

Hello people! 🤓
This thread is about
Intrarenal Acute kidney INJURY 🧐
.
This thread is about
Intrarenal Acute kidney INJURY 🧐
.

Quick Recap😁
As you know the kidney functions by removing waste, regulating electrolytes and water levels as well as producing hormones like Erythropoietin🧐
Blood starts from the renal artery👉🏼to the glomeruli where its filtered either reabsorbed or secreted👉🏼finally to urine
As you know the kidney functions by removing waste, regulating electrolytes and water levels as well as producing hormones like Erythropoietin🧐
Blood starts from the renal artery👉🏼to the glomeruli where its filtered either reabsorbed or secreted👉🏼finally to urine
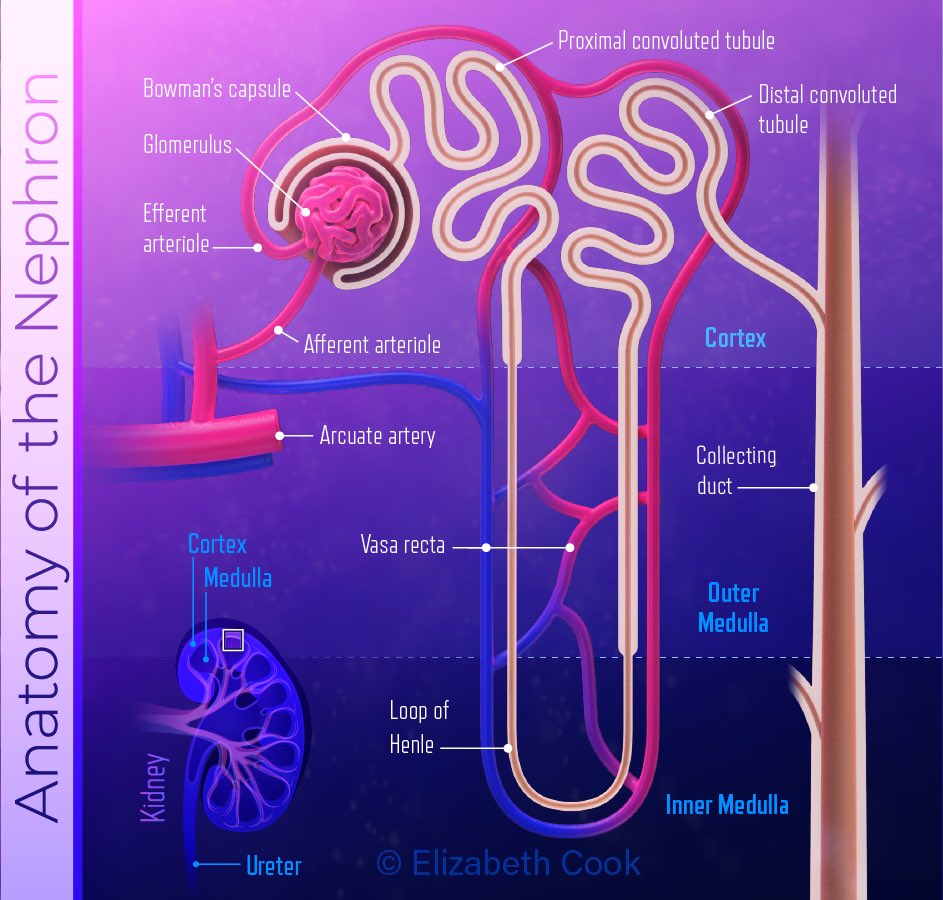
Intrarenal or sometimes called intrinsic acute kidney injury happens when damage to the kidneys tubules like glomerulus, interstitium, causes a sudden loss in kidney function.
The most common cause of Intrarenal Acute Kidney injury is
Acute Tubular Necrosis (ATN)
Which is a condition in where the small filtering tubes in the kidney are injured (epithelial cells die due to ischemia)
Picture’s from: researchgate.net
Acute Tubular Necrosis (ATN)
Which is a condition in where the small filtering tubes in the kidney are injured (epithelial cells die due to ischemia)
Picture’s from: researchgate.net

Since it causes ischemia then it’s a result of decreased blood flow
Decreased blood flow can be a result of:
- severe hypotension (as in hypovolemic patient’s)
- Thromboembolism or cholesterol embolism, etc
Decreased blood flow can be a result of:
- severe hypotension (as in hypovolemic patient’s)
- Thromboembolism or cholesterol embolism, etc
Another cause can be
Nephrotoxins
👉🏼 substances that directly damage the epithelial cells, like:
- Infection ( Sepsis
- Medications (e.g aminoglycosides, amphotericin B)
- Myoglobin from damaged muscles
- Heavy medials
Nephrotoxins
👉🏼 substances that directly damage the epithelial cells, like:
- Infection ( Sepsis
- Medications (e.g aminoglycosides, amphotericin B)
- Myoglobin from damaged muscles
- Heavy medials
What happens?
proximal tubular cells fall into the tubular lumen→debris build up & obstruct tubules→leads to High pressure tubules → blood moves from high p blood vessels to high pressure tubles→ decrease blood filtered→ decreased GFR
Picture from: researchgate.net
proximal tubular cells fall into the tubular lumen→debris build up & obstruct tubules→leads to High pressure tubules → blood moves from high p blood vessels to high pressure tubles→ decrease blood filtered→ decreased GFR
Picture from: researchgate.net
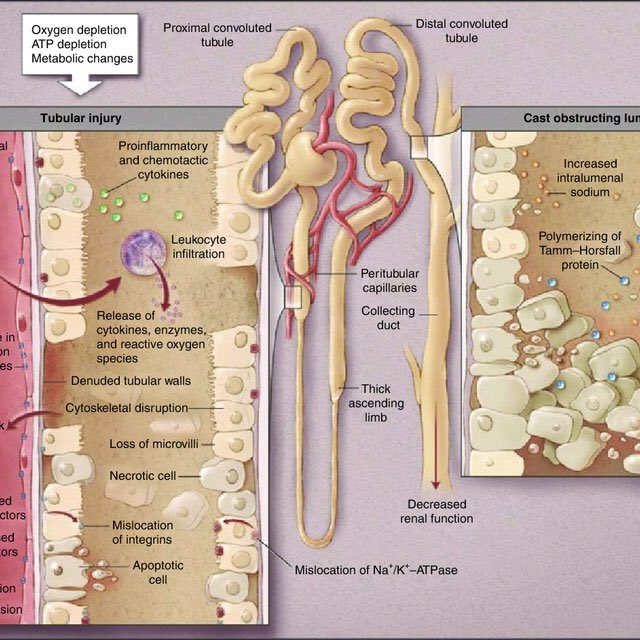
This this will lead to decreased urine output👉🏼Oliguria
Urea and creatinine will not be filtered properly👉🏼increase retention of them in blood👉🏼 azotemia
Since the cells are ischemic can’t filter blood, eventually it’ll lead to Hyperkalemia, metabolic acidosis and uraemia ☹️
Urea and creatinine will not be filtered properly👉🏼increase retention of them in blood👉🏼 azotemia
Since the cells are ischemic can’t filter blood, eventually it’ll lead to Hyperkalemia, metabolic acidosis and uraemia ☹️
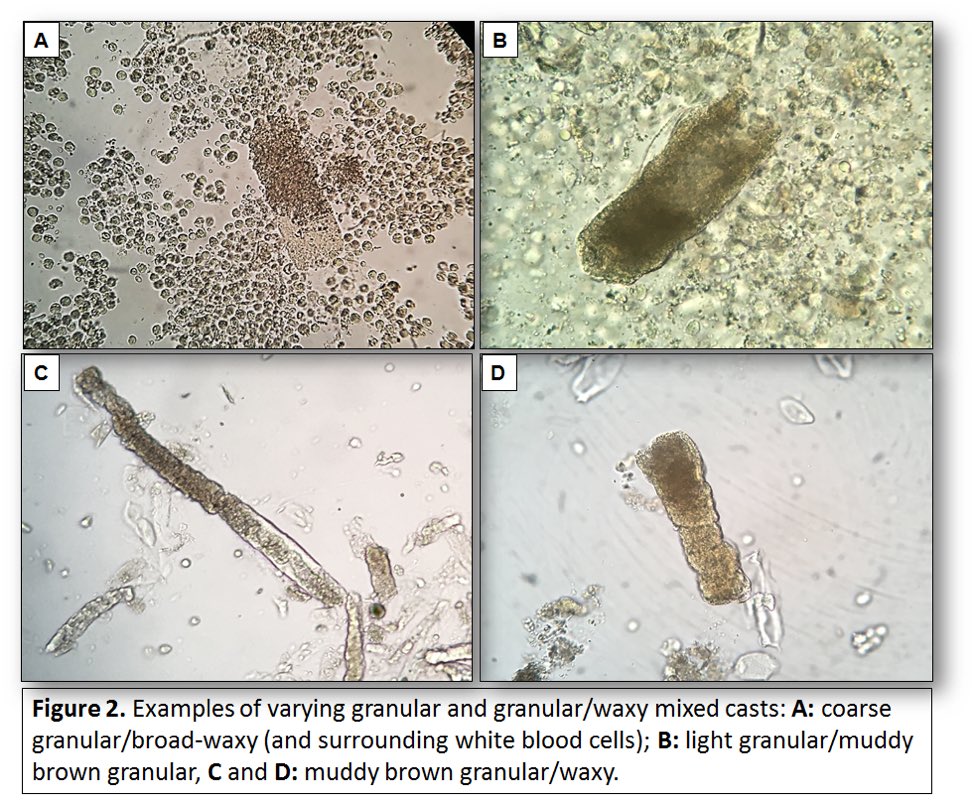
Later on, dead cells that have built in the tubules will form a brown granular caste
This brown cast will be excreted which will cause the diagnostic features of Muddy brown granular cast in urine👇🏼
Picture is from: renalfellow.org
This brown cast will be excreted which will cause the diagnostic features of Muddy brown granular cast in urine👇🏼
Picture is from: renalfellow.org
Upon the cause, the patient is managed
Some patients will experience tubular re-epithelialisation and gain full-recovery when treated adequately 😁👍🏼
Some patients will experience tubular re-epithelialisation and gain full-recovery when treated adequately 😁👍🏼
Another cause of Intrarenal AKI is
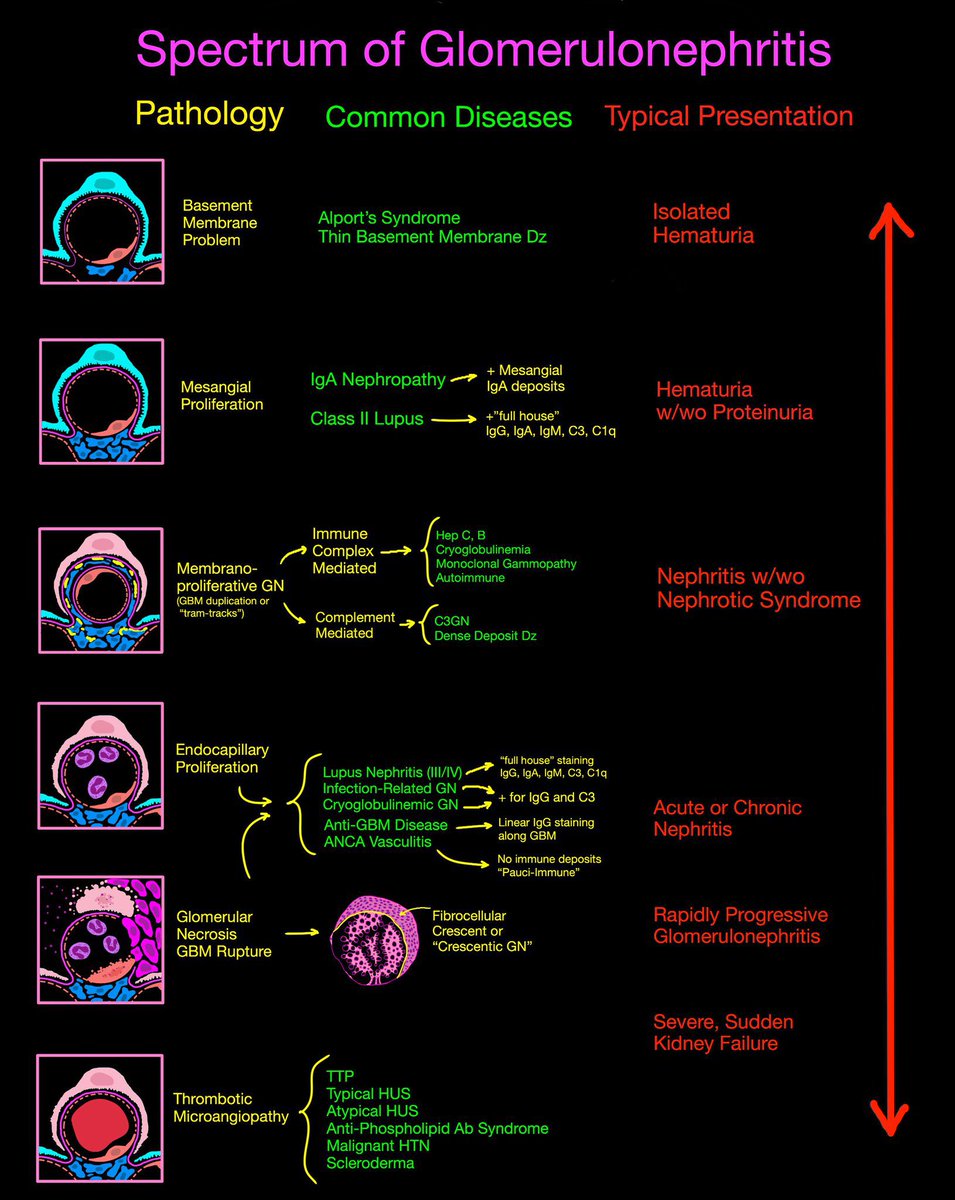
Glomerulonephritis ✨
Which is a condition where the tiny blood vessels in the kidneys become inflamed and damaged
Glomerulonephritis ✨
Which is a condition where the tiny blood vessels in the kidneys become inflamed and damaged
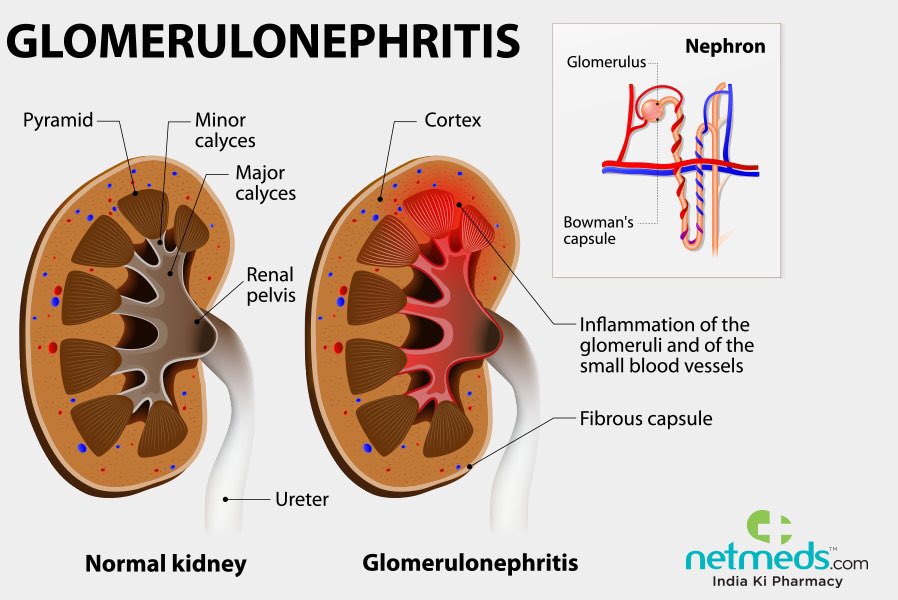
It’s usually caused by antigen-antibody complexes deposition in the glomerular tissue👉🏼activate complement system 👉🏼 lead to inflammation 😳
Quick recap!😊
The endothelium of the fenestrated capillaries are covered with negatively charged proteoglycans & glycosaminoglycans.
Quick recap!😊
The endothelium of the fenestrated capillaries are covered with negatively charged proteoglycans & glycosaminoglycans.
The glomerular basement membrane connects the capillaries and the surrounding Bowman’s capsule thus it is also covered with proteoglycans👉🏼 negatively charged
Picture is from: cjasn.asnjournals.org
Picture is from: cjasn.asnjournals.org
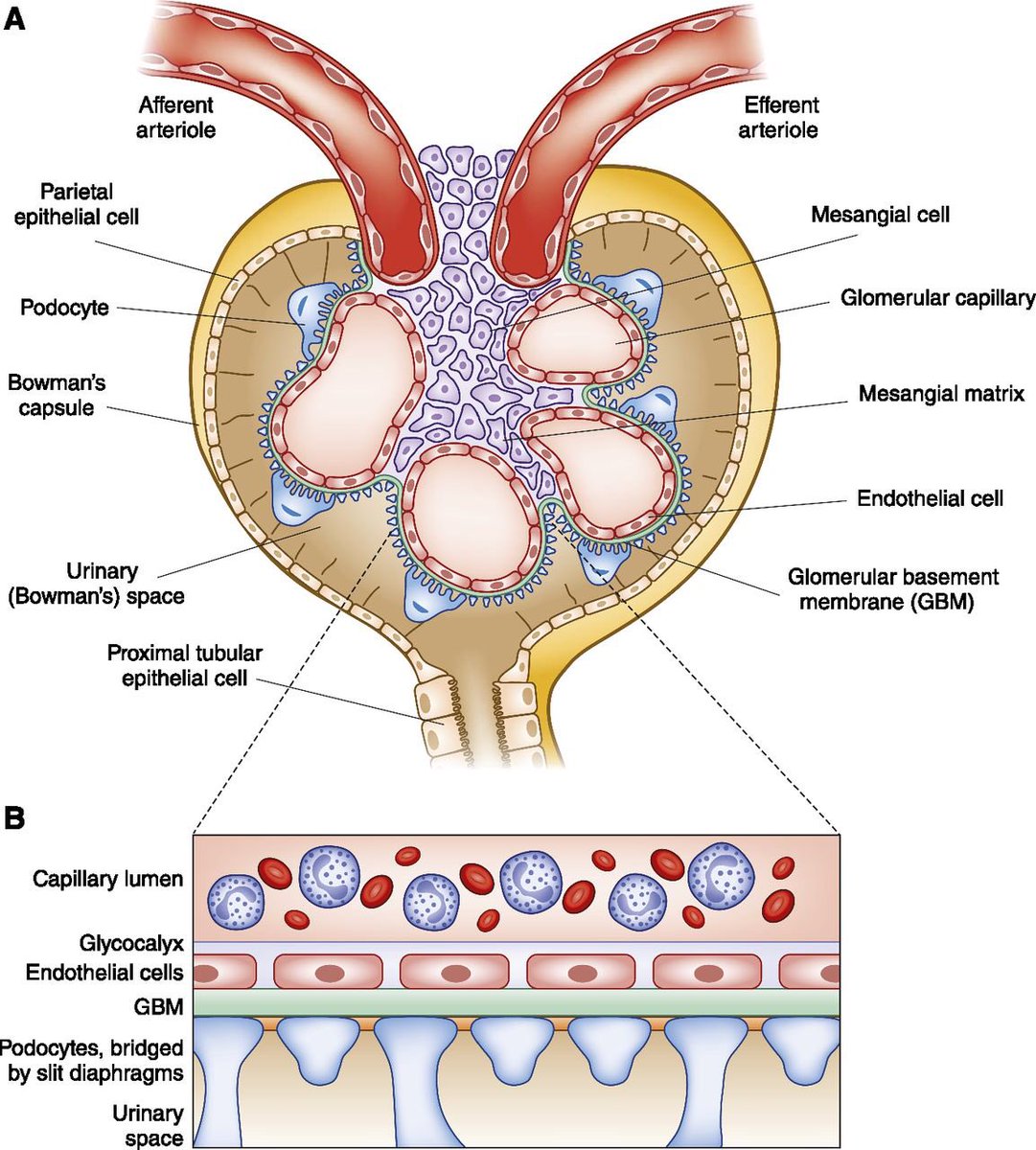
The cells of the visceral layer of Bowman’s capsule are called podocytes, whose processes also form a kind of meshwork
This meshwork prevents filtration of large molecules and anions
💪🏼😤
This meshwork prevents filtration of large molecules and anions
💪🏼😤
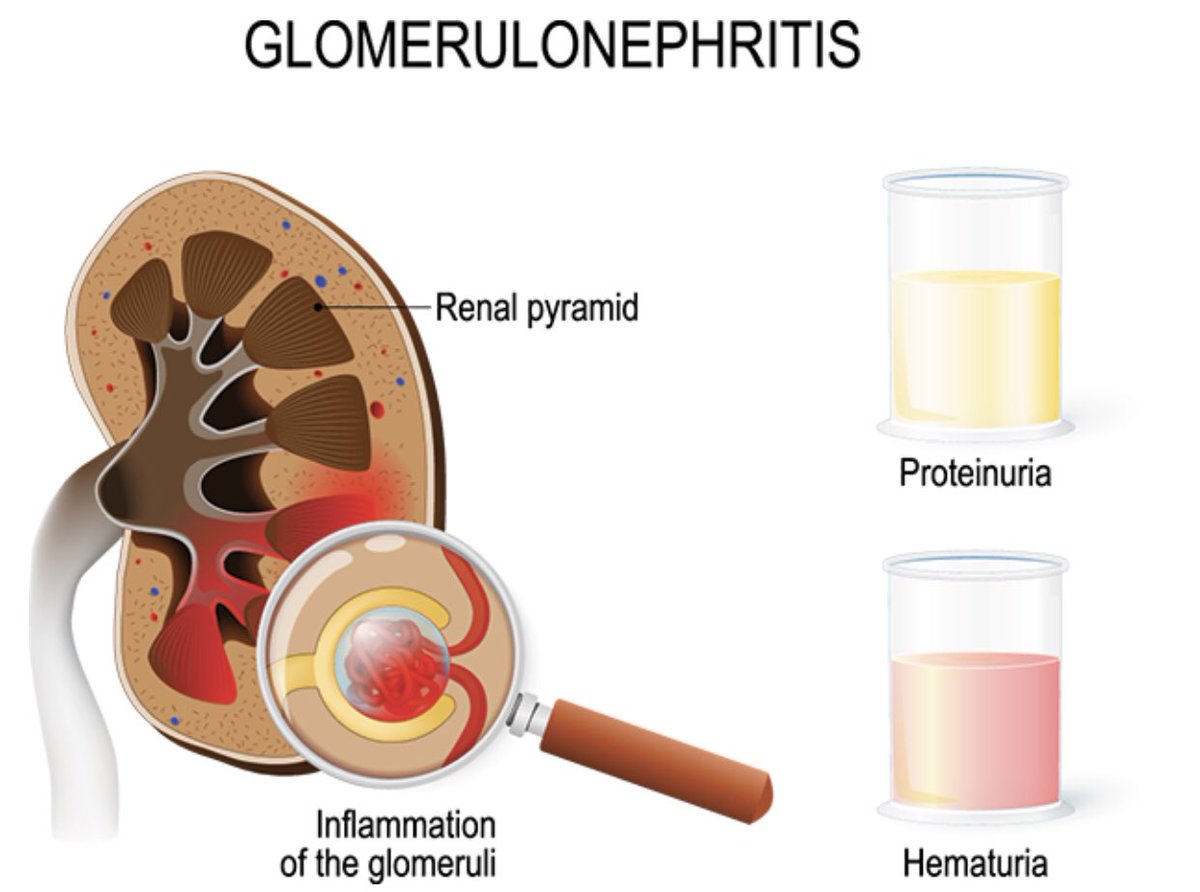
When damaged the membrane permeability ⬆️ and large molecules like protein and blood are filtered ☹️
It can cause the diagnostic features of proteinuria and hematuria
Picture is from: healthychildren.org
It can cause the diagnostic features of proteinuria and hematuria
Picture is from: healthychildren.org
Since the door is open & large molecules enter👉🏼fluid leakage will ⬇️pressure difference 👉🏼 will eventually decrease the GFR due to ongoing damage in the glomeruli
Low GFR👉🏼Low urine output
Possible increased fluid retention
👉🏼 Oedema
Picture’s from: armandoh.org
Low GFR👉🏼Low urine output
Possible increased fluid retention
👉🏼 Oedema
Picture’s from: armandoh.org
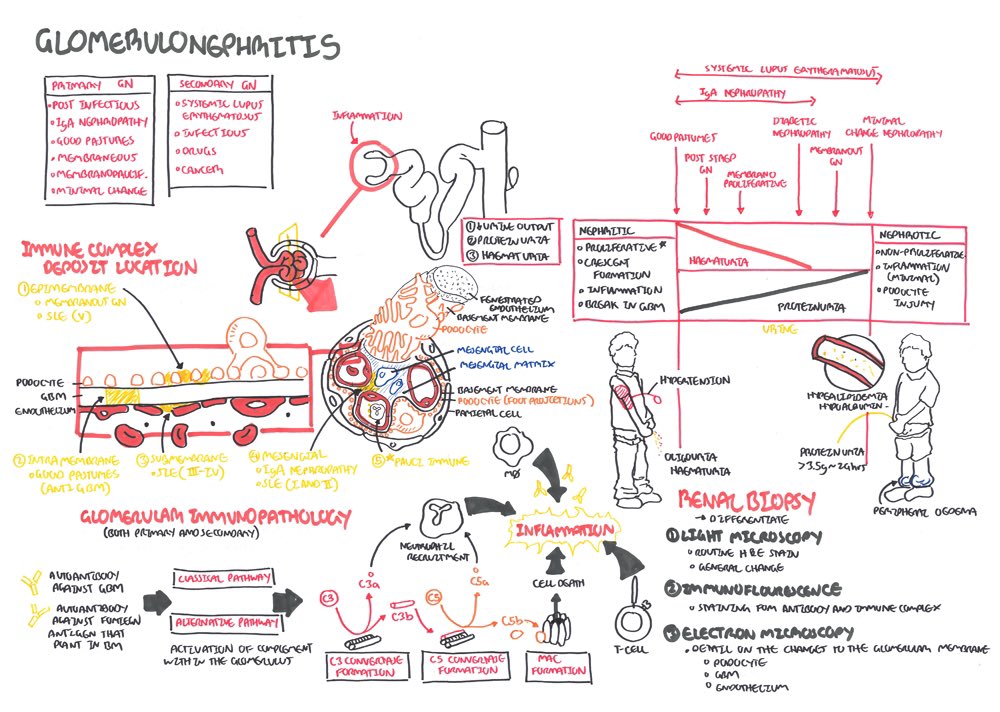
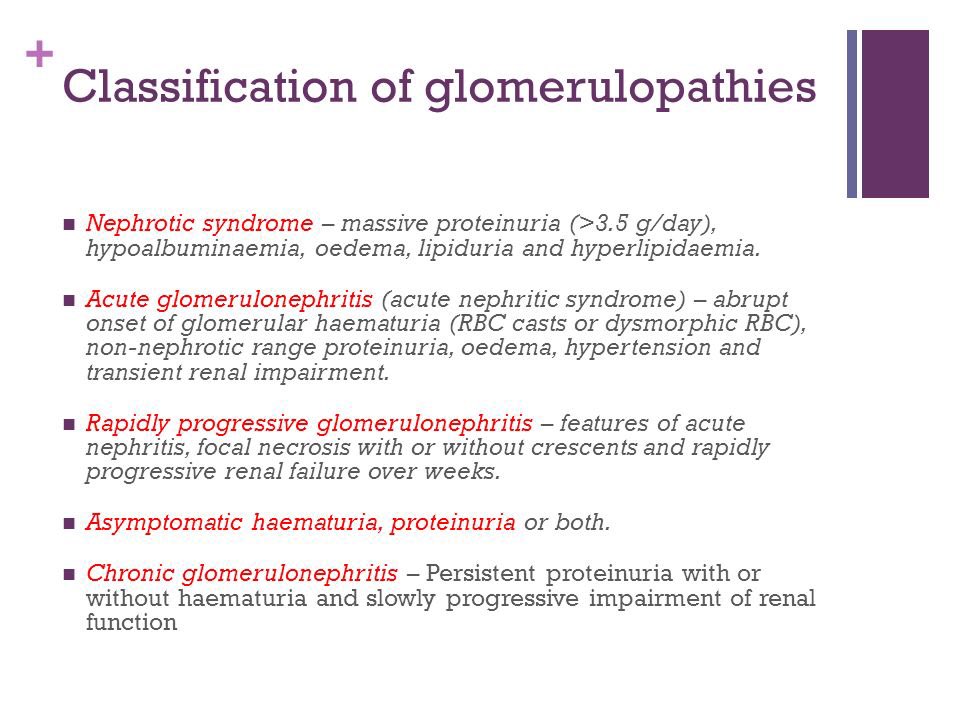
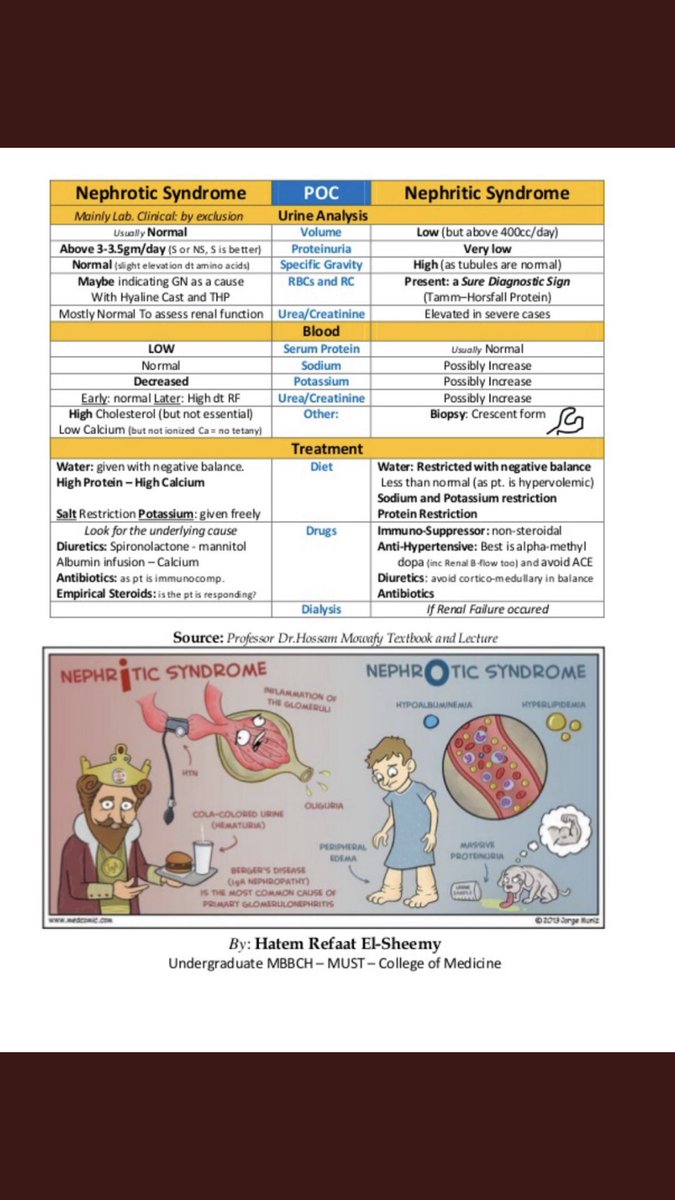
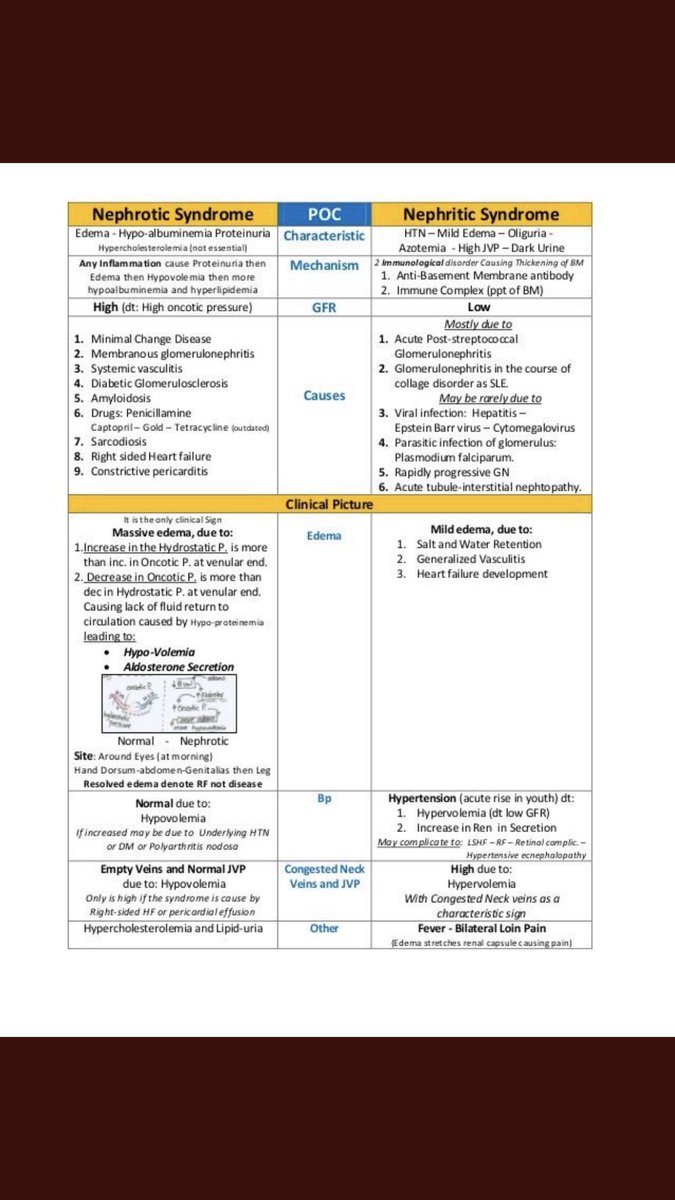
The classification of glomerulopathies and the difference between nephrotic and nephritic syndrome 👌🏼😍
Image is from: google.com
Image is from: google.com
I hope you enjoyed this summarised thread
Thank you for reading it 🙏🏼☺️
Thank you for reading it 🙏🏼☺️

Loading suggestions...