
1) Welcome to our accredited tweetorial on optimal contemporary chronic mgt of #hyperkalemia. Earn 0.5h CME/CE credit by following this thread. I am @edgarvlermamd. @MedTweetorials #medtwitter #cardiotwitter #endotwitter #nephtwitter #nephjc @kidney_boy @DanielJDrucker

Supported by educational grants from Abbott, AstraZeneca, Bayer, Chiesi, NovoNordisk. This program is intended for healthcare providers.
2) First, a case: 67M with T2D, HTN, HFpEF is referred for CKD evaluation. Meds include Metformin, Lisinopril, Amlodipine, and Metoprolol. Pertinent Labs: Na 138, K 5.8, BUN/ Crea 32/ 2.6, A1C 7.6%.
3) Risk Factors for #hyperkalemia include: Advanced stages of #CKD, #heartfailure, resistant #hypertension, #diabetes, myocardial infarction (#MI), and/or, combinations of these conditions (pubmed.ncbi.nlm.nih.gov, pubmed.ncbi.nlm.nih.gov, pubmed.ncbi.nlm.nih.gov)

pubmed.ncbi.nlm.nih.gov/28866674/
Association of Serum Potassium with All-Cause Mortality in Patients with and without Heart Failure, Chronic Kidney Disease, and/or Diabetes - PubMed
Mortality risk progressively increased with dyskalemia and was differentially greater in those with...
pubmed.ncbi.nlm.nih.gov/27418967/
pubmed.ncbi.nlm.nih.gov/28158516/
4) Additional risk factors include #RAASi usage, advanced age, and drugs such as #heparin, ẞ-blockers, nonsteroidal anti-inflammatory drugs, #calcineurin inhibitors, #trimethoprim, #pentamidine, and K-sparing diuretics.
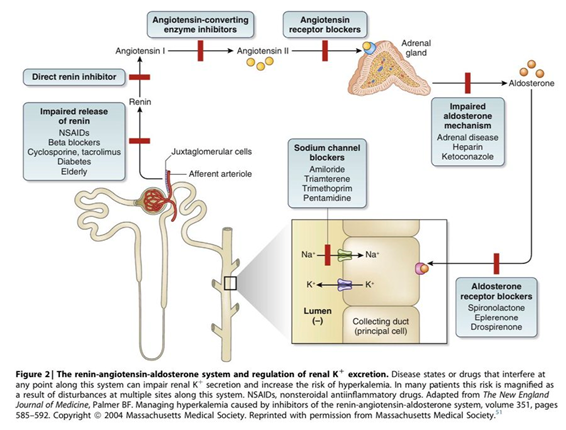
5) The risk of hyperkalemia progressively increases as eGFR decreases <15 mL/min per 1.73 m2. See ncbi.nlm.nih.gov and pubmed.ncbi.nlm.nih.gov
6) Furthermore, patients receiving #RAASi therapy who have an eGFR < 60 mL/min per 1.73 m2 have an elevated #hyperkalemia risk, which progressively increases as eGFR decreases.
7) RAASi are recommended for patients with hypertension, HF, stable coronary artery disease, CKD, diabetic kidney disease (#DKD), and diabetes. They improve survival in patients with CKD, HF, and post-MI status and also provide kidney benefits in patients with non-DKD and DKD.
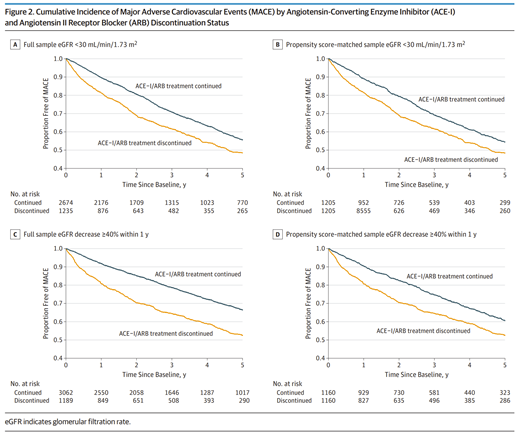
8) In a cohort study of patients who experienced a decline in eGFR to < 30 while receiving RAASi therapy, discontinuation of RAASi therapy was associated with a higher risk of mortality or major adverse cardiovascular events (MACE) than continuation of RAASi.
9) What are the treatment options for the management of his hyperkalemia?
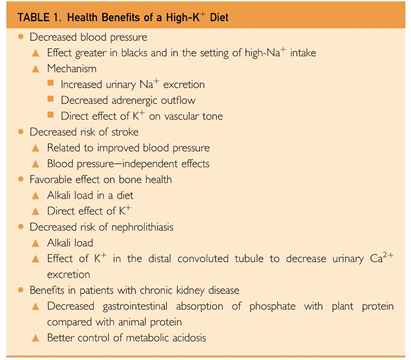
A. Diet
B. Removal of other hyperkalemia-causing drugs
C. Use of diuretics
D. Modification of RAASi dose
E. K+ binders
A. Diet
B. Removal of other hyperkalemia-causing drugs
C. Use of diuretics
D. Modification of RAASi dose
E. K+ binders
10) Mark your answer and return tomorrow for more on this case and more education! @GrahamAbra @arvindcanchi @kidneydoc101 @caioqualunque
@goKDIGO @KatieKwonMD @kdjhaveri @ChristosArgyrop @logiebear111 @SLeonMD @nephondemand @ASNKidney @CardioNerds
@goKDIGO @KatieKwonMD @kdjhaveri @ChristosArgyrop @logiebear111 @SLeonMD @nephondemand @ASNKidney @CardioNerds
11) Welcome back! There's more to go on managing #hyperkalemia with the latest, safest options. I'm @edgarvlermamd. Encourage your colleagues, fellows, and residents to follow us here at @cardiomet_CE for serialized Twitter-based accredited education!
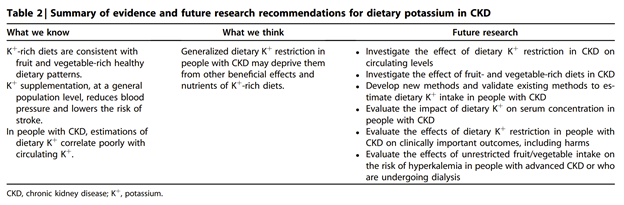
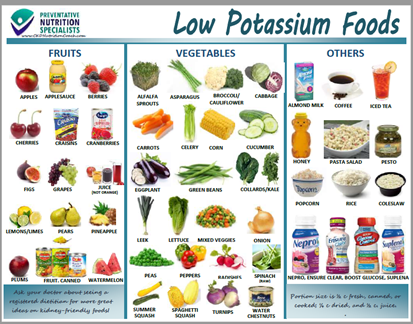
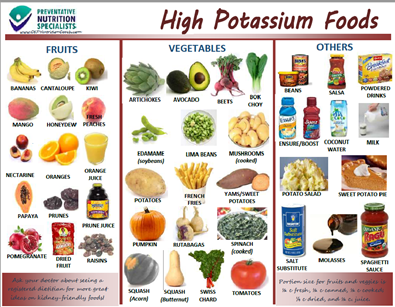
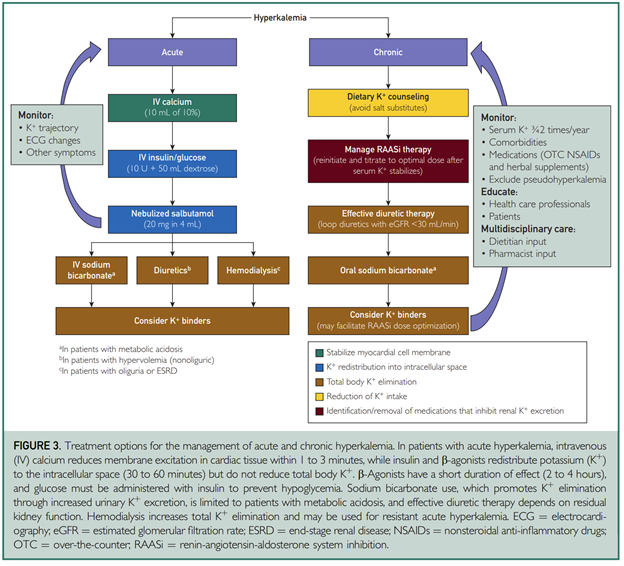
13) A low-K+ diet is difficult for patients to adhere to, particularly those who may have additional dietary restrictions due to #diabetes and reduced sodium intake for CKD or #heartfailure.
15) Diuretics promote urinary excretion of K+ in patients with CKD or DKD by stimulating the flow and delivery of K+ to the renal collecting ducts.
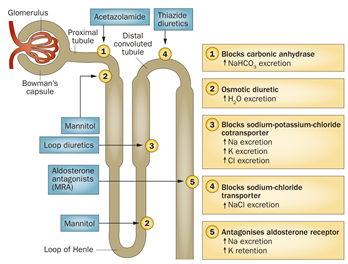
16) Despite beneficial effects of diuretics on volume status and BP, they may increase the risk of gout, volume depletion, decreased distal tubule flow, worsening kidney function, & reduced K+ excretion. Their effectiveness in managing hyperK+ relies on residual kidney function.
17) How about Fludrocortisone?
Fludrocortisone can also increase K+ excretion but is associated with an increased risk of fluid retention, hypertension, and vascular injury.
Fludrocortisone can also increase K+ excretion but is associated with an increased risk of fluid retention, hypertension, and vascular injury.
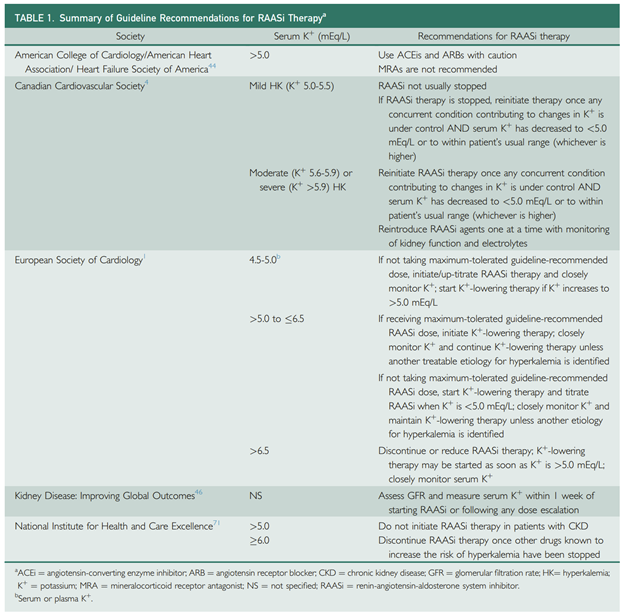
18) Discontinuation or dose reduction of #RAASi therapy may lead to adverse cardiorenal outcomes, and current guidelines differ with regard to recommendations on when to reinitiate RAASi.
19) The final options to consider are the K+ binders. Let’s look at some of the evidence supporting the use of these K+ binders.

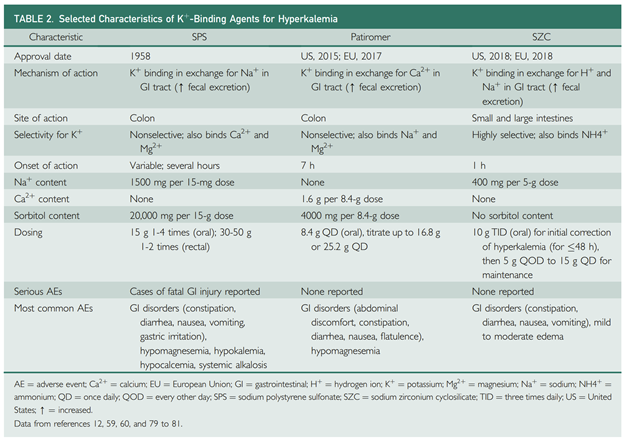
20) K+ binders used for hyperkalemia management are nonabsorbed and consist of a counter ion that is exchanged for K+ facilitating the elimination of bound K+ in the feces.
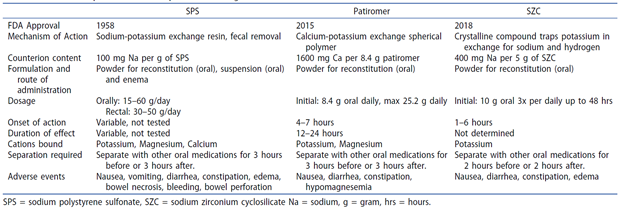
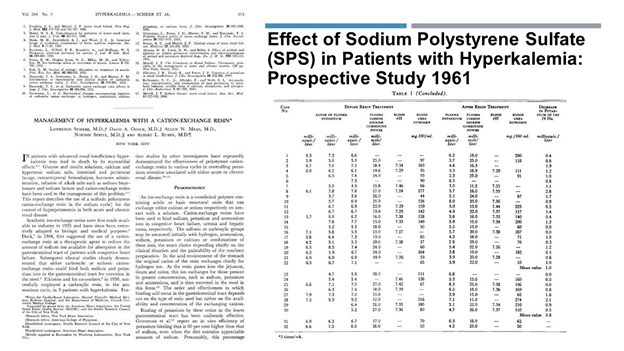
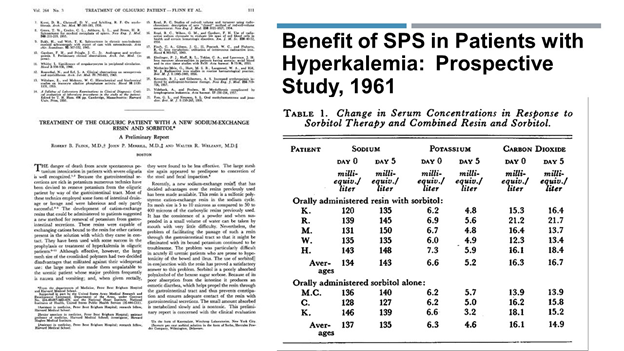
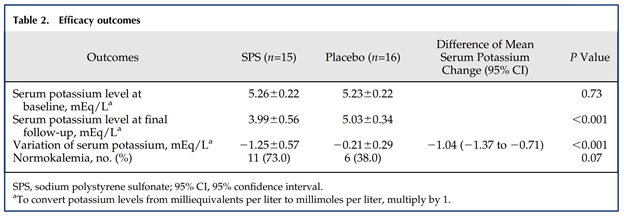
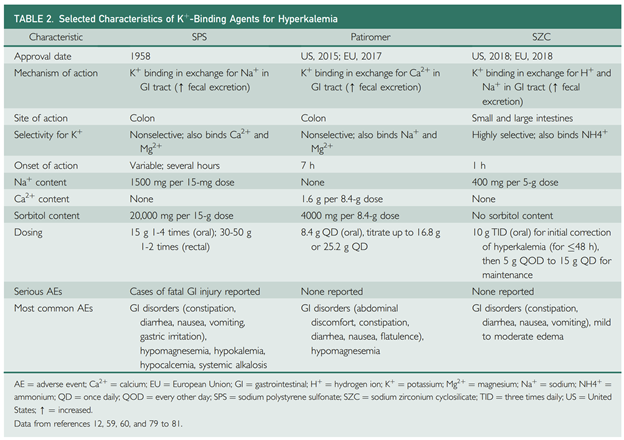
21) Sodium polystyrene sulfonate (SPS) is the K+ binder that has been available for hyperkalemia management for the longest time, and may continue to be the only agent available in parts of the world.
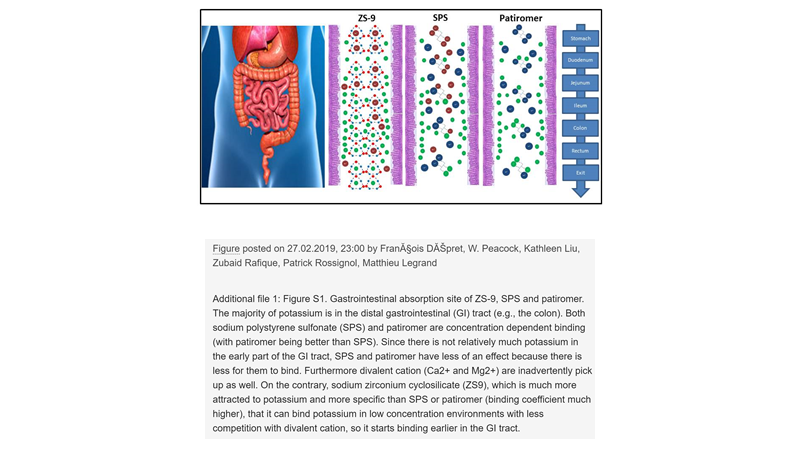
22) SPS is a polymeric cation-exchange resin that binds K+ ions in exchange for Na+ ions in the distal colon. It is nonselective for K+, with affinity for Ca2+ and Mg2+ ions. It may be given either orally or rectally (oral has poor palatability).
23) With only one small randomized, double-blind, 7-day trial, clinical studies supporting its long-term use in patients with hyperkalemia are lacking. Its short-term efficacy is also inconsistent, and the onset of action is variable (hours to days).
24) Two novel oral K+ binders are now approved in the US and the European Union: Patiromer sorbitex calcium and Sodium zirconium cyclosilicate (SZC; [formerly ZS-9]).

25) Do you know these drugs? What is/are the counter-ion for K+ exchange with SZC?
26) Mark your answer and return tomorrow for a detailed exploration of these new binders and a link to your free CE/#CME! @dr_nikhilshah @RenalFellowNtwk @HecmagsMD @Nephro_Sparks @AnnaGaddy @PharmERToxGuy @AliMehdiMD @ISNkidneycare @beaverspharmd @JamesNovakNeph
27) Welcome back! You are just a few clicks away from free #CME/CE. We are talking #hyperkalemia! I am @edgarvlermamd and this program is accredited by @academiccme. Previous programs (and credit!) available at cardiometabolic-ce.com.

28) Oral patiromer contains a Ca2+ sorbitol counterion that exchanges Ca2+ for K+ as it passes through the colon. Like SPS, it is a polymer that is nonselective for K+ and may also bind Mg2+ and small amounts of Na+.
29) Patiromer’s time to onset of action is approximately 7 hours. Administration should be separated from other oral medications by ≥ 3 hours because of the potential for binding.
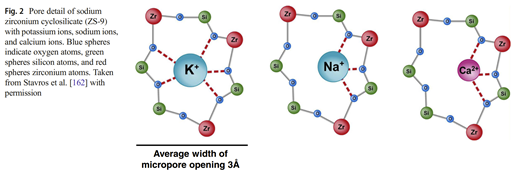
30) Unlike SPS and patiromer, SZC is nonpolymeric with high selectivity for K+ and NH4+ ions (1.25-fold higher affinity for K+ vs NH4+) in exchange for H+ and Na+ throughout the GIT. SZC binds monovalent cations (K+) as opposed to divalent cations (e.g., Ca2+ and Mg2+).
31) Because SZC may affect absorption of other oral medications with pH-dependent solubility due to a transient increase in gastric pH, SZC administration should be separated from these medications by ≥ 2 hours.
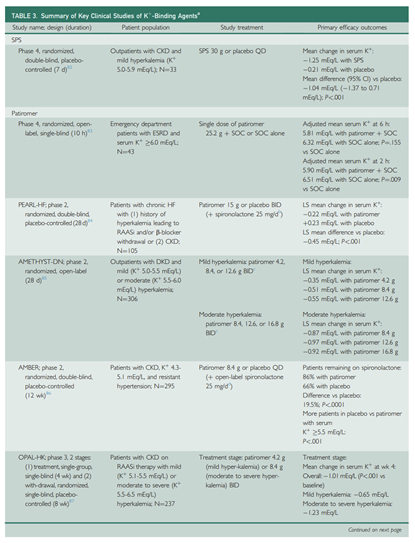
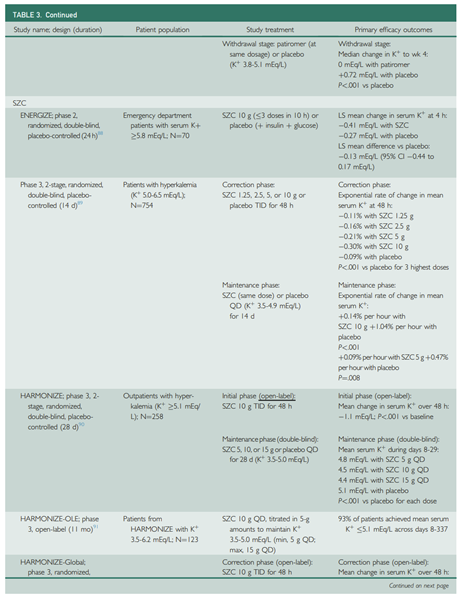
32) Look at the clinical evidence supporting these K+ binders
33) How about adverse events?
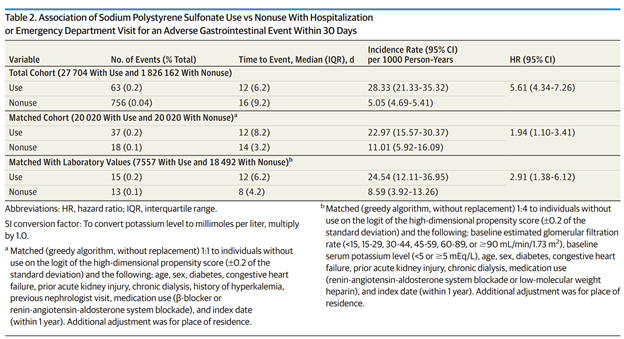
34) SPS has been associated with AEs, e.g., intestinal ischemia and colonic necrosis, a doubling in the risk of hospitalization for serious gastrointestinal AEs, and a reported overall mortality rate of 33% for patients with serious gastrointestinal injury.
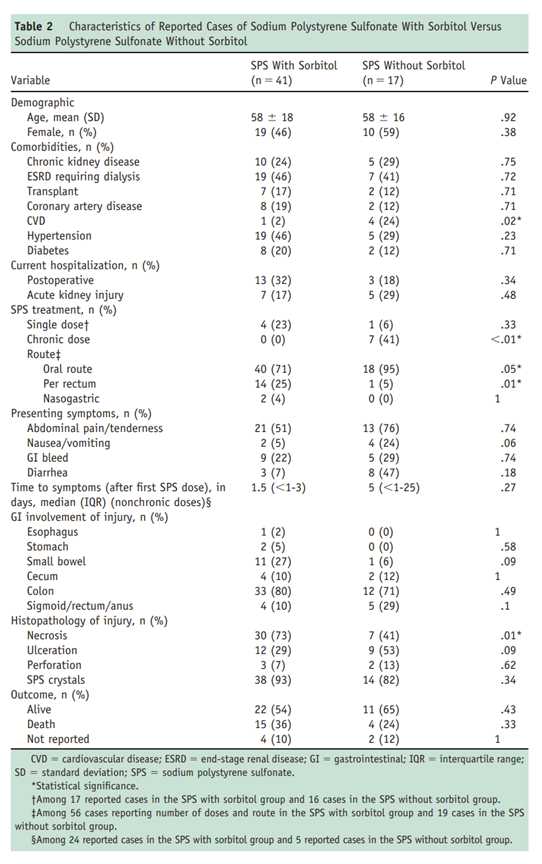
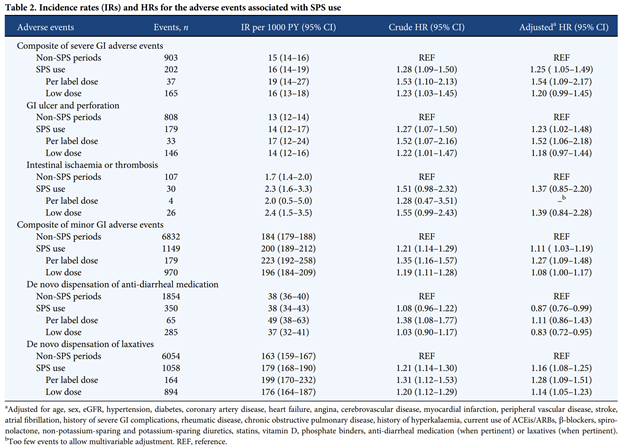
35) Although cohort studies have reported a higher relative risk of gastrointestinal AEs, the incidence of events with SPS was rare (16 or 23 events per 1000 person-years).
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
36) The most common AEs associated with patiromer therapy include gastrointestinal events (constipation, diarrhea, nausea/ vomiting, abdominal discomfort, and flatulence) and electrolyte disturbances (hypokalemia and hypomagnesemia) . . . as per
37) Like Patiromer, Sodium zirconium cyclosilicate has not been associated with any serious AEs in randomized trials. The most common AEs were hypokalemia and a dose-dependent increase in edema
nejm.org
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
nejm.org
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
38) The initiation of newer K+-binding agents should be considered in patients with chronic hyperkalemia despite optimized diuretic therapy and correction of metabolic acidosis.
39) After starting therapy at the recommended dose, K+ binders should be titrated for optimization of serum K+ concentration, with individualized monitoring of serum or plasma K+. Long-term K+-binder tx may be considered in patients with chronic hyperK as in the case presented.
40) The use of one of the newer K+-binding agents (SZC or patiromer) may allow for the continuation and optimization of #RAASi therapy in patients with #hyperkalemia.
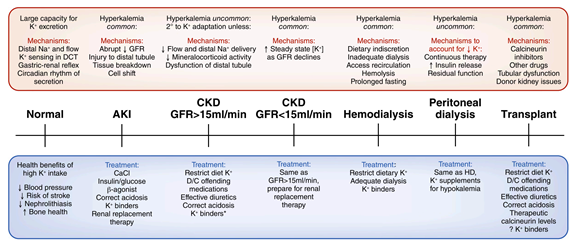
41) Here’s a nice algorithm to follow in the management of chronic hyperkalemia.
42) That's it! You made it! Free CE/#CME! Now, all you #physicians, #nurses, and #pharmacists, go to cardiometabolic-ce.com and claim your credit from @academiccme! I am @edgarvlermamd. Follow @cardiomet_CE for more tweetorials! #medtwittter #nephtwitter @MedTweetorials #FOAMed
Loading suggestions...