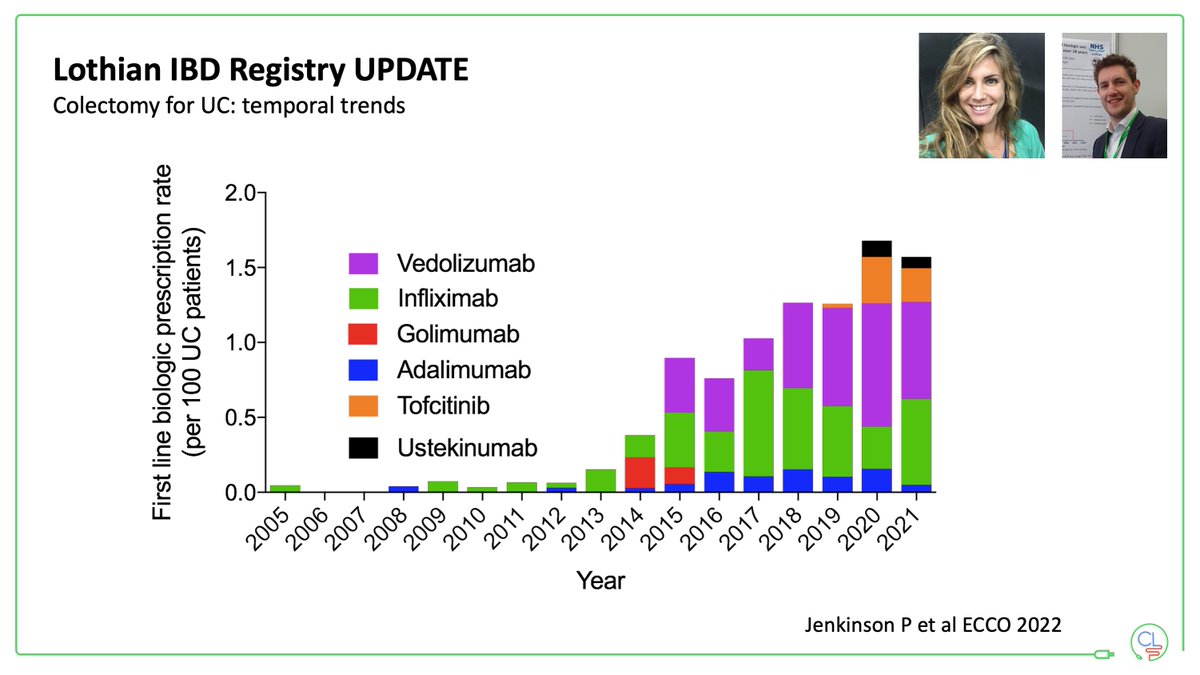
@drlauriekeefer @DrAilsaHart @AGA_Gastro In UC we used very little advanced therapy prior to 2015
This changed with
• NICE MTA for anti-TNF in UC
• approval of vedolizumab
Then we have approvals for USTE and TOFA
This is first-line prescriptions only
This changed with
• NICE MTA for anti-TNF in UC
• approval of vedolizumab
Then we have approvals for USTE and TOFA
This is first-line prescriptions only
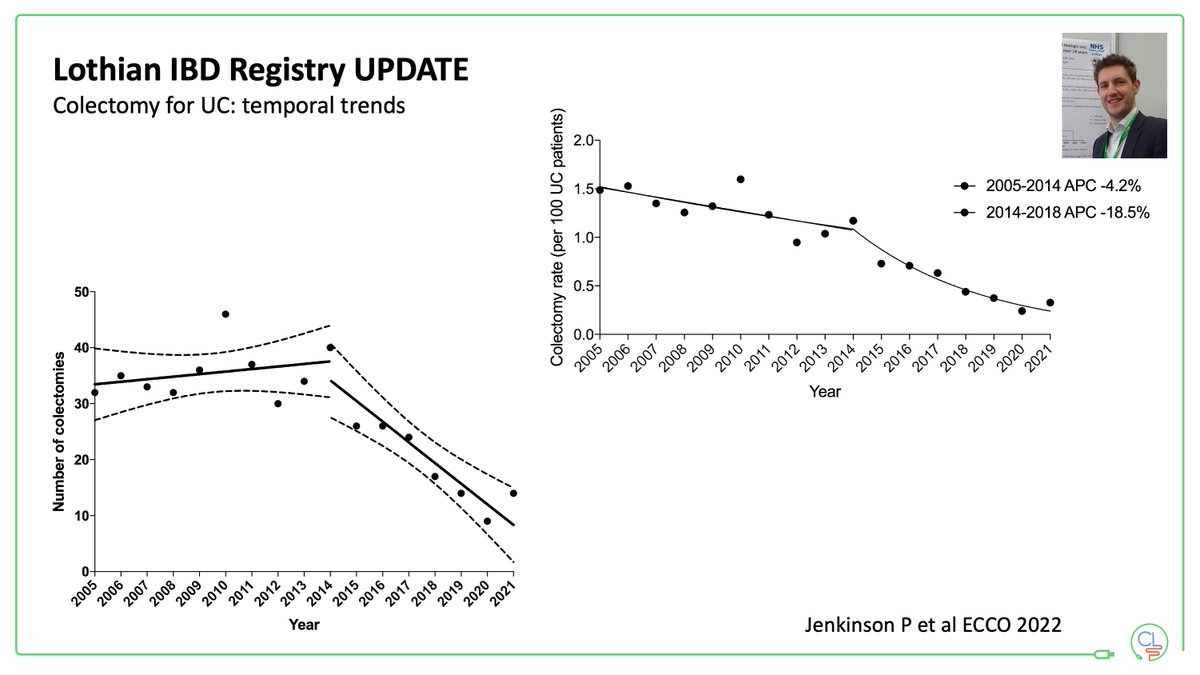
@drlauriekeefer @DrAilsaHart @AGA_Gastro Over the last 10 years we have seen a significant drop in colectomies for UC
The biggest shift happens in 2014-15 when our use of advance therapies goes up
Colectomy remains important for many patients, but fewer now thanks to better therapies
The biggest shift happens in 2014-15 when our use of advance therapies goes up
Colectomy remains important for many patients, but fewer now thanks to better therapies
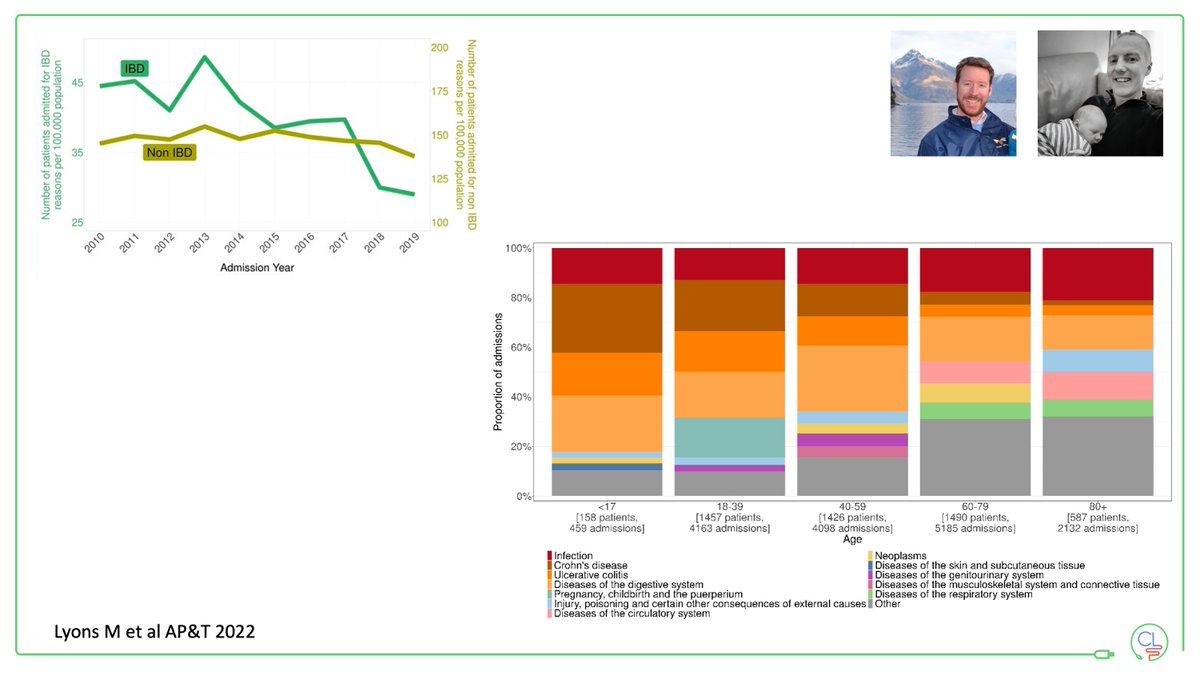
@drlauriekeefer @DrAilsaHart @AGA_Gastro We've seen a drop in hospitalisations for IBD in our Lothian population
Hospitalisations for non-IBD reasons stable over the last 10 years
Note how as patients get older the reasons for hospitalisation shift
• more IBD in younger ages
• more infection in older ages
Hospitalisations for non-IBD reasons stable over the last 10 years
Note how as patients get older the reasons for hospitalisation shift
• more IBD in younger ages
• more infection in older ages
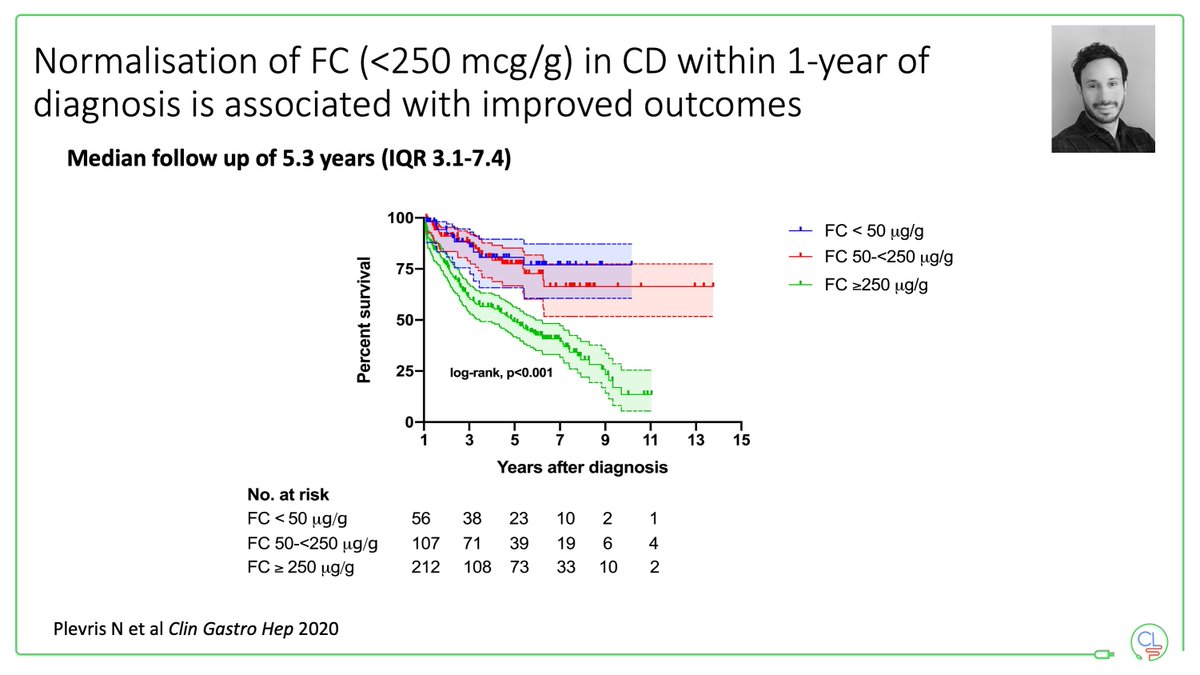
@drlauriekeefer @DrAilsaHart @AGA_Gastro The key to improved outcomes is early effective therapy
In Crohn's disease many patients start on anti-TNF first line
But not everyone needs this - how to tell?
Monitor FCAL - if it stays >250 then start a biologic
In Crohn's disease many patients start on anti-TNF first line
But not everyone needs this - how to tell?
Monitor FCAL - if it stays >250 then start a biologic
@drlauriekeefer @DrAilsaHart @AGA_Gastro This is in keeping with the key learnings from the CALM study
Early in Crohn's disease use a treat-to-target paradigm based on anti-TNF therapy = good outcomes at one year
The biggest trigger for treatment change in CALM was FCAL
Early in Crohn's disease use a treat-to-target paradigm based on anti-TNF therapy = good outcomes at one year
The biggest trigger for treatment change in CALM was FCAL

@drlauriekeefer @DrAilsaHart @AGA_Gastro With SEAVUE we now learn that USTE and ADA are equally effective agents
Early in Crohn's disease after 1 year of therapy they look very similar
? longer-term advantage with USTE
? better effect with dose optimised ADA
Read my thoughts here charlielees.substack.com
Early in Crohn's disease after 1 year of therapy they look very similar
? longer-term advantage with USTE
? better effect with dose optimised ADA
Read my thoughts here charlielees.substack.com

@drlauriekeefer @DrAilsaHart @AGA_Gastro Based on cost alone, first-line advanced therapy for the majority of patients with Crohn's disease now is anti-TNF therapy
• IFX plus AZA for patients with highest risk phenotype
• ADA monotherapy for patients with moderate disease
This is our standard practice
• IFX plus AZA for patients with highest risk phenotype
• ADA monotherapy for patients with moderate disease
This is our standard practice
@drlauriekeefer @DrAilsaHart @AGA_Gastro Adalimumab therapy now costs the same as optimised 5-ASA therapy
This still blows my mind!
It was previously unthinkable. We used to "if anti-TNF therapy was the same price as other therapies ..." and here we are.
This still blows my mind!
It was previously unthinkable. We used to "if anti-TNF therapy was the same price as other therapies ..." and here we are.
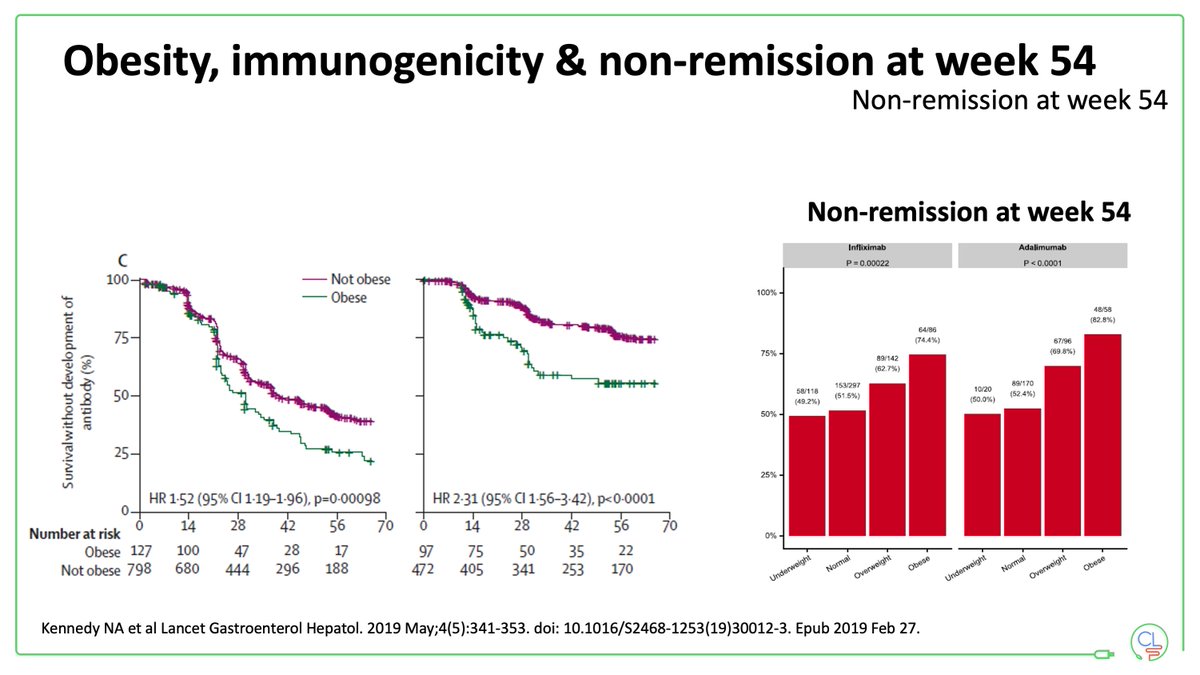
@drlauriekeefer @DrAilsaHart @AGA_Gastro The big problem with anti-TNF therapy is immunogenicity resulting in loss of response
Immunogenicity is driven by a number of factors including:
• obesity
• smoking
• HLA-DQA1*05
Optimised doses and concomitant immunosuppressant guided by TDM help to mitigate this
Immunogenicity is driven by a number of factors including:
• obesity
• smoking
• HLA-DQA1*05
Optimised doses and concomitant immunosuppressant guided by TDM help to mitigate this
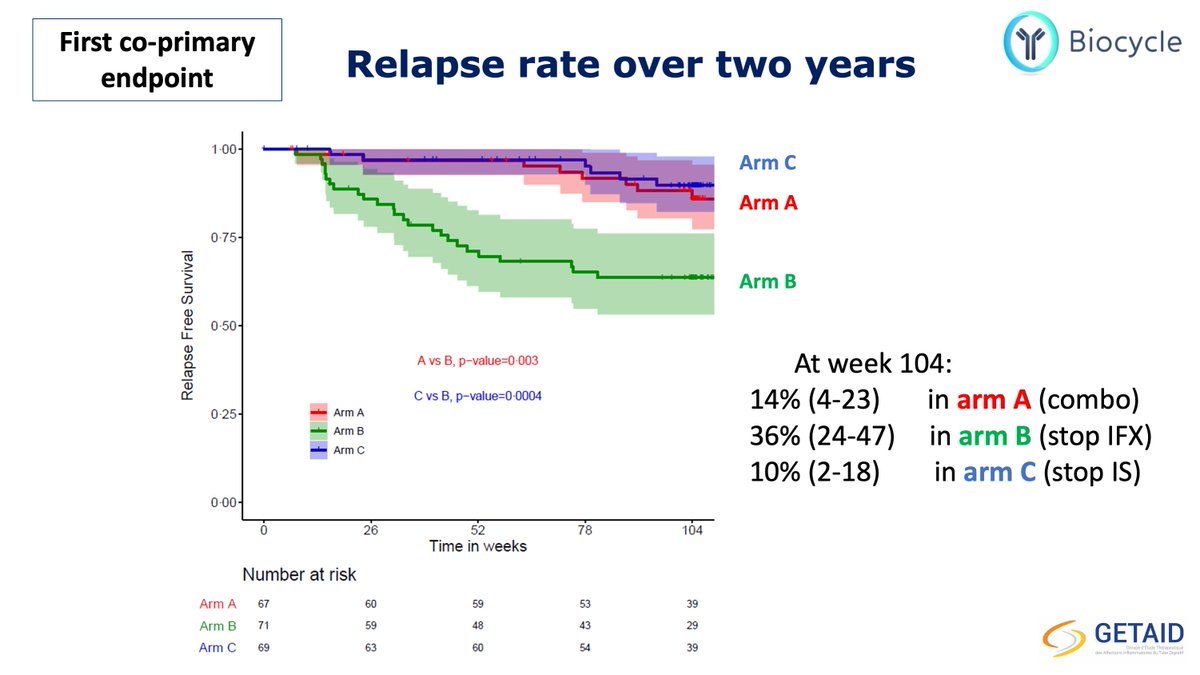
@drlauriekeefer @DrAilsaHart @AGA_Gastro The rates of relapse on stopping anti-TNF therapy are high
In STOP-IT 49& of CD patients relapsed by 1 year
In SPARE 36% of CD patients relapsed by 2 years
Therefore continue therapy OR stop with careful monitoring
Ready my thoughts here charlielees.substack.com
In STOP-IT 49& of CD patients relapsed by 1 year
In SPARE 36% of CD patients relapsed by 2 years
Therefore continue therapy OR stop with careful monitoring
Ready my thoughts here charlielees.substack.com
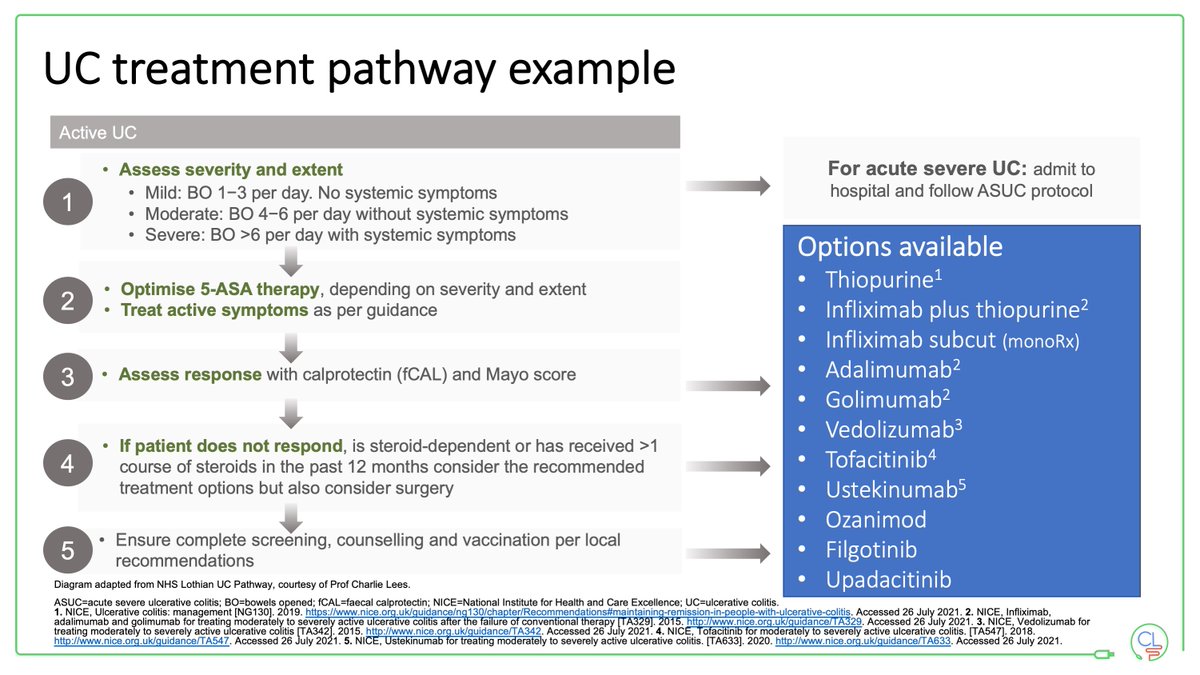
@drlauriekeefer @DrAilsaHart @AGA_Gastro In UC drug positioning is very interesting
• vedo is excellent first-line
• ada is much less effective in UC than CD
• IFX has a new lease of life with sc CT-P13
• TOFA, FILGO & UPA cheaper than originator biologics
Time for precision medicine to come of age and deliver
• vedo is excellent first-line
• ada is much less effective in UC than CD
• IFX has a new lease of life with sc CT-P13
• TOFA, FILGO & UPA cheaper than originator biologics
Time for precision medicine to come of age and deliver
@drlauriekeefer @DrAilsaHart @AGA_Gastro Precision medicine has largely failed in IBD up until now
We will get there and ambitious projects are underway including:
• large single cell sequencing efforts (cell-specific effects)
• ambitious microbiome profiling studies (e.g. IBD response)
This is a hard problem.
We will get there and ambitious projects are underway including:
• large single cell sequencing efforts (cell-specific effects)
• ambitious microbiome profiling studies (e.g. IBD response)
This is a hard problem.
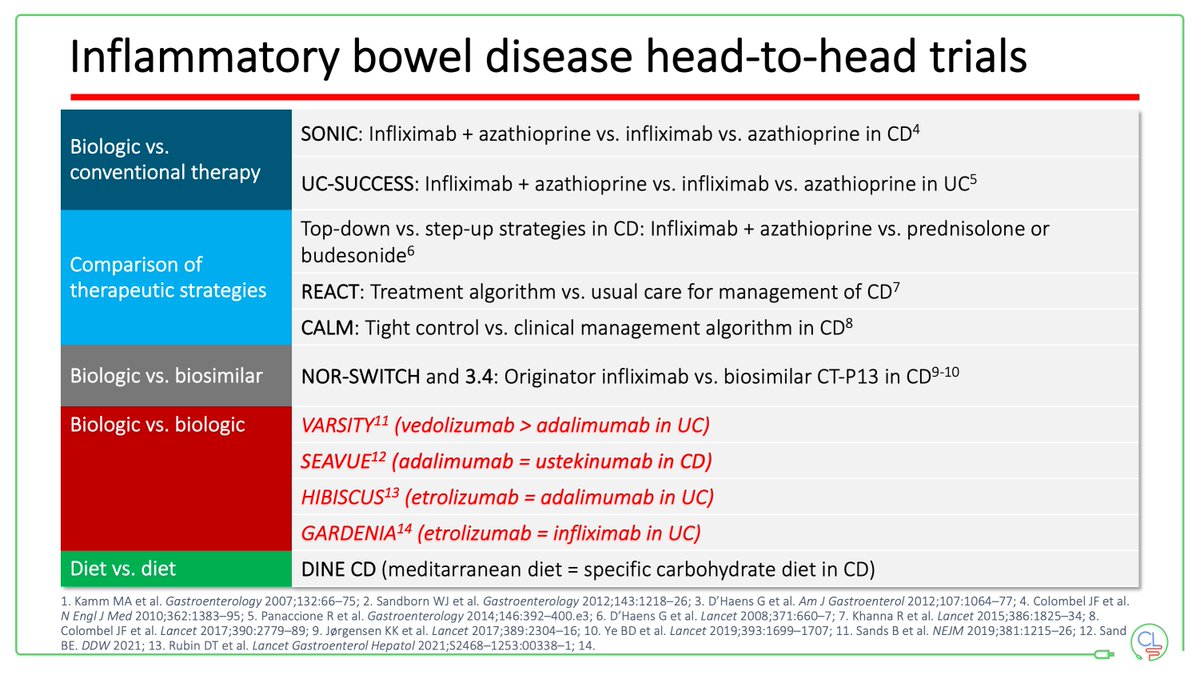
@drlauriekeefer @DrAilsaHart @AGA_Gastro Meantime head-to-head studies are helping with drug positioning
What would you rather see more of in future?
• placebo controlled trials of new drugs
• head-to-head studies of current therapies
• studies where combinations of therapies are tested?
What would you rather see more of in future?
• placebo controlled trials of new drugs
• head-to-head studies of current therapies
• studies where combinations of therapies are tested?
@drlauriekeefer @DrAilsaHart @AGA_Gastro Things I am looking forward to on the near horizon for IBD
• new molecules
• combinations of drugs
• AI applied to colonoscopy & histology
• therapies targeting the gut microbiome
• a deeper understanding of the cause of IBD
Then we move together towards prevention & cure
• new molecules
• combinations of drugs
• AI applied to colonoscopy & histology
• therapies targeting the gut microbiome
• a deeper understanding of the cause of IBD
Then we move together towards prevention & cure

جاري تحميل الاقتراحات...