

✨ Approach to Infiltrative Diseases! ✨
This framework was inspired by @Gurpreet2015's recent Clinical Problem Solving Grand Rounds for @UCSFDOM. Many teaching points on this DDx also passed down by the @CPSolvers.
First, what are the Infiltrative Diseases?
This framework was inspired by @Gurpreet2015's recent Clinical Problem Solving Grand Rounds for @UCSFDOM. Many teaching points on this DDx also passed down by the @CPSolvers.
First, what are the Infiltrative Diseases?

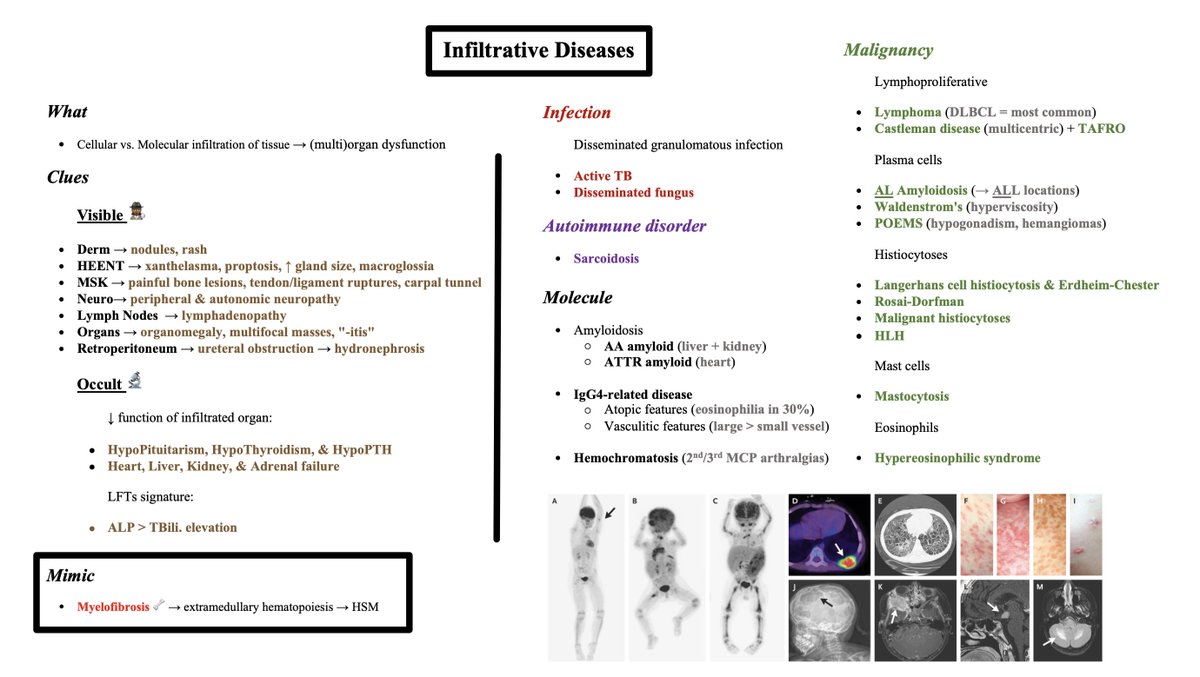
On a quick search, I couldn't find a universal, clear-cut definition for the Infiltrative Diseases, but these diseases all have something in common:
Cellular vs. Molecular infiltration of tissue
👇
(Multi)organ dysfunction
Cellular vs. Molecular infiltration of tissue
👇
(Multi)organ dysfunction
Various clues may prompt suspicion for Infiltrative Disease, as some etiologies have a specific organ predilection, while others have more widespread, multi-organ involvement.
🔑 Key to this schema is reading about each disease & taking note of "favorite" sites of involvement.
🔑 Key to this schema is reading about each disease & taking note of "favorite" sites of involvement.
Disease-specific organ predilection aside, here's a list of "Visible" clues (on exam/imaging) that should raise suspicion for an Infiltrative Disease (list organized by system):
✋Nodules, rash
🗣️Xanthelasma, proptosis, increased gland size (eg parotid swelling), macroglossia
✋Nodules, rash
🗣️Xanthelasma, proptosis, increased gland size (eg parotid swelling), macroglossia
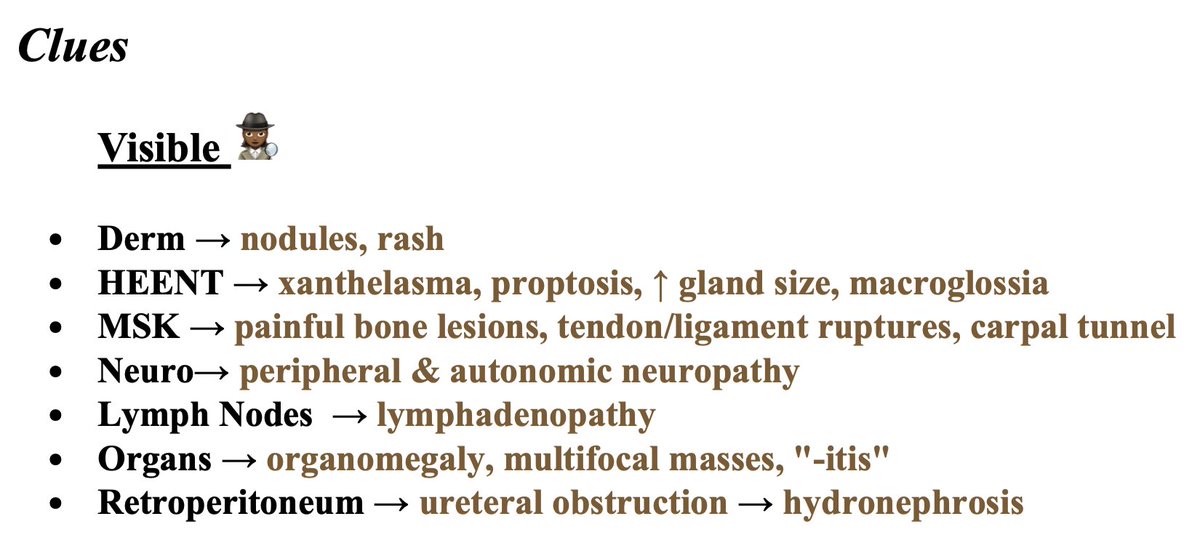
🦴Painful bone lesions, tendon/ligament ruptures, carpal tunnel syndrome
🧠Peripheral & autonomic neuropathy
🟢Lymphadenopathy
❤️Organomegaly, multifocal masses, "-itis" (eg colitis)
⚪Ureteral obstruction (retroperitoneal fibrosis/infiltration) leading to hydronephrosis
🧠Peripheral & autonomic neuropathy
🟢Lymphadenopathy
❤️Organomegaly, multifocal masses, "-itis" (eg colitis)
⚪Ureteral obstruction (retroperitoneal fibrosis/infiltration) leading to hydronephrosis
Suspicion may also be raised by more "Occult" clues (on labs/syndrome assessment).
🕵️♀️ "Occult" clues are due to decreased function of infiltrated organ:
- HypoPit, Hypothyroid, HypoParathyroid
- Heart, Liver, Kidney, & Adrenal failure
🕵️♀️ "Occult" clues are due to decreased function of infiltrated organ:
- HypoPit, Hypothyroid, HypoParathyroid
- Heart, Liver, Kidney, & Adrenal failure
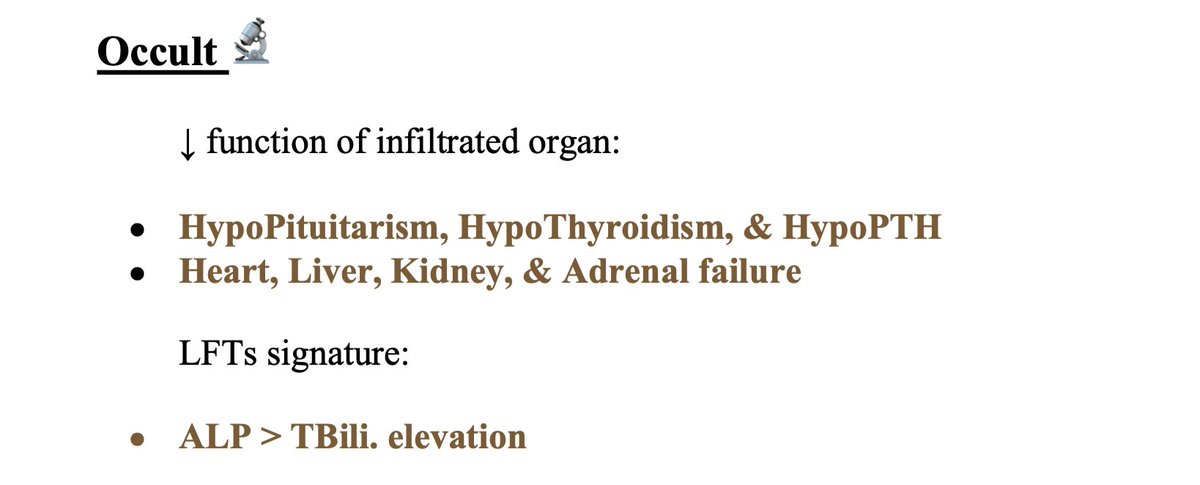
📗Note 1: liver involvement usually leaves a signature in the LFTs as AlkPhos > TBili. elevation.
📗Note 2: if pancytopenia + hepatosplenomegaly (HSM) w/o imaging signs of infiltration, consider myelofibrosis as a mimic. HSM is due to compensatory extramedullary hematopoiesis.
📗Note 2: if pancytopenia + hepatosplenomegaly (HSM) w/o imaging signs of infiltration, consider myelofibrosis as a mimic. HSM is due to compensatory extramedullary hematopoiesis.

Now that we've covered clues that point toward Infiltrative Diseases, let's go through some etiologies within each diagnostic bucket:
❓Infection
❓Malignancy
❓Autoimmune disorder
❓Molecule
Remember: 🔑 to this schema is developing illness scripts for each etiology
❓Infection
❓Malignancy
❓Autoimmune disorder
❓Molecule
Remember: 🔑 to this schema is developing illness scripts for each etiology
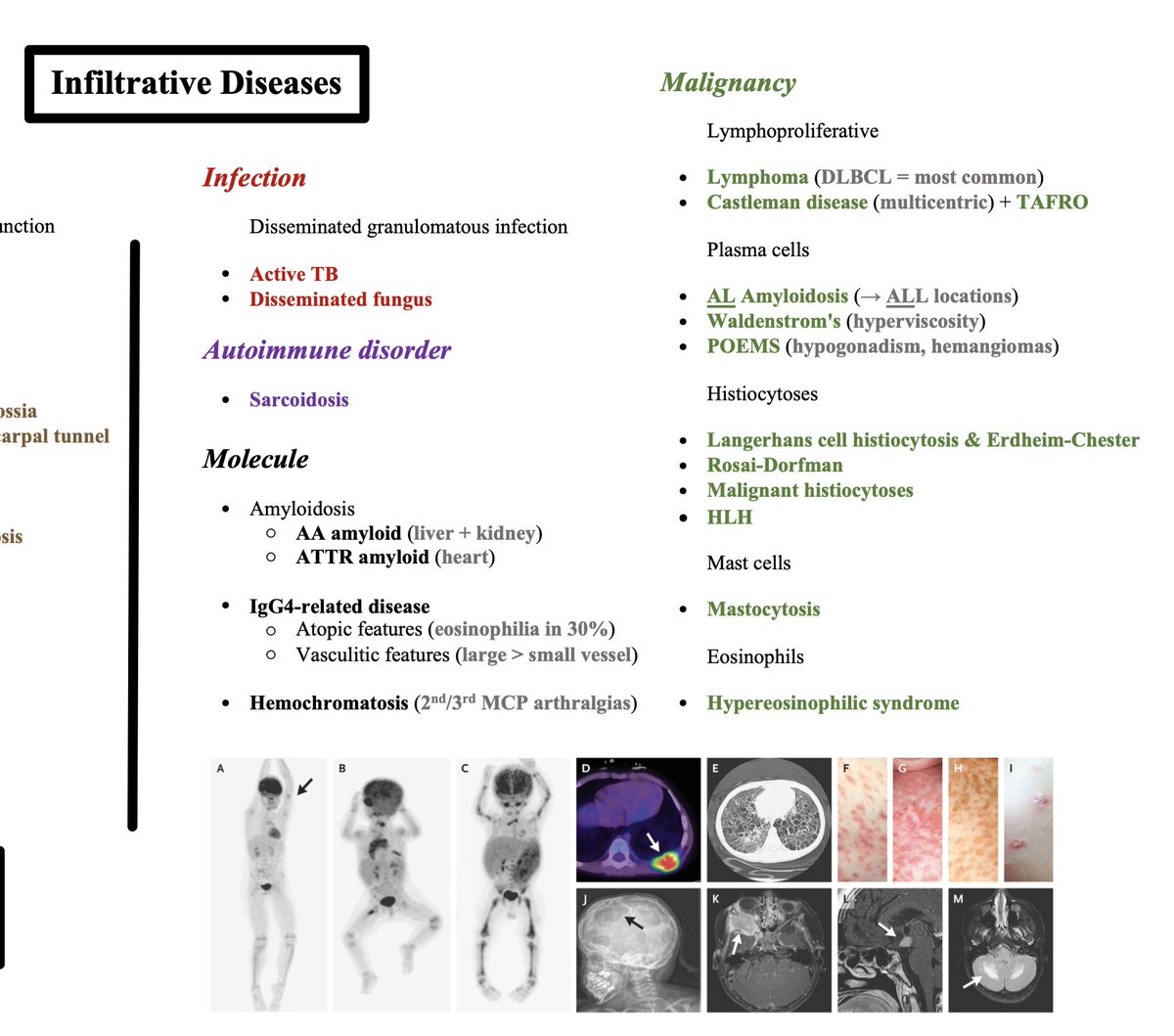
🦠 Infections
While additional infectious diseases may join this list, the most common offenders are disseminated granulomatous infections, namely:
- Active TB
- Disseminated fungus
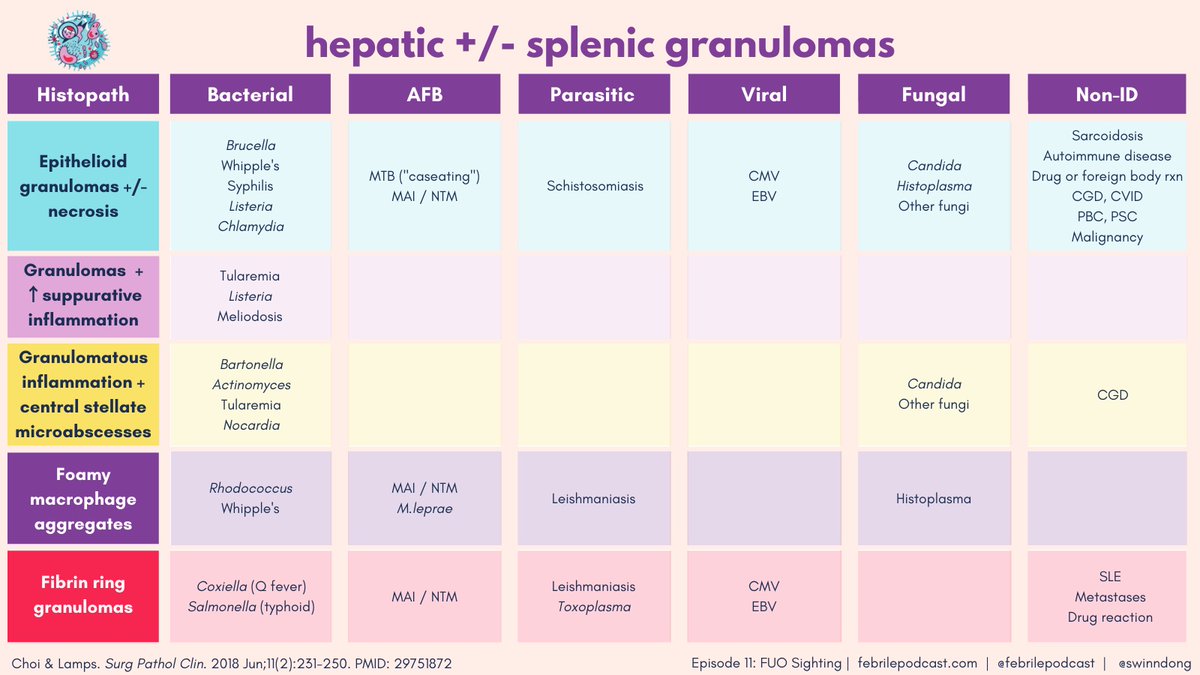
📚 If hepatosplenic granulomas, consider broader DDx as below
📚 Graphic by @febrilepodcast
While additional infectious diseases may join this list, the most common offenders are disseminated granulomatous infections, namely:
- Active TB
- Disseminated fungus
📚 If hepatosplenic granulomas, consider broader DDx as below
📚 Graphic by @febrilepodcast
✨ Autoimmune disorders
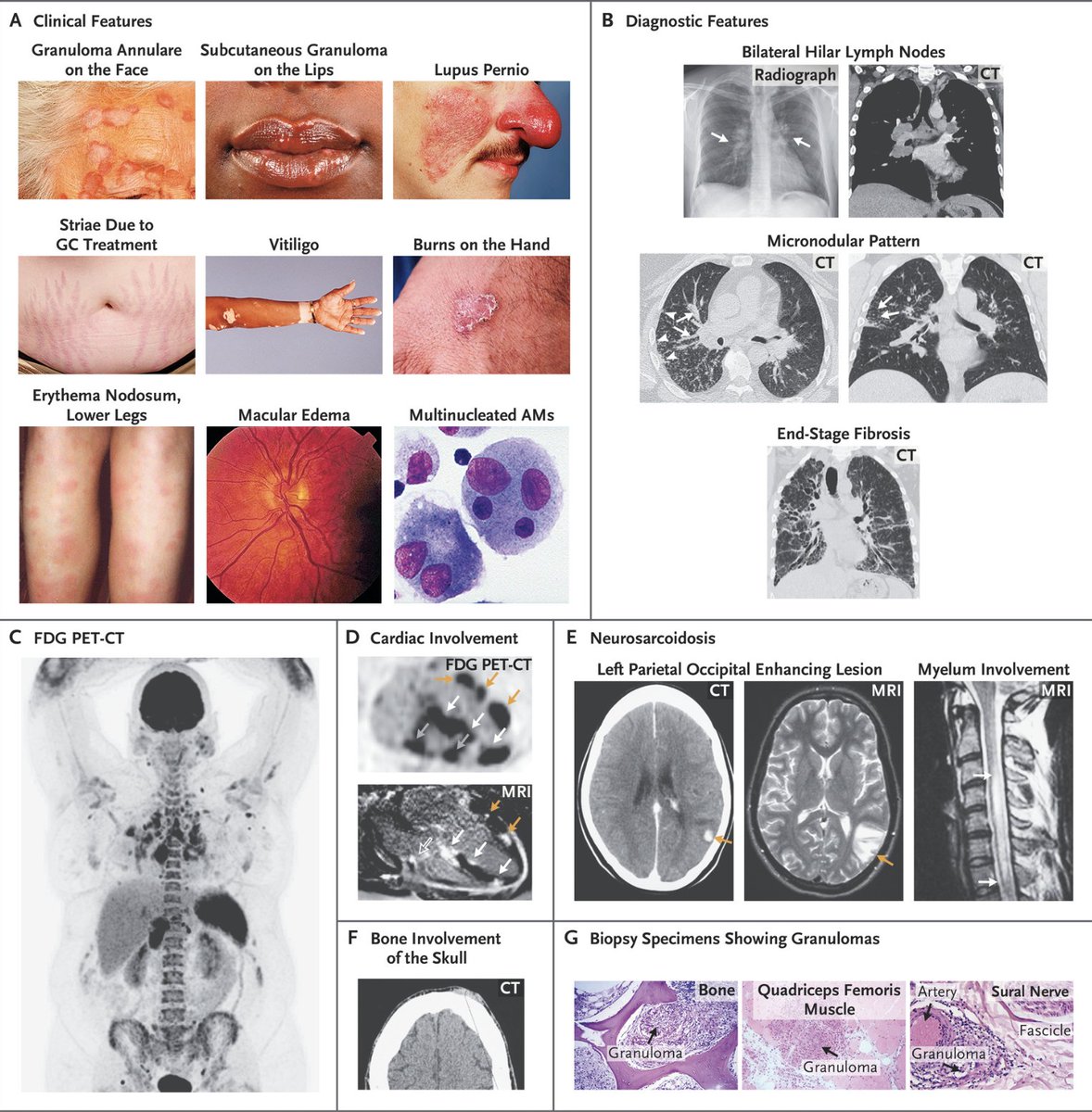
- Sarcoidosis
Common features:
🟣Hilar LAD, pulm infiltrates, pulm fibrosis
🟣Lofgren's syndrome (hilar LAD + E. nodosum + polyarticular arthritis)
🟣CN palsies, uveitis
Ref: nejm.org
- Sarcoidosis
Common features:
🟣Hilar LAD, pulm infiltrates, pulm fibrosis
🟣Lofgren's syndrome (hilar LAD + E. nodosum + polyarticular arthritis)
🟣CN palsies, uveitis
Ref: nejm.org

⚙️ Molecule deposition
- Amyloidosis (AA = liver & kidney predilection; ATTR = heart predilection)
- IgG4-related disease (notable atopic features & vasculitic features, large > small vessel)
- Hemochromatosis (2nd/3rd MCP arthralgia somewhat unique)
- Amyloidosis (AA = liver & kidney predilection; ATTR = heart predilection)
- IgG4-related disease (notable atopic features & vasculitic features, large > small vessel)
- Hemochromatosis (2nd/3rd MCP arthralgia somewhat unique)
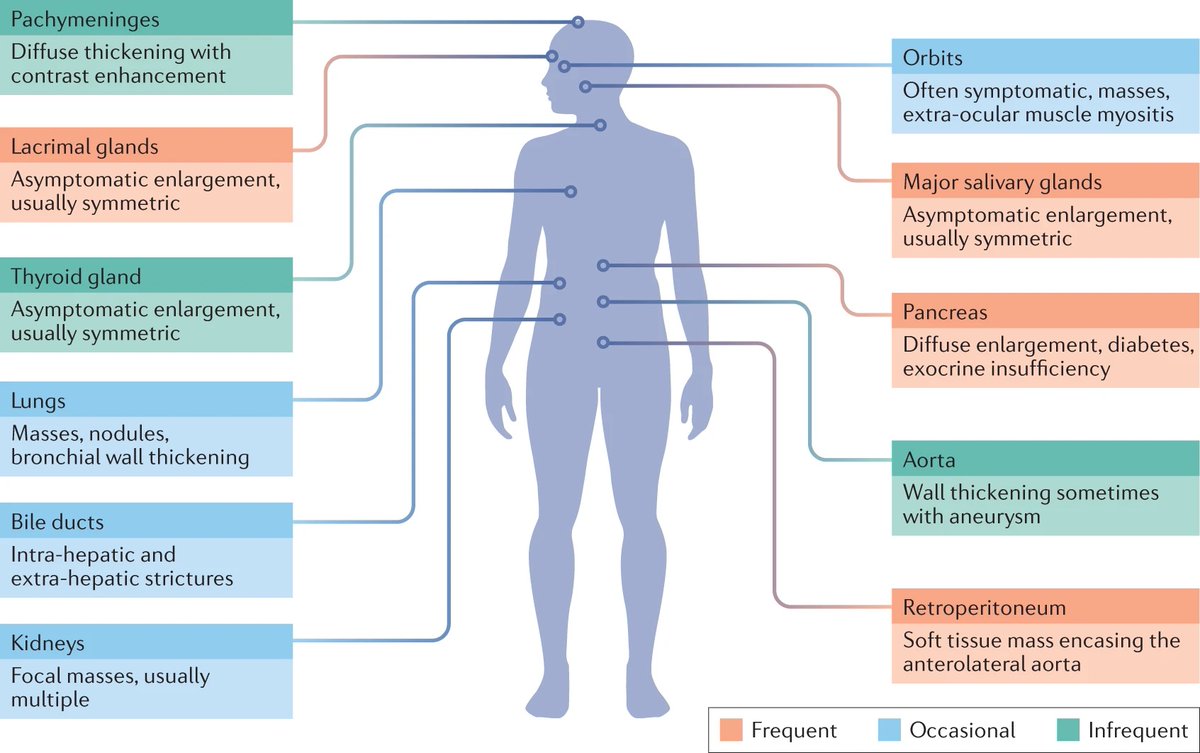
⚙️ More on IgG4-related disease:
▪️ Onset: 50-70s
▪️ Insidious, progressive, fibroinflammatory tumor-like lesions
▪️ Fever uncommon (High ESR + Normal CRP)
▪️ IgG4 >135 mg/dL (75-90%); IgE >1000 mg/dL (60%)
▪️ Tissue affinity: lacrimal/salivary glands, pancreas, retroperitoneum
▪️ Onset: 50-70s
▪️ Insidious, progressive, fibroinflammatory tumor-like lesions
▪️ Fever uncommon (High ESR + Normal CRP)
▪️ IgG4 >135 mg/dL (75-90%); IgE >1000 mg/dL (60%)
▪️ Tissue affinity: lacrimal/salivary glands, pancreas, retroperitoneum
🩸 Malignancies
Here is where the DDx can get quite long, but malignancies can be broken down by origin of abnormality:
- Lymphoproliferative
- Plasma cells
- Histiocytoses
- Mast cells
- Eosinophils
Here is where the DDx can get quite long, but malignancies can be broken down by origin of abnormality:
- Lymphoproliferative
- Plasma cells
- Histiocytoses
- Mast cells
- Eosinophils
🩸 Lymphoproliferative:
- Lymphoma (DLBCL = most common)
- Castleman disease (multicentric) + TAFRO
- Lymphoma (DLBCL = most common)
- Castleman disease (multicentric) + TAFRO
🩸 More on Castleman disease & TAFRO:
🟩 Castleman (multicentric): fever + diffuse LAD + HSM + cytopenias + organ dysfunction 👉 plasmablastic findings on LN biopsy
🟩 TAFRO (variant): Thrombocytopenia + Anasarca + myeloFibrosis + Renal dysfunction + Organomegaly
🟩 Castleman (multicentric): fever + diffuse LAD + HSM + cytopenias + organ dysfunction 👉 plasmablastic findings on LN biopsy
🟩 TAFRO (variant): Thrombocytopenia + Anasarca + myeloFibrosis + Renal dysfunction + Organomegaly
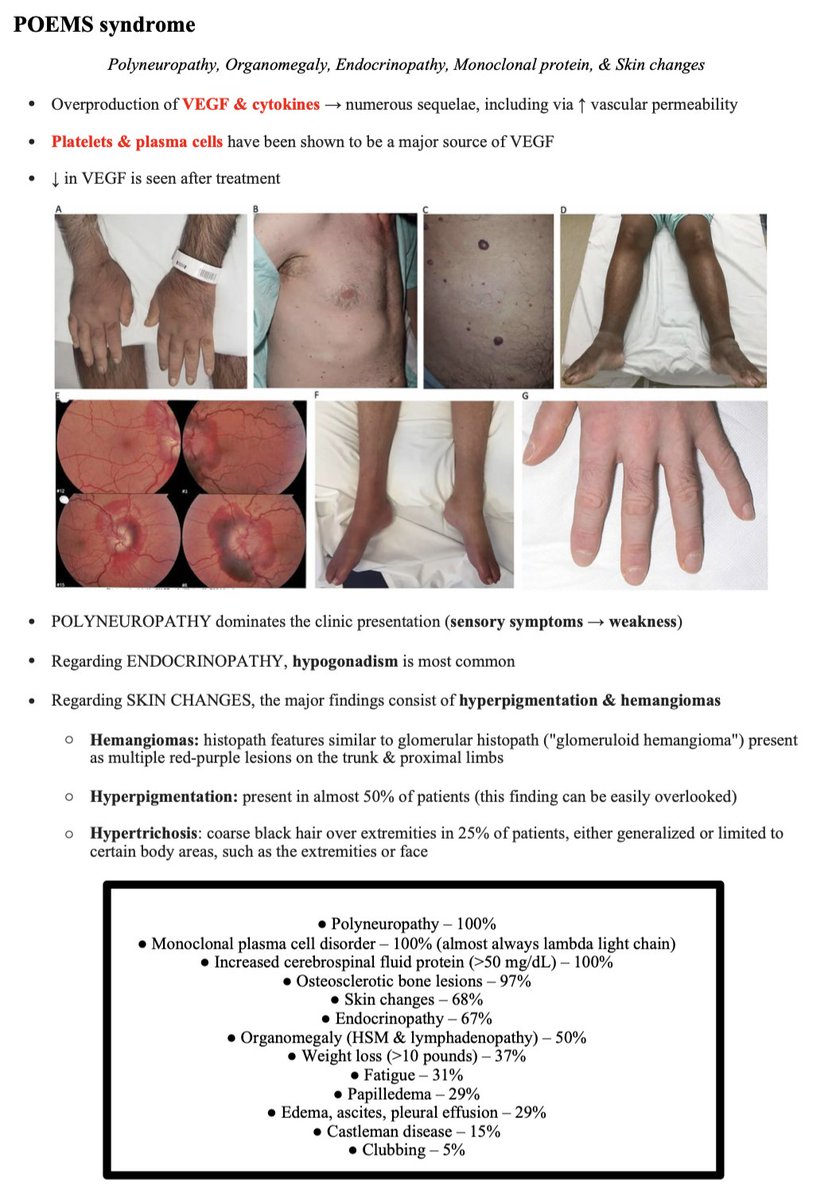
🩸 Plasma cells
- AL amyloid (can deposit in ALL locations)
- Waldenstrom's (think hyperviscosity)
- POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, skin changes)
📚 More on POEMS attached:
- AL amyloid (can deposit in ALL locations)
- Waldenstrom's (think hyperviscosity)
- POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, skin changes)
📚 More on POEMS attached:
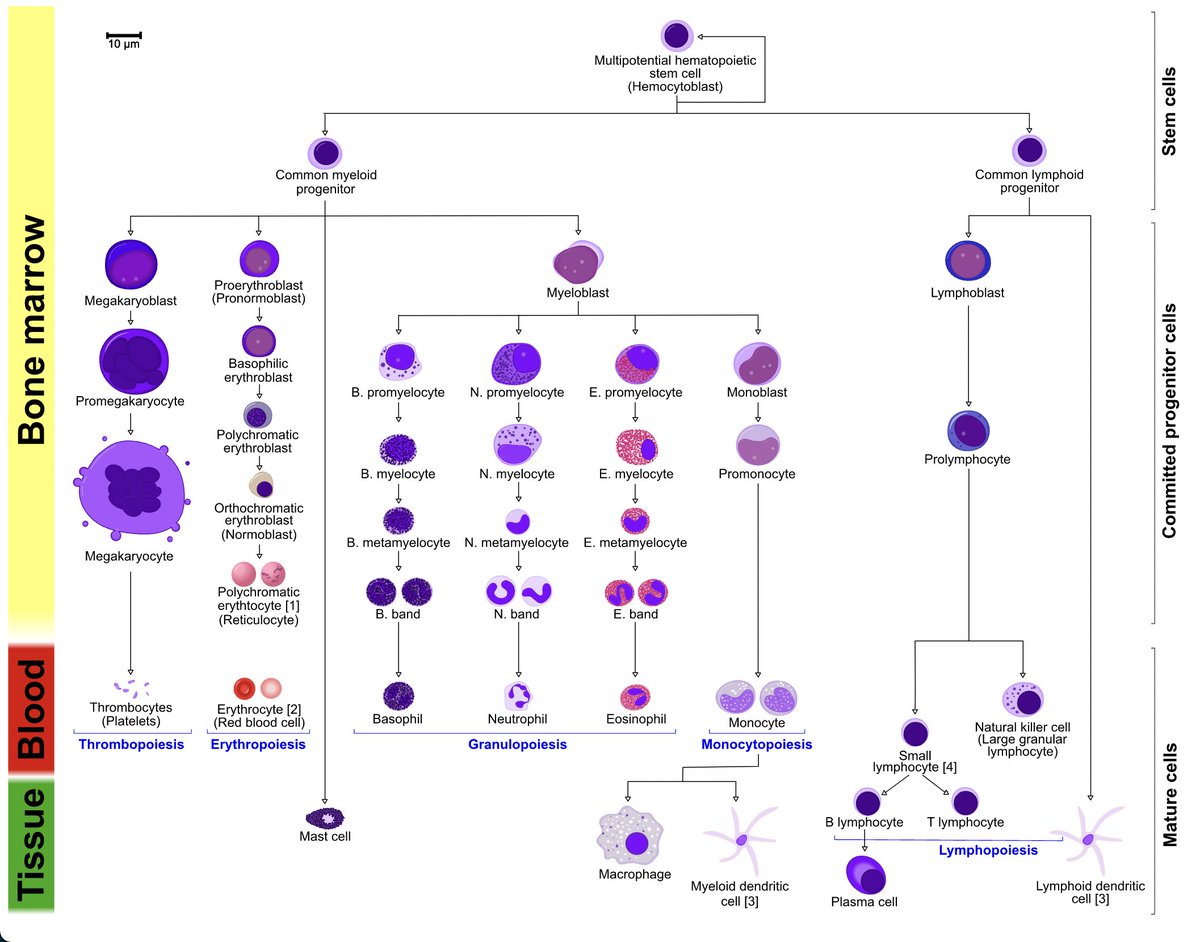
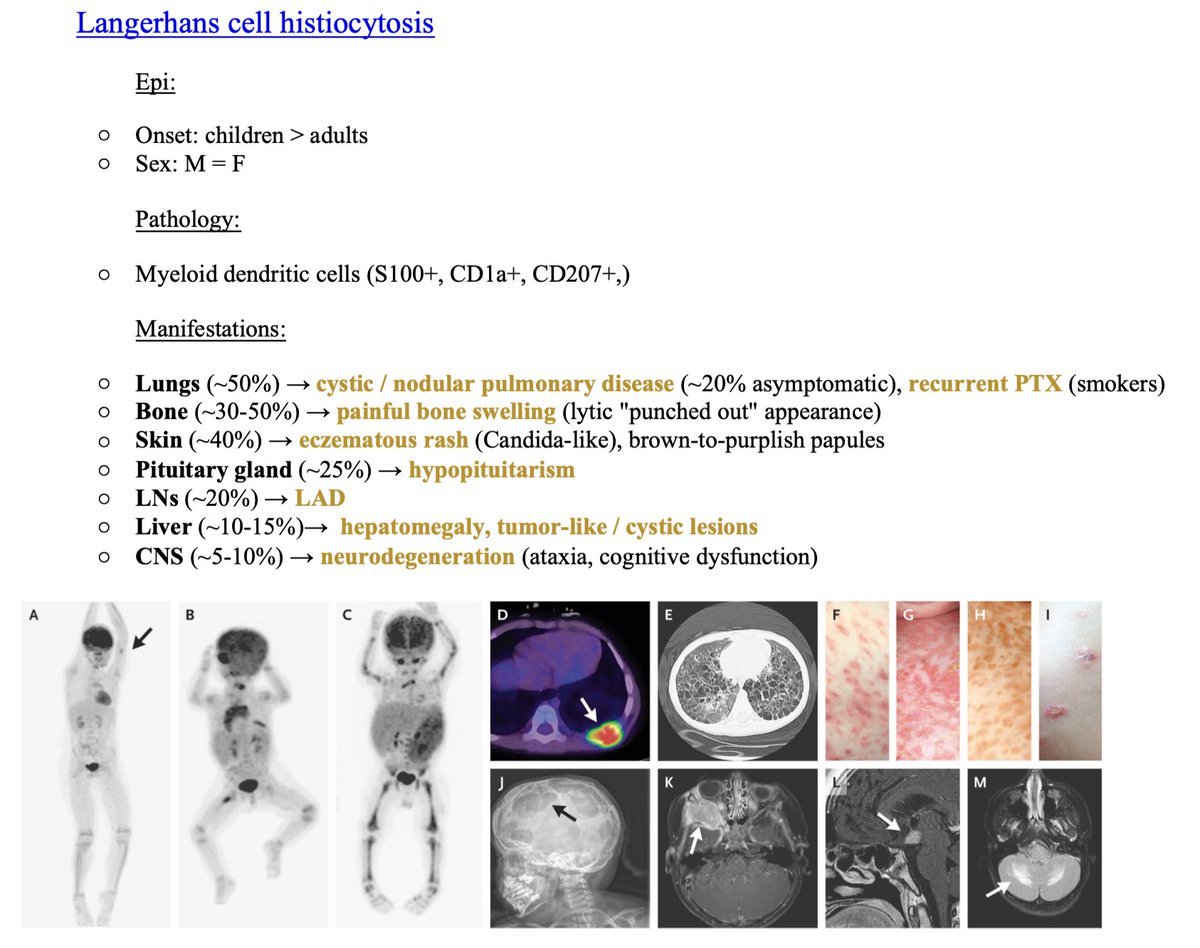
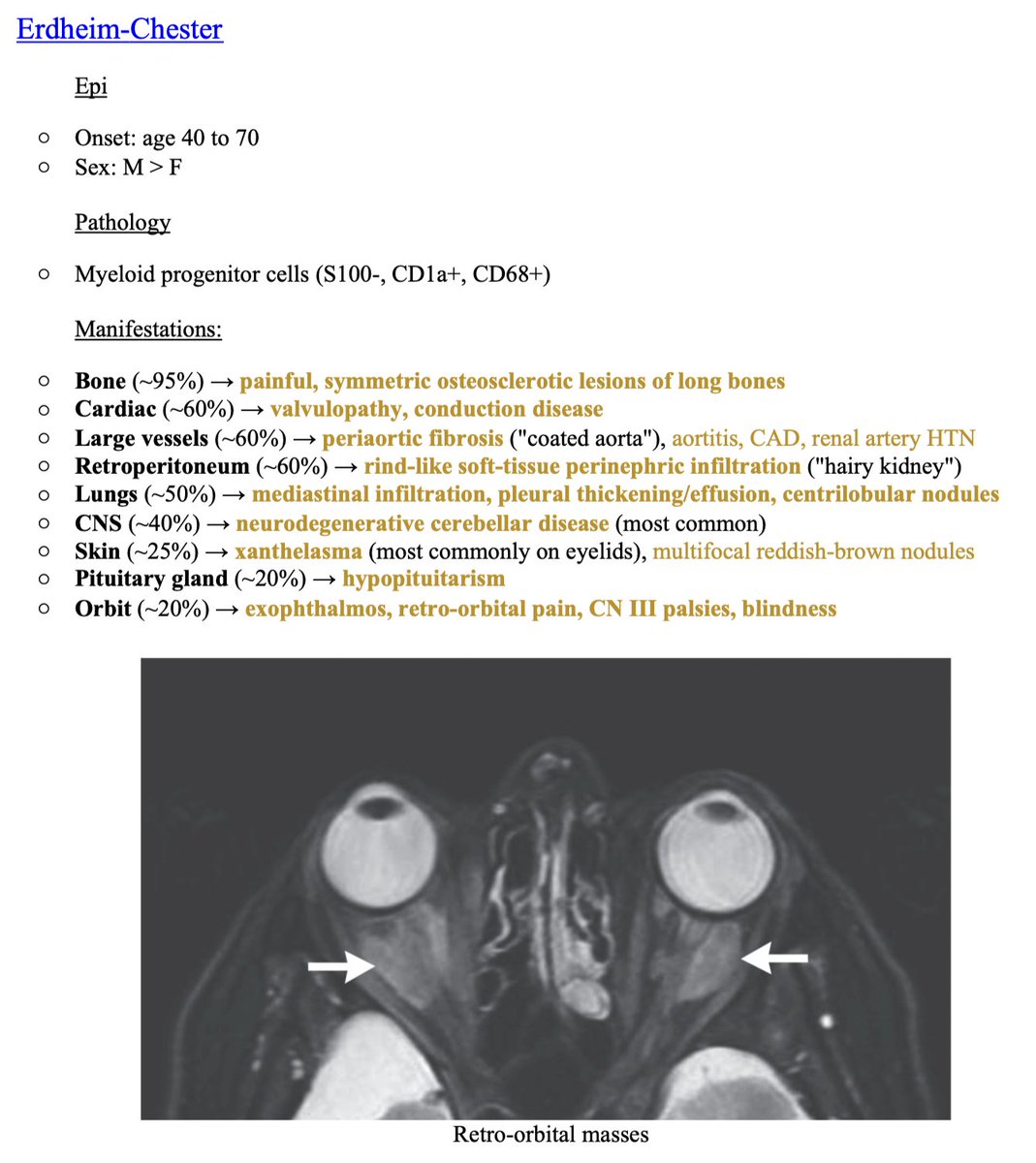
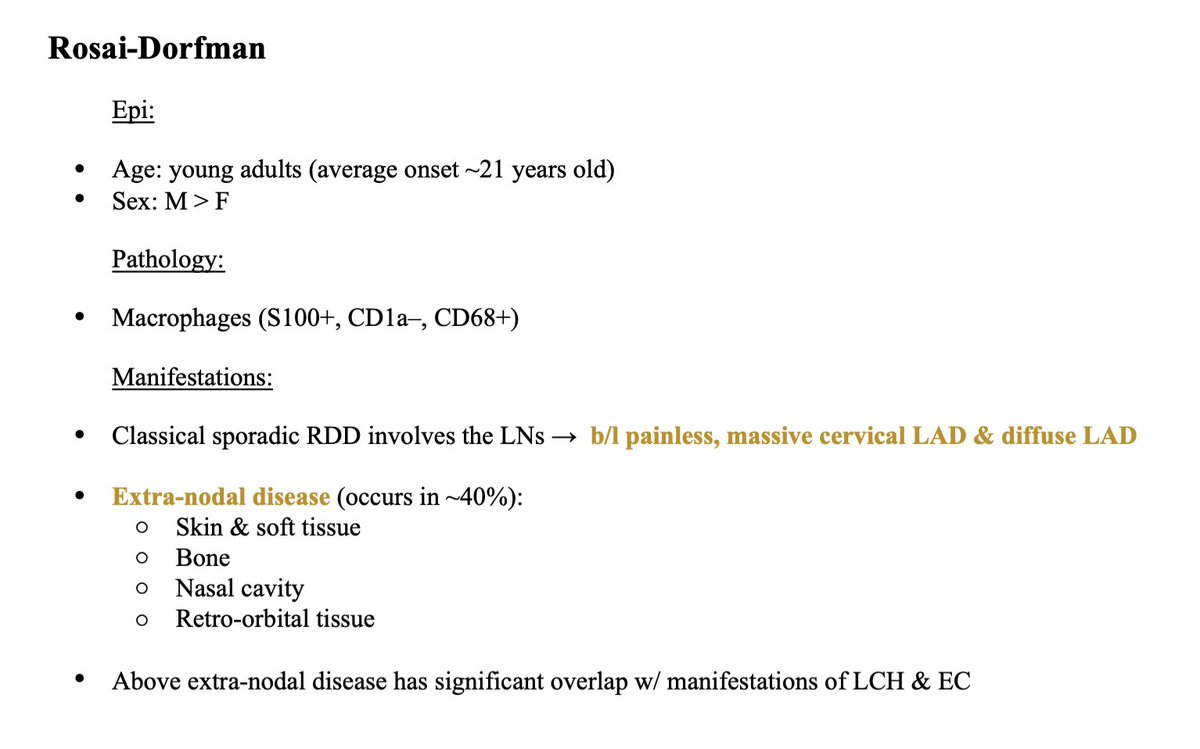
🩸 Histiocytoses
This is a group of disorders of macrophages/monocytes & dendritic cells that infiltrate tissues:
- Langerhans cell histiocytosis & Erdheim-Chester
- Rosai-Dorfman
- Malignant histiocytoses
- HLH
This is a group of disorders of macrophages/monocytes & dendritic cells that infiltrate tissues:
- Langerhans cell histiocytosis & Erdheim-Chester
- Rosai-Dorfman
- Malignant histiocytoses
- HLH
🩸 More on Langerhans cell histiocytosis (LCH), Erdheim-Chester (EC), & Rosai-Dorfman (RD):
▪️ LCH & EC are grouped because nearly 20% of EC patients also have LCH lesions
▪️ Illness scripts for these 3 histiocytoses are attached:
▪️ LCH & EC are grouped because nearly 20% of EC patients also have LCH lesions
▪️ Illness scripts for these 3 histiocytoses are attached:
🩸 Mast cells
- Mastocytosis
Presents as:
🔹Urticarial rash vs. Episodic symptoms of mast cell activation (eg hTN, flushing) w/o a rash
🔹Cytopenias (marrow infiltration) +/- additional MPN
🔹HSM
- Mastocytosis
Presents as:
🔹Urticarial rash vs. Episodic symptoms of mast cell activation (eg hTN, flushing) w/o a rash
🔹Cytopenias (marrow infiltration) +/- additional MPN
🔹HSM
🩸 Eosinophils
- Hypereosinophilic syndrome
Defined as:
🔸 Hypereosinophilia + cell-mediated organ damage
Common findings:
🔸 Rash, myocarditis, pulm fibrosis, gastritis/enteritis/colitis, thrombosis, peripheral neuropathy
@Anand_88_Patel:
- Hypereosinophilic syndrome
Defined as:
🔸 Hypereosinophilia + cell-mediated organ damage
Common findings:
🔸 Rash, myocarditis, pulm fibrosis, gastritis/enteritis/colitis, thrombosis, peripheral neuropathy
@Anand_88_Patel:
🏁 That's it for my whirlwind tour of some major Infiltrative Diseases!
- Summary:
🏁 Suspicion for Infiltrative Disease may be prompted by "Visible" clues (on exam/imaging) or "Occult" clues (on labs/syndrome assessment)
🏁 Organ predilection varies by disease type
- Summary:
🏁 Suspicion for Infiltrative Disease may be prompted by "Visible" clues (on exam/imaging) or "Occult" clues (on labs/syndrome assessment)
🏁 Organ predilection varies by disease type
Acknowledgments:
@KirtanPatolia, thanks for the encouragement & helpful comments! Several pearls not possible w/o you.
@rabihmgeha, for introducing me to a basic approach to the Infiltrative Diseases via the podcast!
@KirtanPatolia, thanks for the encouragement & helpful comments! Several pearls not possible w/o you.
@rabihmgeha, for introducing me to a basic approach to the Infiltrative Diseases via the podcast!
References:
1) ncbi.nlm.nih.gov
2) ashpublications.org
3) casereports.bmj.com
4) nejm.org
5) #H801363" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com #H801363" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com
6) nejm.org
7) #H2020280863" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com #H2020280863" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com
8) uptodate.com
1) ncbi.nlm.nih.gov
2) ashpublications.org
3) casereports.bmj.com
4) nejm.org
5) #H801363" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com #H801363" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com
6) nejm.org
7) #H2020280863" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com #H2020280863" target="_blank" rel="noopener" onclick="event.stopPropagation()">uptodate.com
8) uptodate.com
ncbi.nlm.nih.gov/pmc/articles/P…
casereports.bmj.com/content/2014/b…
uptodate.com/contents/erdhe…
nejm.org/doi/full/10.10…

ashpublications.org/blood/article/…
Revised classification of histiocytoses and neoplasms of the macrophage-dendritic cell lineages
Abstract. The histiocytoses are rare disorders characterized by the accumulation of macrophage, dend...
uptodate.com/contents/clini…
nejm.org/doi/full/10.10…
IgG4-Related Disease | NEJM
Review Article from The New England Journal of Medicine — IgG4-Related Disease
uptodate.com/contents/poems…
جاري تحميل الاقتراحات...