

#URINARY_TRACT_INFECTIONS🦠💊
Introduction
1. Most common bacterial infection in humans: 7 million office visits per year; 1 million hospitalizations
2. Many women (15%–20%) will have a urinary tract infection (UTI) during their lifetime
#ACCP
Introduction
1. Most common bacterial infection in humans: 7 million office visits per year; 1 million hospitalizations
2. Many women (15%–20%) will have a urinary tract infection (UTI) during their lifetime
#ACCP
3. 1–50 years of age: UTIs occur predominantly in women; after 50: men are increasingly affected because
of prostate problems B.
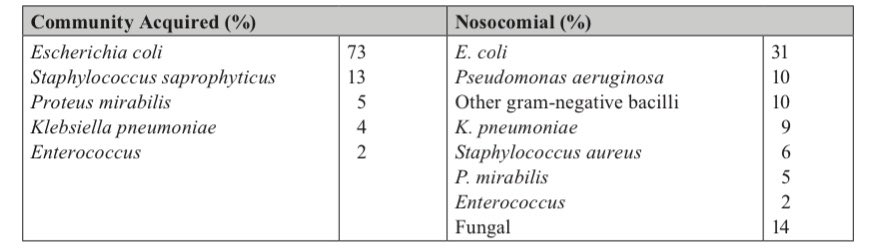
🦠Microbiology 🔬
Incidence of Urinary Tract Infections by Organism:
#ACCP
of prostate problems B.
🦠Microbiology 🔬
Incidence of Urinary Tract Infections by Organism:
#ACCP
📍Predisposing Factors :
1. Age
2. Female sex
3. Diabetes mellitus
4. Pregnancy
5. Immunosuppression
6. Urinary tract instrumentation
7. Urinary tract obstruction
8. Renal disease, renal transplantation 9. Neurologic dysfunction
#URINARY_TRACT_INFECTIONS🦠
#ACCP
1. Age
2. Female sex
3. Diabetes mellitus
4. Pregnancy
5. Immunosuppression
6. Urinary tract instrumentation
7. Urinary tract obstruction
8. Renal disease, renal transplantation 9. Neurologic dysfunction
#URINARY_TRACT_INFECTIONS🦠
#ACCP
📍Clinical Presentation:
1. Lower UTI: Cystitis (older adults may have only nonspecific symptoms, such as mental status changes,
abdominal pain, and decreased eating or drinking) a. Dysuria
b. Frequent urination
c. Urgency
d. Occasionally, gross hematuria
#ACCP 💊
1. Lower UTI: Cystitis (older adults may have only nonspecific symptoms, such as mental status changes,
abdominal pain, and decreased eating or drinking) a. Dysuria
b. Frequent urination
c. Urgency
d. Occasionally, gross hematuria
#ACCP 💊
2. Upper UTI: Pyelonephritis (older adults may have only nonspecific symptoms, such as mental status
changes, abdominal pain, and decreased eating or drinking)
changes, abdominal pain, and decreased eating or drinking)
a. Frequency, dysuria, hematuria
b. Suprapubic pain
c. Costovertebral angle tenderness; flank pain
d. Fever, chills
e. Elevated WBC
f. Nausea, vomiting
#ACCP
#Infectious_Diseases🦠
b. Suprapubic pain
c. Costovertebral angle tenderness; flank pain
d. Fever, chills
e. Elevated WBC
f. Nausea, vomiting
#ACCP
#Infectious_Diseases🦠
📝 Diagnosis:
Urinalysis (blood cultures will be positive in 20% of patients with upper UTIs)
1. Pyuria (WBC greater than 10 cells/mm3)
2. Bacteriuria (more than 102 colony-forming units per milliliter is diagnostic) in symptomatic patients or
those with catheters
#ACCP 🦠💊
Urinalysis (blood cultures will be positive in 20% of patients with upper UTIs)
1. Pyuria (WBC greater than 10 cells/mm3)
2. Bacteriuria (more than 102 colony-forming units per milliliter is diagnostic) in symptomatic patients or
those with catheters
#ACCP 🦠💊
3. Red blood cells
4. Cloudiness
5. Nitrite positive (E. coli, Proteus, Klebsiella)
6. Leukocyte esterase positive
7. Casts (if pyelonephritis)
8. Note: patient must also have symptoms; diagnosis cannot be made on urinalysis results alone.
#ACCP 💊🦠
#Infectious_Diseases 🦠
4. Cloudiness
5. Nitrite positive (E. coli, Proteus, Klebsiella)
6. Leukocyte esterase positive
7. Casts (if pyelonephritis)
8. Note: patient must also have symptoms; diagnosis cannot be made on urinalysis results alone.
#ACCP 💊🦠
#Infectious_Diseases 🦠
📍Therapy :💊
1. Uncomplicated cystitis
a. Recommended therapy
i. Trimethoprim/sulfamethoxazole 160 mg/800 mg twice daily for 3 days. Avoid if resistance
prevalence is known to exceed 20% or if used for UTI in previous 3 months.
#Infectious_Diseases
1. Uncomplicated cystitis
a. Recommended therapy
i. Trimethoprim/sulfamethoxazole 160 mg/800 mg twice daily for 3 days. Avoid if resistance
prevalence is known to exceed 20% or if used for UTI in previous 3 months.
#Infectious_Diseases
📍Therapy : 💊
ii. Nitrofurantoin monohydrate/macrocrystals 100 mg twice daily for 5 days (ineffective in
patients with a CrCl less than 30 mL/minute/1.73 m2) iii. Fosfomycin tromethamine 3 g, one dose.
ii. Nitrofurantoin monohydrate/macrocrystals 100 mg twice daily for 5 days (ineffective in
patients with a CrCl less than 30 mL/minute/1.73 m2) iii. Fosfomycin tromethamine 3 g, one dose.
📍Alternatives:💊
i. Fluoroquinolones (not moxifloxacin) for 3 days – Because of serious adverse effects, avoid
fluoroquinolones if there are other treatment options.
ii. β-Lactams (amoxicillin-clavulanate, cefdinir, cefaclor, cephalexin, and cefpodoxime proxetil)
for 5–7 days.
i. Fluoroquinolones (not moxifloxacin) for 3 days – Because of serious adverse effects, avoid
fluoroquinolones if there are other treatment options.
ii. β-Lactams (amoxicillin-clavulanate, cefdinir, cefaclor, cephalexin, and cefpodoxime proxetil)
for 5–7 days.
📍Inpatient therapy:💊
i. Fluoroquinolone
ii. Aminoglycoside
iii. Ceftriaxone (consider a β-lactam with antipseudomonal activity in patients recently hospital-
ized or with urinary catheters or living in nursing homes)
iv. Therapy duration: 5–14 days (5 days with levofloxacin)
i. Fluoroquinolone
ii. Aminoglycoside
iii. Ceftriaxone (consider a β-lactam with antipseudomonal activity in patients recently hospital-
ized or with urinary catheters or living in nursing homes)
iv. Therapy duration: 5–14 days (5 days with levofloxacin)
📍Uncomplicated pyelonephritis:
a. Outpatient therapy (if patient is not immunocompromised or does not have nausea and vomiting)
i. Trimethoprim/sulfamethoxazole 160 mg/800 mg twice daily for 14 days
#ACCP 🦠
a. Outpatient therapy (if patient is not immunocompromised or does not have nausea and vomiting)
i. Trimethoprim/sulfamethoxazole 160 mg/800 mg twice daily for 14 days
#ACCP 🦠
ii. Levofloxacin 750 mg orally daily for 5 days or ciprofloxacin 500 mg orally twice daily for 7
days (not moxifloxacin) – Because of serious adverse effects, avoid fluoroquinolones if there
are other treatment options.
days (not moxifloxacin) – Because of serious adverse effects, avoid fluoroquinolones if there
are other treatment options.
iii. β-Lactams (see above) for 10–14 days (less effective than first two options)
b. Uropathogen resistance greater than 10%: Use initial dose of an intravenous, long-acting β-lactam (e.g., ceftriaxone) or once-daily aminoglycoside.
b. Uropathogen resistance greater than 10%: Use initial dose of an intravenous, long-acting β-lactam (e.g., ceftriaxone) or once-daily aminoglycoside.
📍Complicated UTIs💊
a. Outpatient therapy
i. Trimethoprim/sulfamethoxazole 160 mg/800 mg twice daily for 7-14 days
ii. Levofloxacin 750mg oral daily for 5 days or ciprofloxacin 500mg oral twice daily for 7 days
(not moxifloxacin)
iii. β-Lactams (see above) for 7–14 days
a. Outpatient therapy
i. Trimethoprim/sulfamethoxazole 160 mg/800 mg twice daily for 7-14 days
ii. Levofloxacin 750mg oral daily for 5 days or ciprofloxacin 500mg oral twice daily for 7 days
(not moxifloxacin)
iii. β-Lactams (see above) for 7–14 days
📍Pregnancy (pregnant women should be screened for bacteriuria and treated, even if asymptomatic)
a. Antibiotic options
i. Amoxicillin/clavulanate for 3-5 days
ii. Nitrofurantoin (avoid in the first trimester and at term if other options available) for 5 days 💊
a. Antibiotic options
i. Amoxicillin/clavulanate for 3-5 days
ii. Nitrofurantoin (avoid in the first trimester and at term if other options available) for 5 days 💊
iii. Cephalexin or cefpodoxime proxetil for 3-5 days
iv. Fosfomycin tromethamine single dose.
iv. Fosfomycin tromethamine single dose.
Loading suggestions...