

1/ #IDTwitter #HIVTwitter
Let’s begin session 2 of our #HIVResistance Tweetorial series: Basic Principles.
Let’s begin session 2 of our #HIVResistance Tweetorial series: Basic Principles.
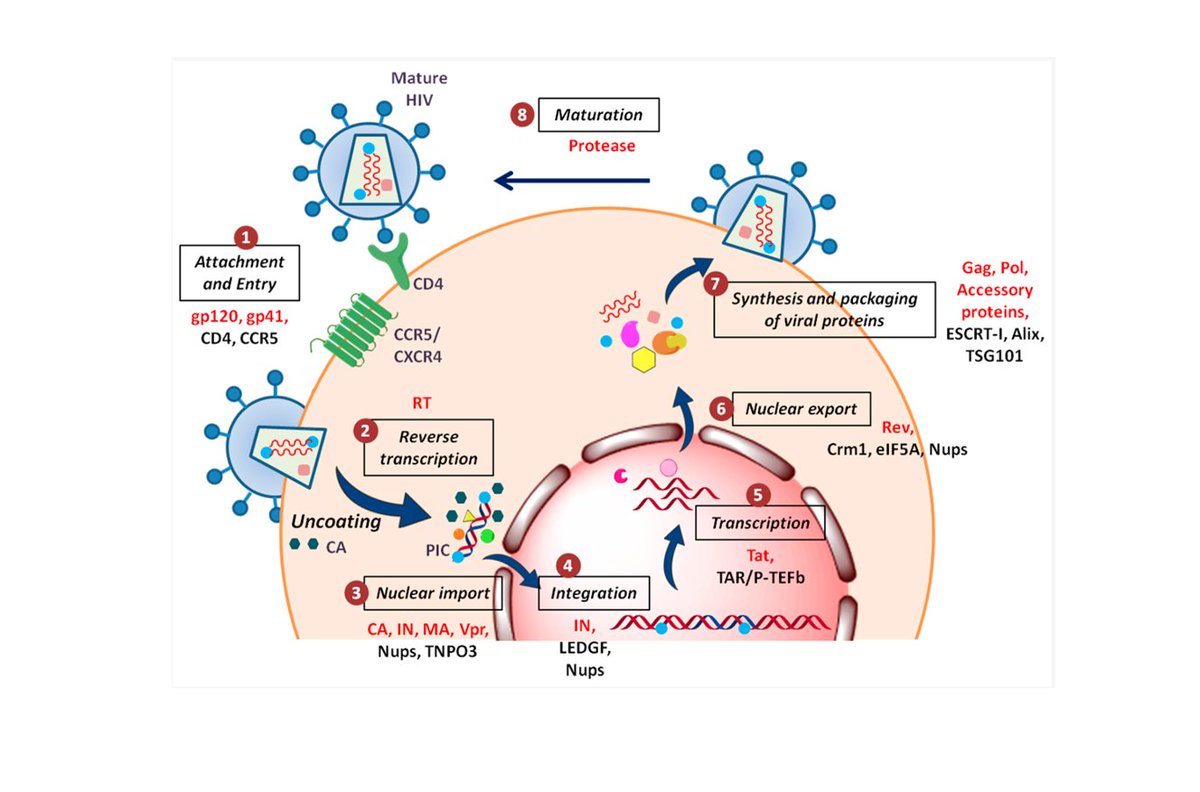
2/ Let’s review the steps of HIV viral replication:
1.Attachment and entry
2.Reverse transcription (viral RNA viral dsDNA)
3.Nuclear import
4.Integration
5.Transcription
6.Nuclear export
7.Protein synthesis and packaging
8.Maturation
1.Attachment and entry
2.Reverse transcription (viral RNA viral dsDNA)
3.Nuclear import
4.Integration
5.Transcription
6.Nuclear export
7.Protein synthesis and packaging
8.Maturation
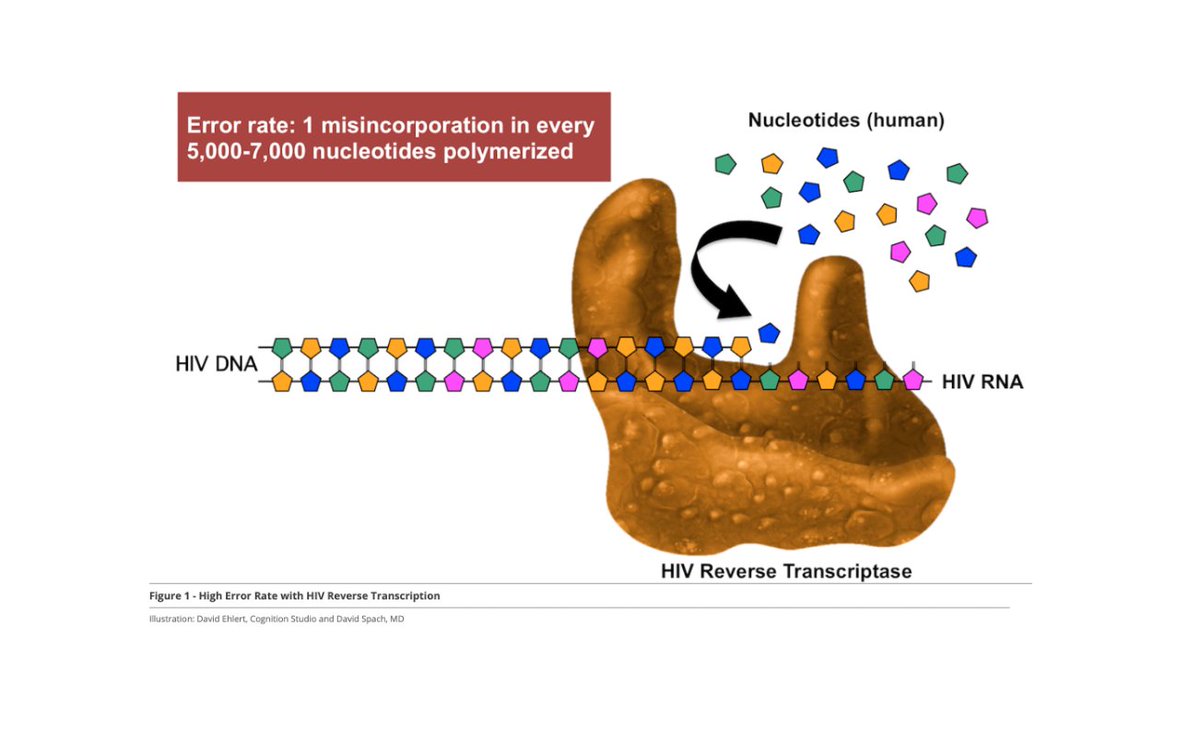
3/ Reverse transcriptase (RT) is responsible for step #2: synthesizing viral DNA from a viral RNA template. HIV can replicate at extremely high rates BUT RT is quite prone to errors. It incorporates an incorrect nucleotide every ~6,000 bases or so.
4/ If we invoke the central dogma of biology (DNA->RNA->protein) we can deduce that the errors made by RT will result in changes in the viral DNA, viral RNA, and ultimately viral amino acid (AA) sequences. A change in AA sequence -> change in protein structure.
5/ Sometimes these changes in the protein structures of HIV reverse transcriptase, protease, and/or integrase makes our ART ineffective (in other words, these changes make our NRTIs, NNRTIs, PIs, and INSTIs ineffective against that particular HIV).
6/ Often, the errors made by RT (which I’ll refer to as mutations) confer a fitness cost to the virus. This just means that these errors can make HIV less efficient at replicating.

7/ In the absence of ART, HIV virions with wildtype (wt) sequence tend to predominate within a given person’s population of HIV virions since wt virions are more efficient at replicating vs virions with mutations.
8/ If a patient receives an ART regimen that does not fully suppress viral replication (either because the regimen is inadequate and/or the patient is nonadherent), virions with mutations that enable them to replicate despite drug presence have a selective advantage.
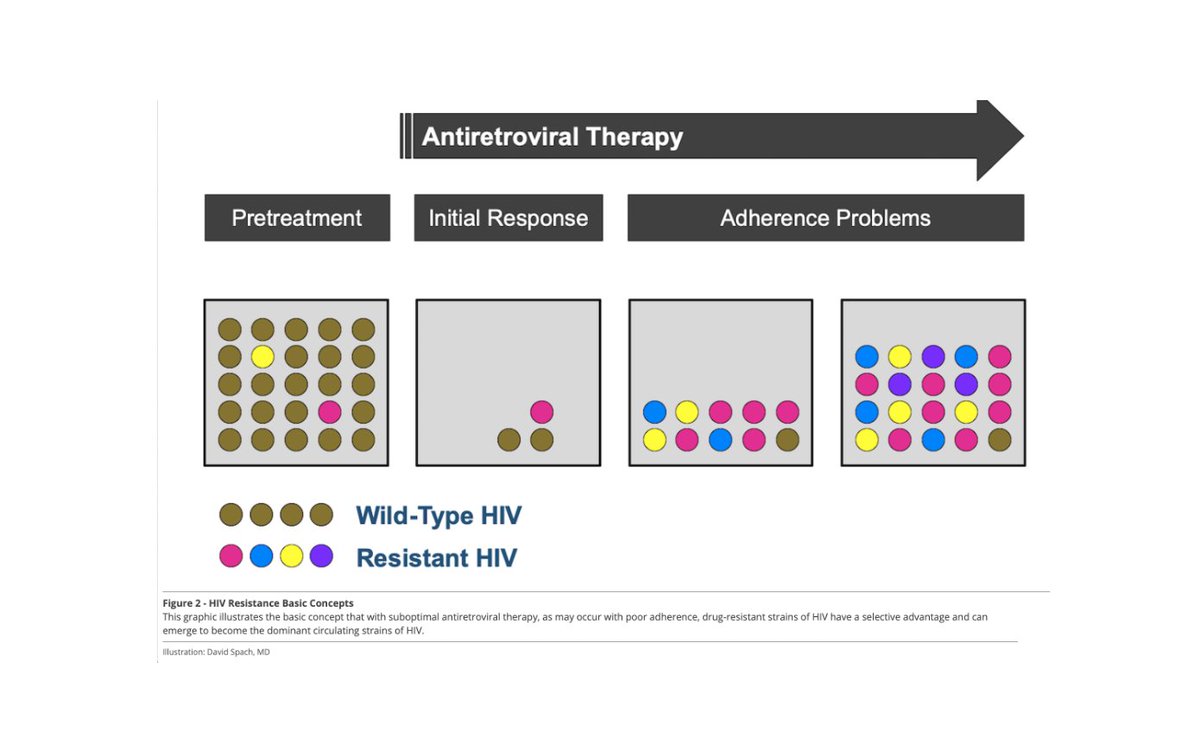
9/ And over time, these virions will be the predominate virions within the viral population. This leads to virologic failure to either some or all of the components in the patient’s regimen.
This image from UofW is SO important I included it twice.
This image from UofW is SO important I included it twice.
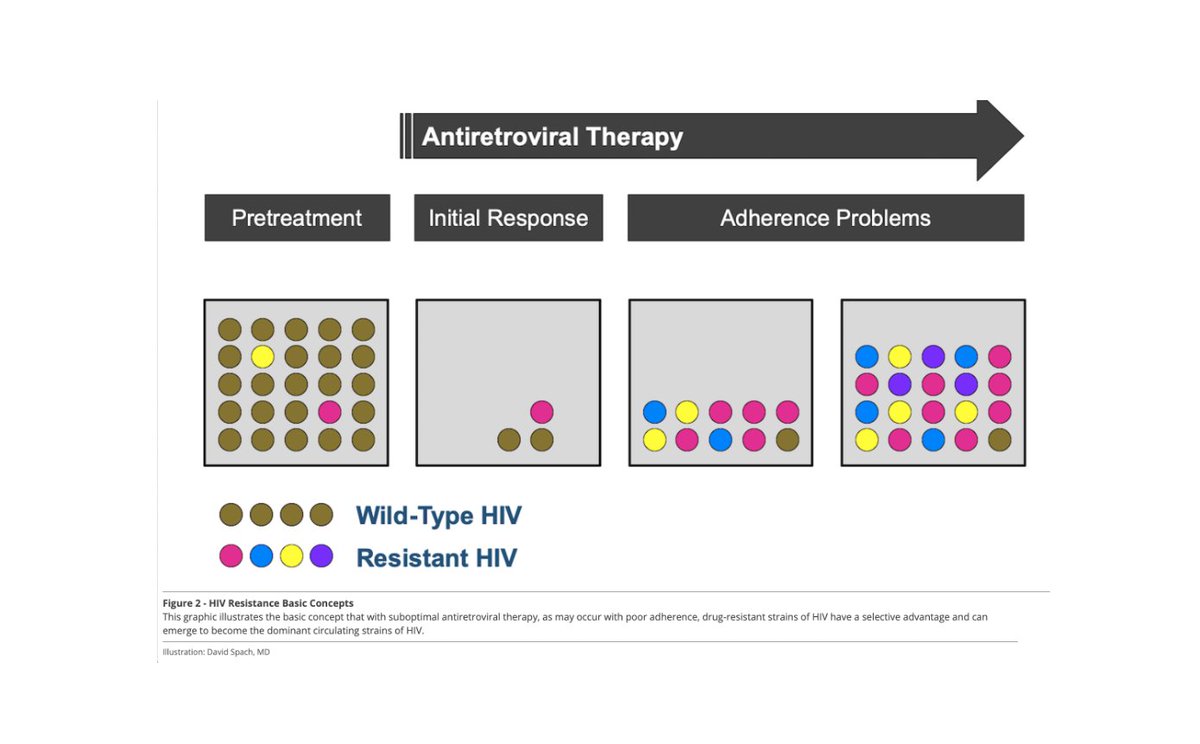
10/ Often when the medications to which the patient’s virus is resistant are stopped, the majority of their HIV virions will revert to wildtype. This is because, in the absence of drug, there is no longer a selective advantage for virions harboring resistance mutations.
11/ Key Clinical Correlate #1
Patients struggling w/ adherence are sometimes better off stopping their regimen while adherence barriers are addressed vs continuing w/ poor adherence. This is a complicated topic we’ll delve into later.
Patients struggling w/ adherence are sometimes better off stopping their regimen while adherence barriers are addressed vs continuing w/ poor adherence. This is a complicated topic we’ll delve into later.

12/ Key Clinical Correlate #2
Resistance testing done after a patient has been completely off their regimen for 4 weeks or more cannot fully be trusted since their virus may have reverted to wildtype. Specificity is good but sensitivity, not so much.
Resistance testing done after a patient has been completely off their regimen for 4 weeks or more cannot fully be trusted since their virus may have reverted to wildtype. Specificity is good but sensitivity, not so much.

13/ Key Clinical Correlate #3
HIV drug resistance really cannot develop in the absence of viral replication. Thus, if a patient is adherent to an effective regimen and they remain suppressed, they will not develop drug resistance.
HIV drug resistance really cannot develop in the absence of viral replication. Thus, if a patient is adherent to an effective regimen and they remain suppressed, they will not develop drug resistance.

14/ I hope this throwback to high school biology was helpful. Next time we will review transmitted vs acquired drug resistance.
Loading suggestions...