

Hi #MedTwitter #MedStudentTwitter #neurotwitter #MedEd #FOAMed! It's been too long since my last #EndNeurophobia #tweetorial so here's an introduction to brain imaging–thanks @sarrovasta for the request!🧠❤️
cc:@CPSolvers @rabihmgeha @DxRxEdu @AvrahamCooperMD @caseyalbin
1/🧵
cc:@CPSolvers @rabihmgeha @DxRxEdu @AvrahamCooperMD @caseyalbin
1/🧵
Let's start w/CT. I'll focus on brain (and not bone or soft tissue). First:
* Identify normal structures and any abnormalities in:
- Size
- Shape
- Symmetry
(note *symmetric* abnormalities such as ventriculomegaly or diffuse cerebral edema may not be obvious w/o experience)
2/
* Identify normal structures and any abnormalities in:
- Size
- Shape
- Symmetry
(note *symmetric* abnormalities such as ventriculomegaly or diffuse cerebral edema may not be obvious w/o experience)
2/
Next:
* Identify abnormalities
- Hypodensity
- Hyperdensity
Broadly:
• Hypodensity:
- Ischemia
- Inflammation
- Infection
- Neoplasm
• Hyperdensity:
- Blood
- Calcification
- Hyperdense tumors (e.g. lymphoma)
- Thrombus in vessel
- Contrast enhancement
3/
* Identify abnormalities
- Hypodensity
- Hyperdensity
Broadly:
• Hypodensity:
- Ischemia
- Inflammation
- Infection
- Neoplasm
• Hyperdensity:
- Blood
- Calcification
- Hyperdense tumors (e.g. lymphoma)
- Thrombus in vessel
- Contrast enhancement
3/
Hypodensities= BROAD DDx. Distinguishing infl v infxn v neoplasm requires clinical context & more imaging.
Distinguishing stroke v the rest: if hypodensity respects gray-white junction= likely NOT stroke. Stroke close to cortical surface =affects both gray & white matter...
4/
Distinguishing stroke v the rest: if hypodensity respects gray-white junction= likely NOT stroke. Stroke close to cortical surface =affects both gray & white matter...
4/
Which one is the stroke?
Clinical context would help but, radiologically...
5/
Clinical context would help but, radiologically...
5/

⬆️The left one = hypodensity NOT respecting gray-white junction= ischemic stroke
The right one = respects G-W junction = tumor v infection v inflammation (in this case was toxo but no way to tell from non-con CT alone (let alone no clinical context)
6/
The right one = respects G-W junction = tumor v infection v inflammation (in this case was toxo but no way to tell from non-con CT alone (let alone no clinical context)
6/
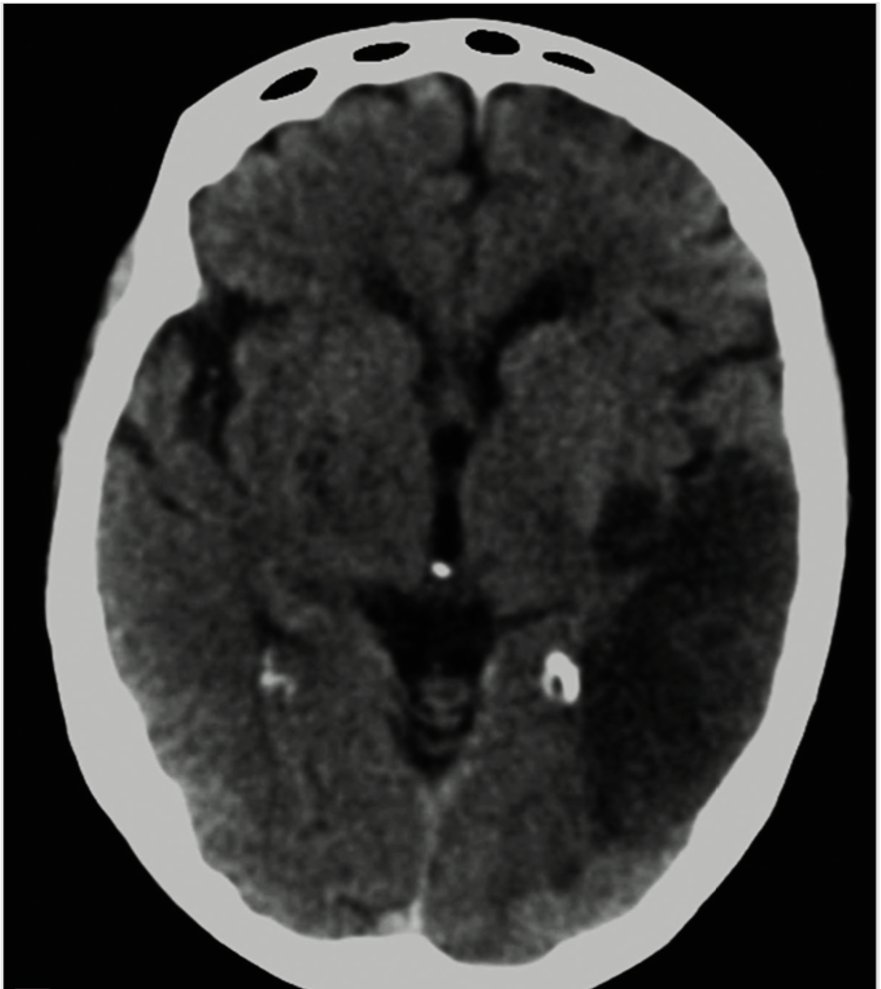
Hyperdensities: blood v calcification v hypercellular mass v IV contrast. Clinical context usually makes distinction obvious. When in doubt, Hounsfield units can distinguish
Here's an intracerebral hemorrhage (left) and neurocysticercosis (right)
7/
Here's an intracerebral hemorrhage (left) and neurocysticercosis (right)
7/


Now on to MRI. Here was also look for size/shape/symmetry of normal structures and abnormalities of these or presence of hypointensity or hyperintensity.
But the significance of hypo v hyper depends on the sequence....
8/
But the significance of hypo v hyper depends on the sequence....
8/
T1: Gray matter dark, white matter brighter
T2: Gray matter bright, white matter dark (like a photographic ‘negative’ of T1)
9/
T2: Gray matter bright, white matter dark (like a photographic ‘negative’ of T1)
9/


FLAIR: T2 with CSF signal subtracted (makes it easier to see periventricular white matter lesions).
T2 on L, FLAIR on R. Can you see the lesion adjacent to the frontal horn of the right lateral ventricle on the T2? Nope! That's how FLAIR helps!
10/
T2 on L, FLAIR on R. Can you see the lesion adjacent to the frontal horn of the right lateral ventricle on the T2? Nope! That's how FLAIR helps!
10/


Blood has different signal characteristics on T1 v T2 depending on age. See this table.
Mnemonic (I = iso, B= bright, D= dark)
IB
ID
BD
BB
DD
11/
Mnemonic (I = iso, B= bright, D= dark)
IB
ID
BD
BB
DD
11/

DWI/ADC: looks for decreased diffusion of water molecules through tissue (bright on DWI/dark on ADC):
- cytotoxic edema (acute ischemic stroke, ongoing seizure activity)
- tightly packed cells (abscess, lymphoma)
- in cortical ribbon and basal ganglia in CJD
Here: MCA stroke
12/
- cytotoxic edema (acute ischemic stroke, ongoing seizure activity)
- tightly packed cells (abscess, lymphoma)
- in cortical ribbon and basal ganglia in CJD
Here: MCA stroke
12/

GRE/SWI: blood and calcium are dark
Here: multiple microhemorrhages in a patient with cerebral amyloid angiopathy (see and by @a_charidimou )
13/
Here: multiple microhemorrhages in a patient with cerebral amyloid angiopathy (see and by @a_charidimou )
13/

So where to start?
1. As w/CT, look at size/shape/symmetry of structures (often done on T1)
2. FLAIR: look for hyperintensities=pathology
3. T1 pre vs post: look for whether lesions enhance (= blood brain barrier breakdown: inflammation/tumor/infection/subacute stroke)
14/
1. As w/CT, look at size/shape/symmetry of structures (often done on T1)
2. FLAIR: look for hyperintensities=pathology
3. T1 pre vs post: look for whether lesions enhance (= blood brain barrier breakdown: inflammation/tumor/infection/subacute stroke)
14/
4. DWI/ADC: look for hyperintense DWI with corresponding hypointense ADC (and remember not all that restricts is stroke; see above)
5. GRE/SWI: look for hypointensities (blood or calcium)
15/
5. GRE/SWI: look for hypointensities (blood or calcium)
15/
Still don't know the answer with the history, exam, labs and MRI....? Depending on context....
- Consider more imaging (MR Spectroscopy, PET, MR/CT perfusion)
- Consider CSF analysis
- Consider brain biopsy
16/
- Consider more imaging (MR Spectroscopy, PET, MR/CT perfusion)
- Consider CSF analysis
- Consider brain biopsy
16/
What's your approach to brain imaging 101?
@caseyalbin @NMatch2022 @a_charidimou @tabby_kennedy @WendeNGibbs @theneuroradguy @learnneurorad @RyanBPetersonMD @gabifpucci @MariaMjaleman @valeroldan23 @doug_pet @harvardneuromds @Tracey1milligan @WmOBrienDO @JudyGadde @TheASNR
17/
@caseyalbin @NMatch2022 @a_charidimou @tabby_kennedy @WendeNGibbs @theneuroradguy @learnneurorad @RyanBPetersonMD @gabifpucci @MariaMjaleman @valeroldan23 @doug_pet @harvardneuromds @Tracey1milligan @WmOBrienDO @JudyGadde @TheASNR
17/
Want tons of CT and MRI examples of classic and rare diseases? Look up my book on AccessMedicine through your school's digital library for free access!
accessmedicine.mhmedical.com
accessmedicine.mhmedical.com
Loading suggestions...