

For the fellows, this case is the penultimate learning case for bleeding. Prepare yourself this is THE nightmare.
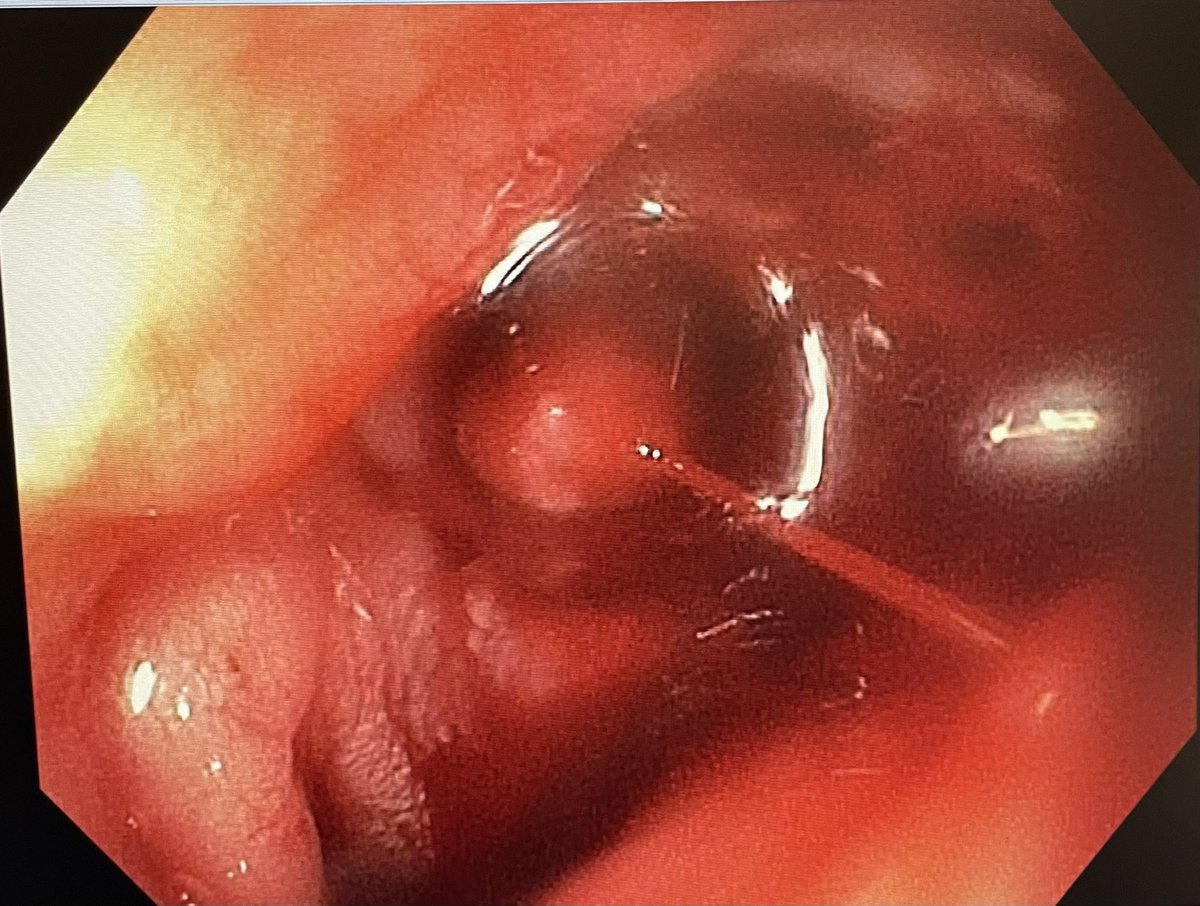
You see this duodenal ulcer with adherent clot. What you would you do next?
#GITwitter @ScopingSundays
You see this duodenal ulcer with adherent clot. What you would you do next?
#GITwitter @ScopingSundays

What do you think do next?
You disrupt the clot and arterial bleeding ensues. Your mother always told you not to pick scabs (Forrest 2b)!
Now what?
Now what?

What do you do next?
The bipolar probe 7Fr was too small, 10Fr was too stiff and the scope tip could not reach the vessel.

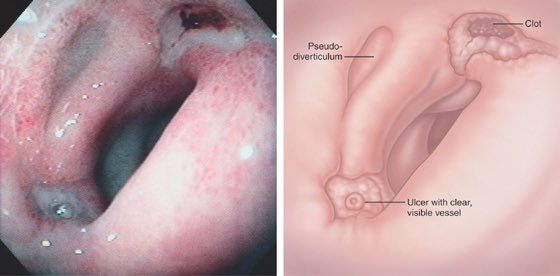
Note the anatomical orientation of the duodenal bulb. Knowing the device exits a gastroscope at 7 o’clock, we can understand why posterior/superior ulcers are hard to reach.

As the bipolar probe cannot reach the target vessel, what would you do next?
The patient is destabilizing.
The patient is destabilizing.
Hemospray is attempted even with modified Bonewax tipped catheter technique, but technical failure (clogged catheter).
Note: The clear cap allows tamponade of the vessel, buying precious time. This allowed stat blood to be delivered, new IV, IR to be alerted, and OTSC to load.
Note: The clear cap allows tamponade of the vessel, buying precious time. This allowed stat blood to be delivered, new IV, IR to be alerted, and OTSC to load.

While tamponade was held for 5 minutes…
Hemospray was prepared and multiple scopes, including duodenoscope (En fos view) and another gastroscope (preload OTSC) were brought in.
IR cleared their next case for us.
A breath was taken.
Think plan C, D as your move to plan B.
Hemospray was prepared and multiple scopes, including duodenoscope (En fos view) and another gastroscope (preload OTSC) were brought in.
IR cleared their next case for us.
A breath was taken.
Think plan C, D as your move to plan B.
The duodenoscope was attempted but quickly abandoned as the pylorus could not be crossed blind through a torrent of blood.
What’s left ?
OTSC was successful.
Three reasons:
1. OTSC does not reduce the flexibility of the scope tip (only tripwire in channel)
2. Suction is permitted.
3. Clear cap tamponade is built in.
Three reasons:
1. OTSC does not reduce the flexibility of the scope tip (only tripwire in channel)
2. Suction is permitted.
3. Clear cap tamponade is built in.

Loading suggestions...