

تكره الجراحة والدورات؟ Fine✋🏻
ثريد بأهم النقاط العلمية التي تساعد في فهم السؤال ومن المفيد تذكرها قبل دخول اختبار SMLE 🔥 (يفضل مراجعتها قبل دخول الاختبار بيوم ليومين)
✅ سيتم اضافة النقاط المهمة والأسئلة كل ما تذكرت وتلقيت الأسئلة من الزملاء والزميلات
✅ نبدأ على بركة الله👇🏻
ثريد بأهم النقاط العلمية التي تساعد في فهم السؤال ومن المفيد تذكرها قبل دخول اختبار SMLE 🔥 (يفضل مراجعتها قبل دخول الاختبار بيوم ليومين)
✅ سيتم اضافة النقاط المهمة والأسئلة كل ما تذكرت وتلقيت الأسئلة من الزملاء والزميلات
✅ نبدأ على بركة الله👇🏻
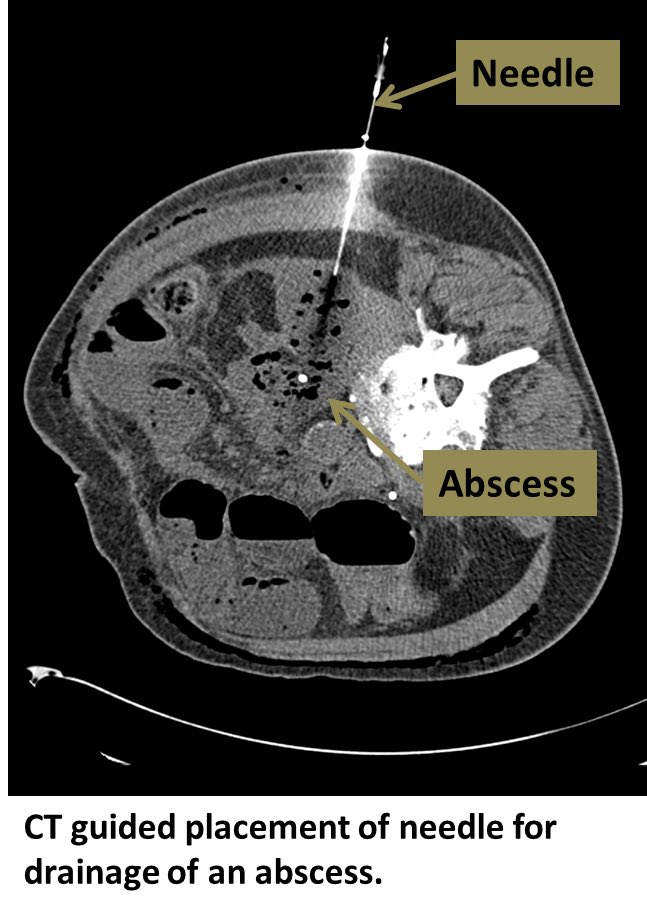
Abdominal collections: (General Rules)
Percutaneous drainage if size > 4cm
IV AB if smaller
O.R if unstable
Multiple collections? Open VS lap lavage & leave a drain (don’t try to fix the primary pathology -appendix or diverticulitis, control sepsis, wash, put a drain and leave🗣
Percutaneous drainage if size > 4cm
IV AB if smaller
O.R if unstable
Multiple collections? Open VS lap lavage & leave a drain (don’t try to fix the primary pathology -appendix or diverticulitis, control sepsis, wash, put a drain and leave🗣
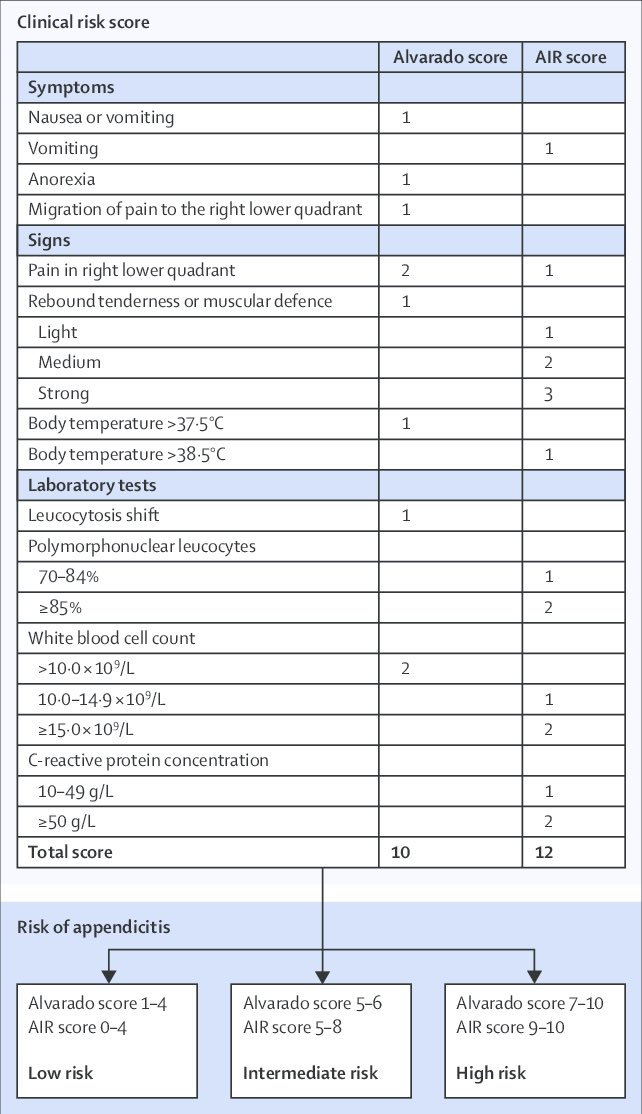
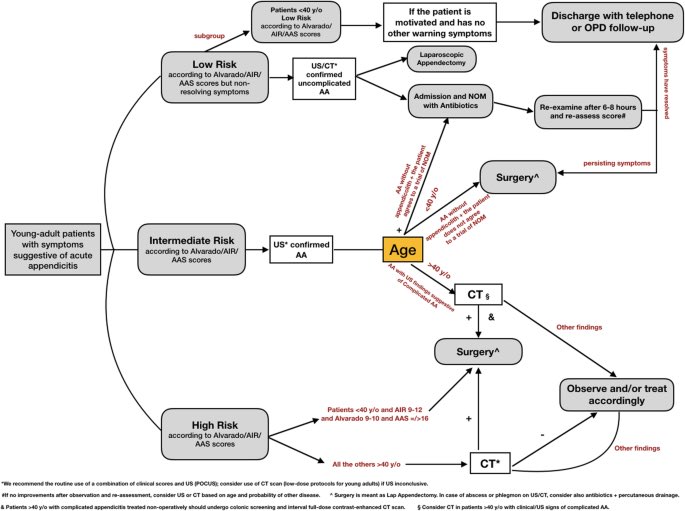
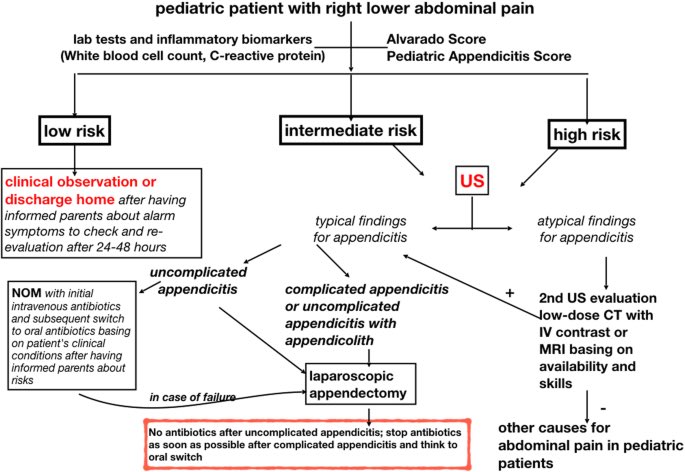
In acute appendicitis diagnosis is made with US, you need CT here:
Older than 40 (debatable)
Symptoms > 72 hours
Morbidly obese
Recurrent atypical symptoms
——
Young male Alvarado/AIR score is high>> direct OR
Female US to assess for gyne problems.
Pediatrics>> US is the standard
Older than 40 (debatable)
Symptoms > 72 hours
Morbidly obese
Recurrent atypical symptoms
——
Young male Alvarado/AIR score is high>> direct OR
Female US to assess for gyne problems.
Pediatrics>> US is the standard
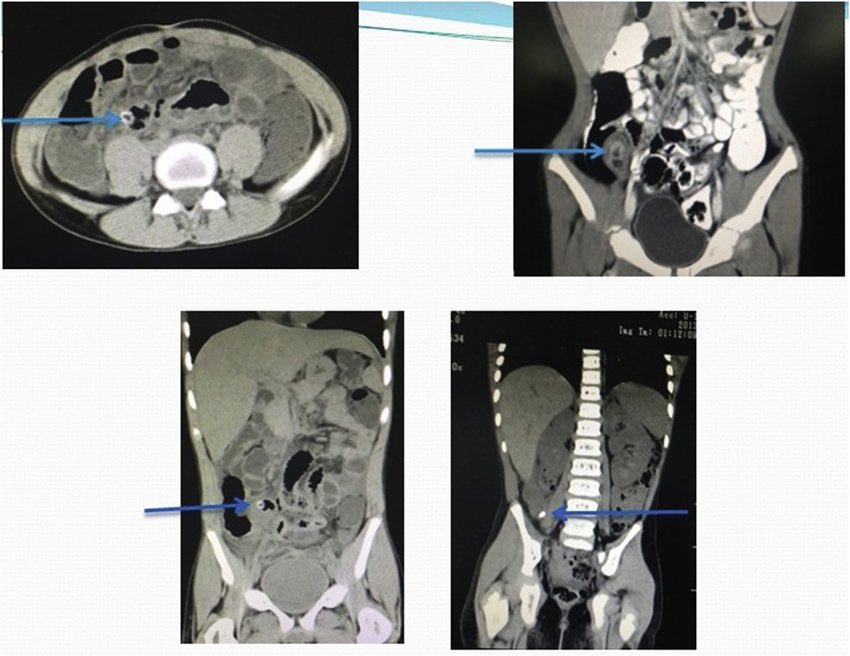
Patients with appendicitis can come with Phlegmon (the process just before forming a mature abscess, where small bowel, omentum and appendix forms a mass)
Tx is IV AB , drain only if abscess,unstable or worrisome symptoms? Exploration (open for the exam)
Interval appendectomy?👇🏻
Tx is IV AB , drain only if abscess,unstable or worrisome symptoms? Exploration (open for the exam)
Interval appendectomy?👇🏻


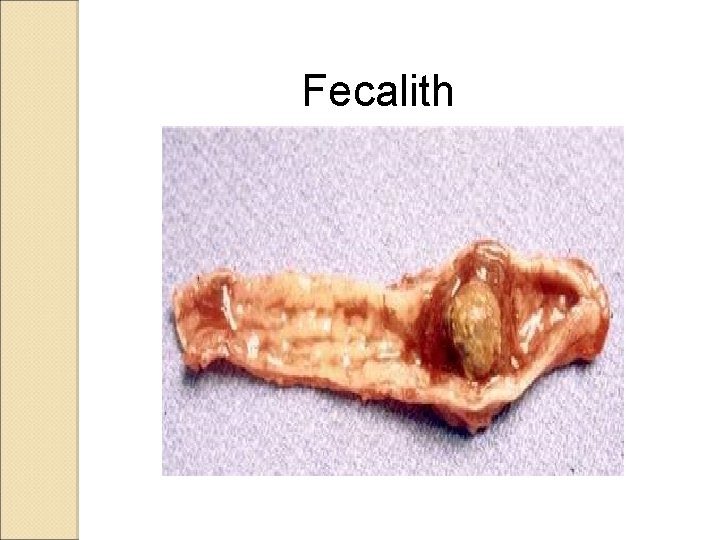
Interval appendectomy is only done on case by case basis, if symptoms persists and there’s a fecolith since the first presentation, it’s likely you’ll need to do surgery, usually 6-12 weeks after pts has improved, you need a new CT scan before it,colonoscopy for all those >40 y/o
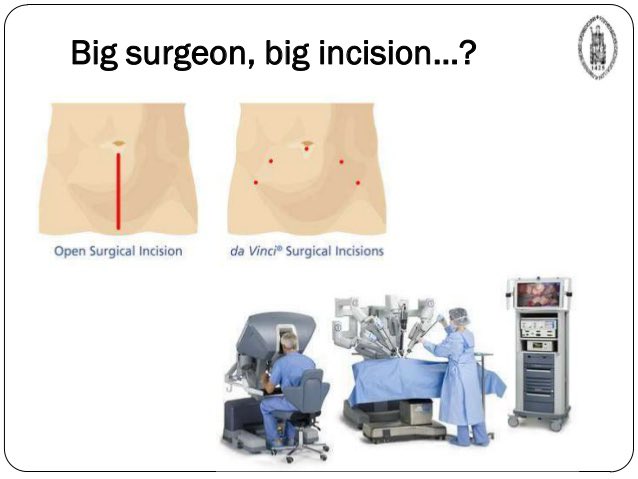
There’s no longer the so called “big surgeon big incision” , the goal is to minimize the trauma of intervention for your patient so he can leave the hospital early:
AB (Oral vs IV)
Percutaneous drainage
Laparoscopic lavage or exploration
And finally; open surgery
الهرم الجراحي🤓
AB (Oral vs IV)
Percutaneous drainage
Laparoscopic lavage or exploration
And finally; open surgery
الهرم الجراحي🤓
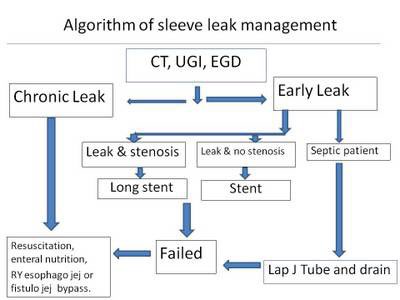
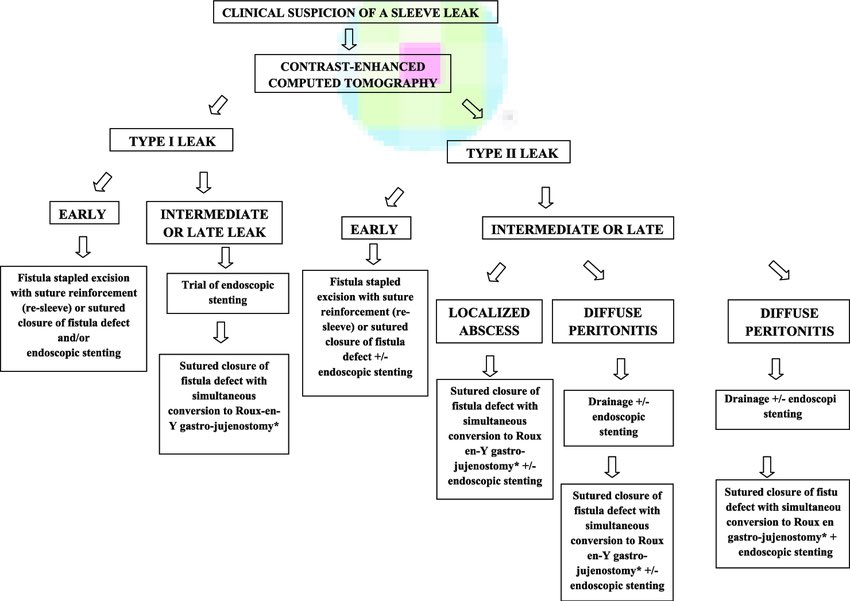
In scenarios of post bariatric surgery complications:
It could be PE (mainly chest pain, hypoxia & tachy)
Leak (abdominal pain, tachycardia)
Bleeding (drop in Hb, tachy)
In general:
Resuscitation and CT with contrast oral and IV
If unstable or major early leak>> diagnostic lap
It could be PE (mainly chest pain, hypoxia & tachy)
Leak (abdominal pain, tachycardia)
Bleeding (drop in Hb, tachy)
In general:
Resuscitation and CT with contrast oral and IV
If unstable or major early leak>> diagnostic lap
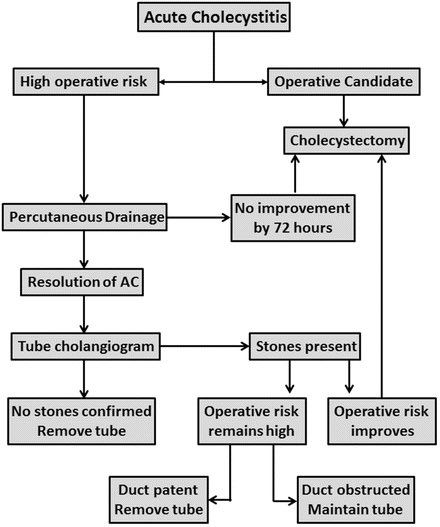
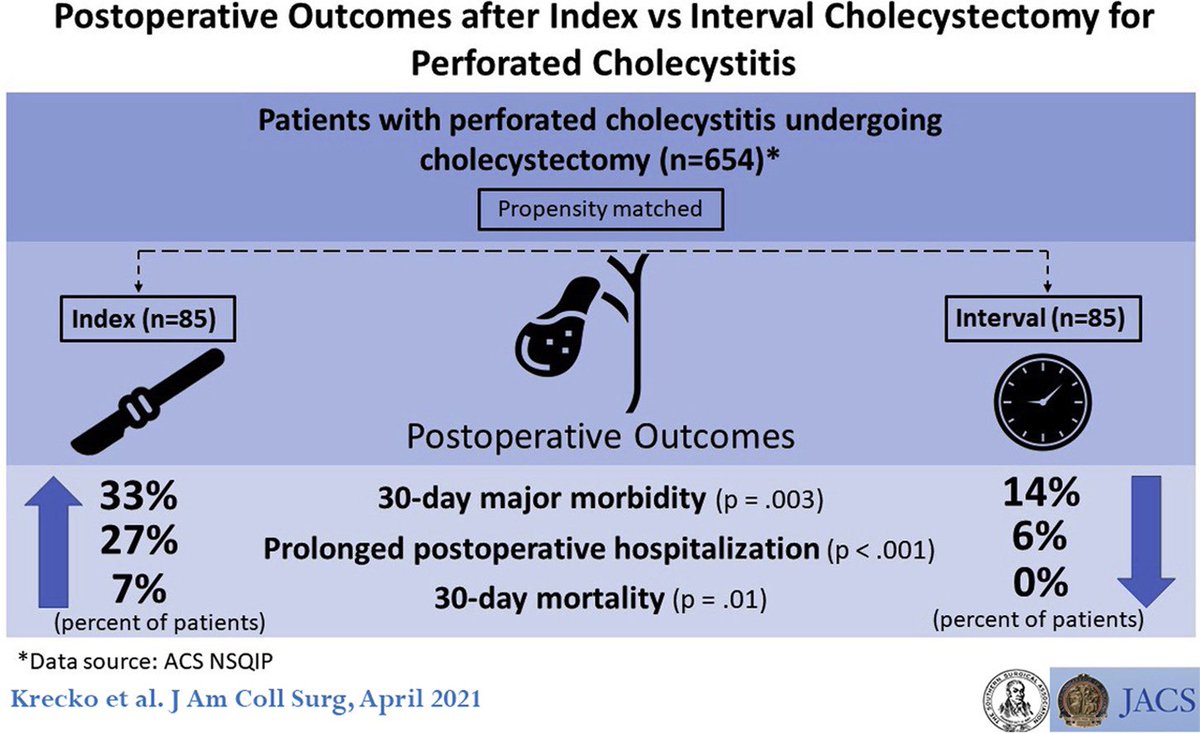
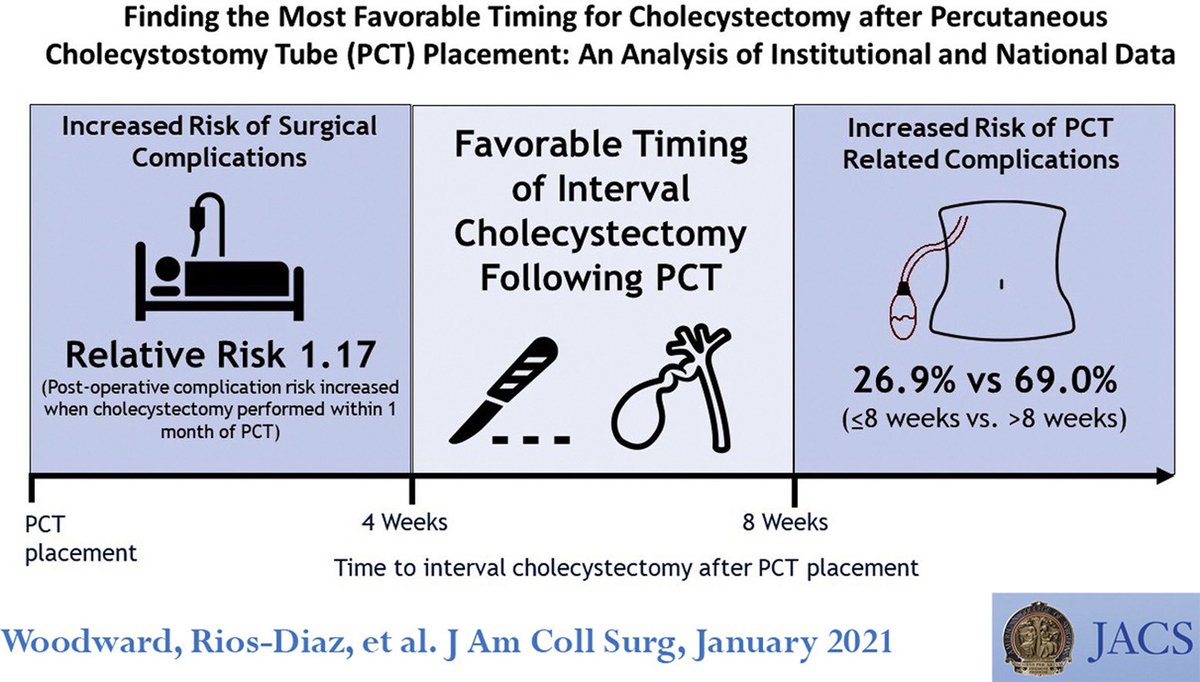
Timing of cholecystectomy:
Biliary pain: elective (wks)
Acute chole: same admission (unless unfit you can go for cholecystostomy tube as a bridge)
Acute chole post MI: surgery in 6-8 weeks (Fiser 2020)
Pancreatitis: mild & moderate:same admission, severe 6 wks.
Cholangitis 6 wks
Biliary pain: elective (wks)
Acute chole: same admission (unless unfit you can go for cholecystostomy tube as a bridge)
Acute chole post MI: surgery in 6-8 weeks (Fiser 2020)
Pancreatitis: mild & moderate:same admission, severe 6 wks.
Cholangitis 6 wks
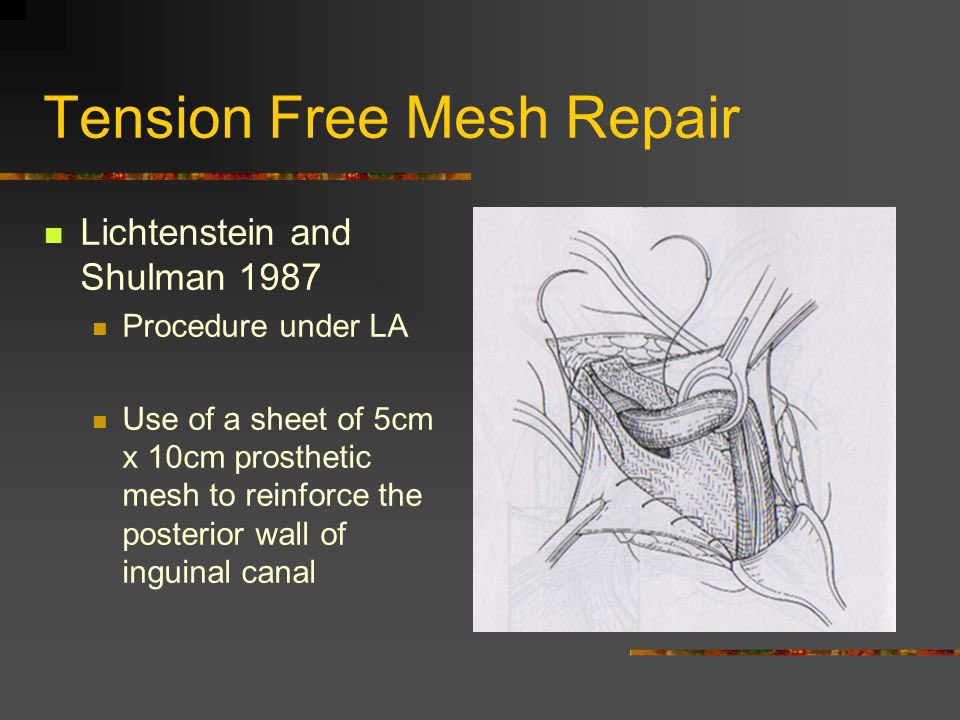
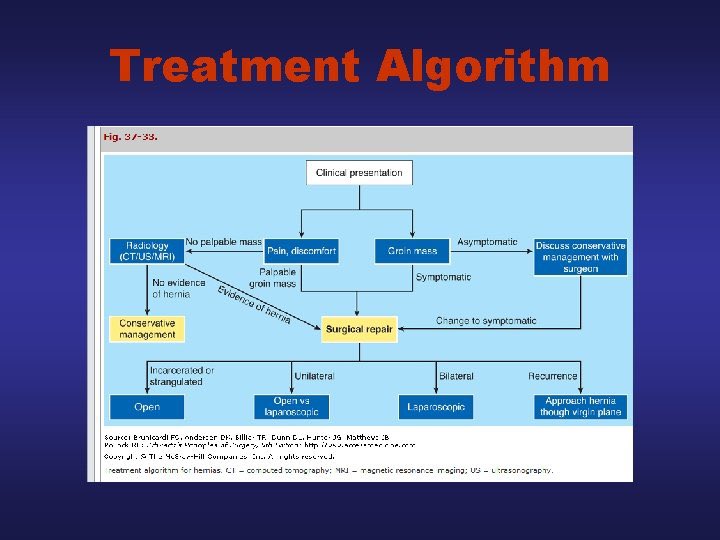
Hernia:
Indirect inguinal hernia is MC in all age groups
Females MC hernia: inguinal indirect
Femoral:always repair (lap vs open)
Pediatrics:mo mesh repair(herniotomy)
Complicated hernia (strangulated or obstructed):herniorhaphy (no mesh, tissue repair)
All others: Lechtinestien
Indirect inguinal hernia is MC in all age groups
Females MC hernia: inguinal indirect
Femoral:always repair (lap vs open)
Pediatrics:mo mesh repair(herniotomy)
Complicated hernia (strangulated or obstructed):herniorhaphy (no mesh, tissue repair)
All others: Lechtinestien

Men with minimally symptomatic hernia: observation
Clinically not clear hernia: US
Lap in: bilateral, obese recurrent after open repair
Recurrent after lap: Open repair
Hernia= Anatomy !
MC complication: neuralgia (not recurrence)
Ischemic orchitis: pampiniform plexus injury
Clinically not clear hernia: US
Lap in: bilateral, obese recurrent after open repair
Recurrent after lap: Open repair
Hernia= Anatomy !
MC complication: neuralgia (not recurrence)
Ischemic orchitis: pampiniform plexus injury
These rules are general and in real life we tailor the Mx according to the case and the latest evidence, exams are not real life❌
More pearls will follow on thyroid, adrenals, GIT and HPB, vascular & more, discussion is welcome.
Stay tuned for more under this thread soon💪🏻🔥
More pearls will follow on thyroid, adrenals, GIT and HPB, vascular & more, discussion is welcome.
Stay tuned for more under this thread soon💪🏻🔥
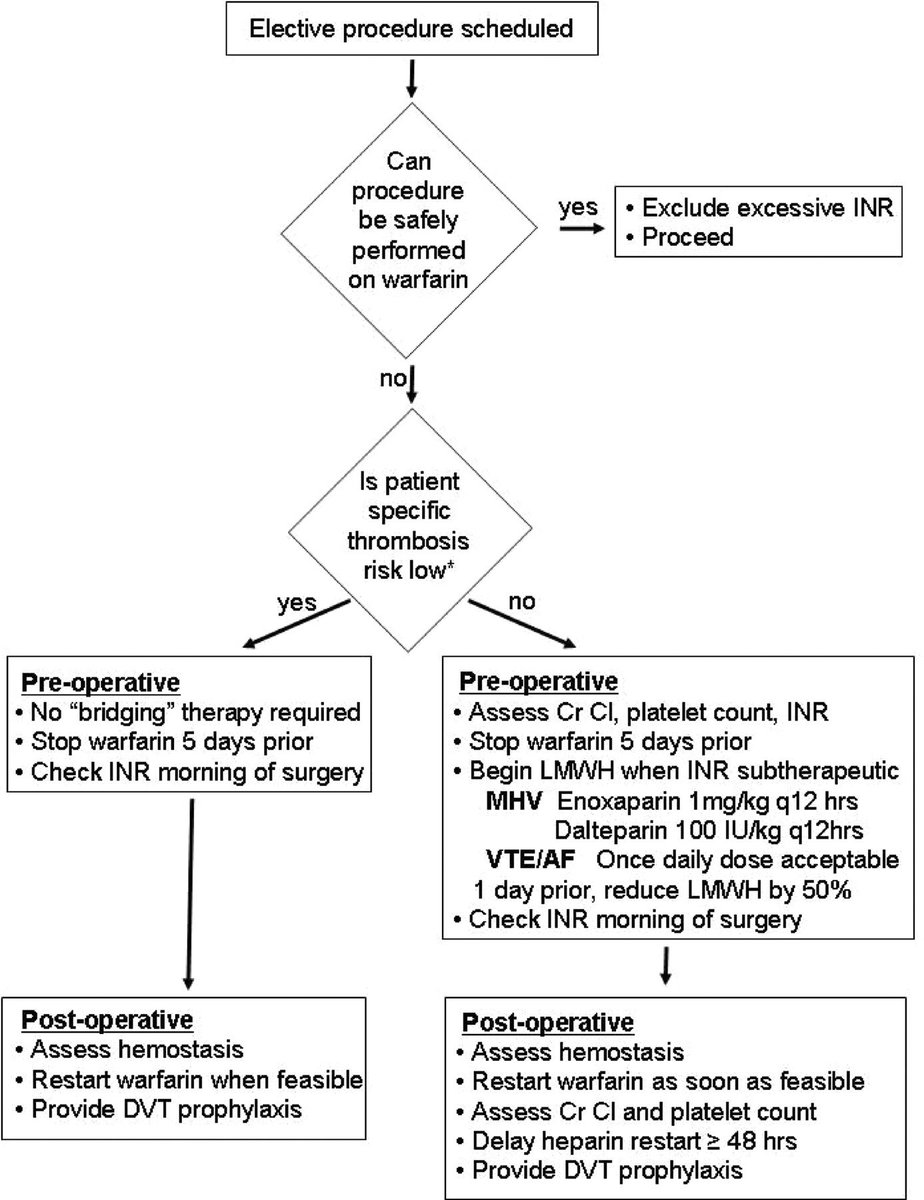
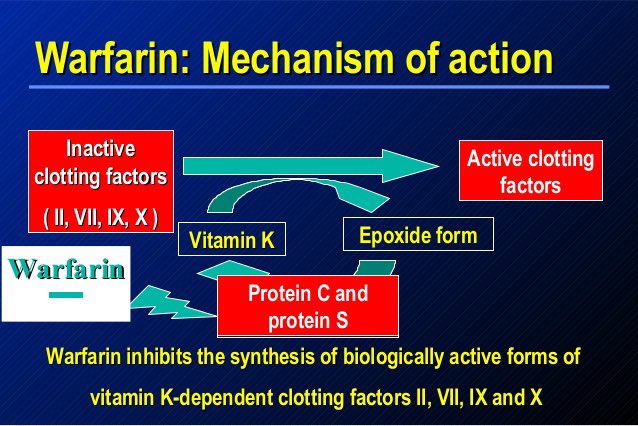
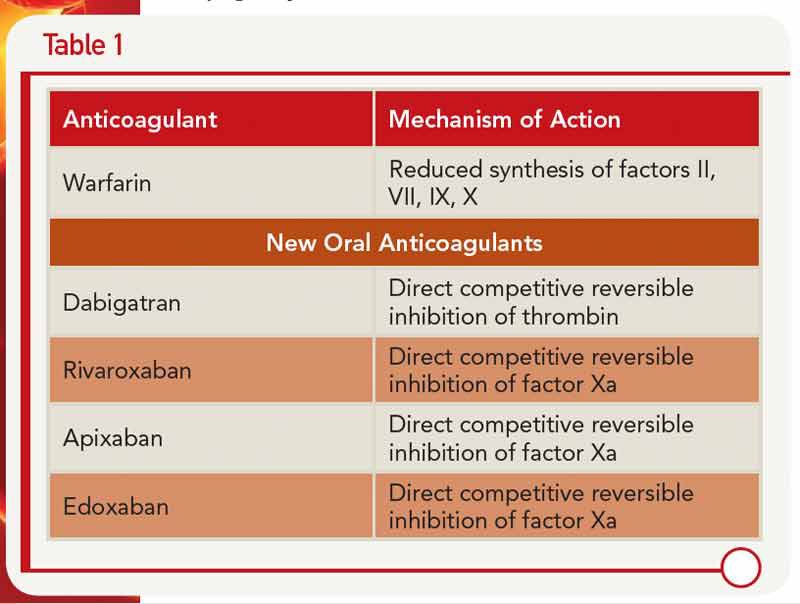
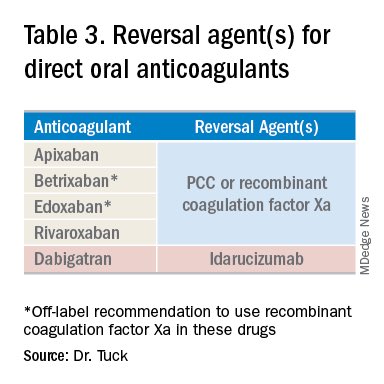
When to stop anticoagulation:
Warfarin 5 days pre-op (Sabiston)
Then bridge with LMWH or UFH till 6hrs pre-OP (no bridging in low risk Sx) , always bridge in metallic valves.
Re-warfarin after no bleeding risk post op, keep LMWH simultaneously for 5 days (to prevent thrombosis)
Warfarin 5 days pre-op (Sabiston)
Then bridge with LMWH or UFH till 6hrs pre-OP (no bridging in low risk Sx) , always bridge in metallic valves.
Re-warfarin after no bleeding risk post op, keep LMWH simultaneously for 5 days (to prevent thrombosis)
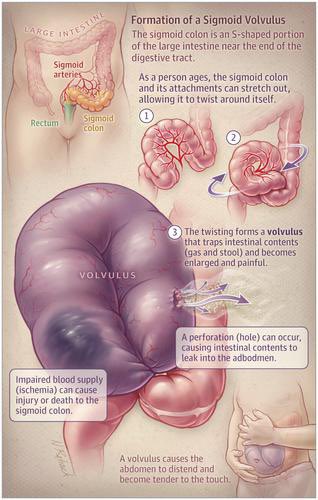
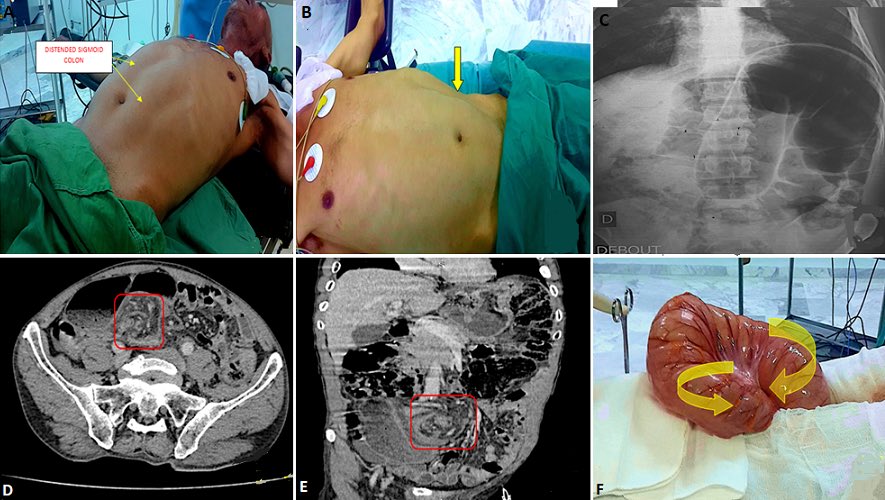
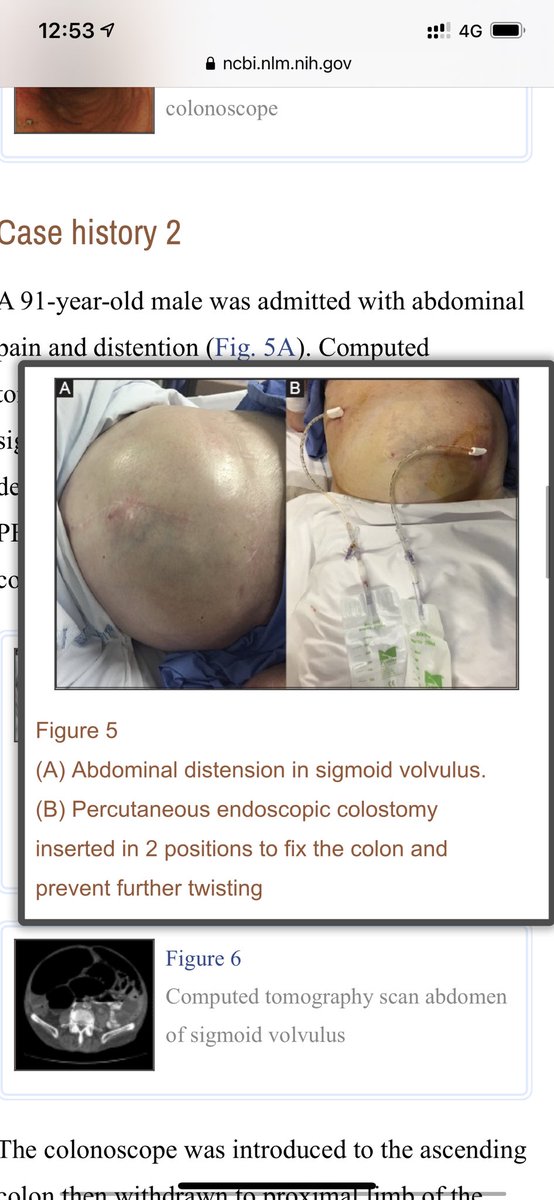
Volvulus:
Sigmoid is most common
Huge distention in bed ridden elderly w/ no previous surgeries.
Xray: coffee bean
Unstable: Hartman’s procedure
Stable: Colonoscopy & elective resection same admission
Cecal volvulus: Rt hemicolectomy, no deflation
Some centers: PEC tube (see pix)
Sigmoid is most common
Huge distention in bed ridden elderly w/ no previous surgeries.
Xray: coffee bean
Unstable: Hartman’s procedure
Stable: Colonoscopy & elective resection same admission
Cecal volvulus: Rt hemicolectomy, no deflation
Some centers: PEC tube (see pix)

Let’s try this Q
-what extra info do you need to answer?
- what’s the general approach to colorectal polyps?
Q:
Patient had a sigmoid polyp removed. They found on histopathology well differentiated
adenocarcinoma and the margins are free from cancer. What is the best next step?
-what extra info do you need to answer?
- what’s the general approach to colorectal polyps?
Q:
Patient had a sigmoid polyp removed. They found on histopathology well differentiated
adenocarcinoma and the margins are free from cancer. What is the best next step?
فاصل 😁
@drkeithsiau your opinion here is so much valid, too many opinions and guidelines, I saw your previous awesome thread on this, can we give the summary of summary here for students and residents? 🔥🔥
See? Surgeons are nice 😅😅
See? Surgeons are nice 😅😅
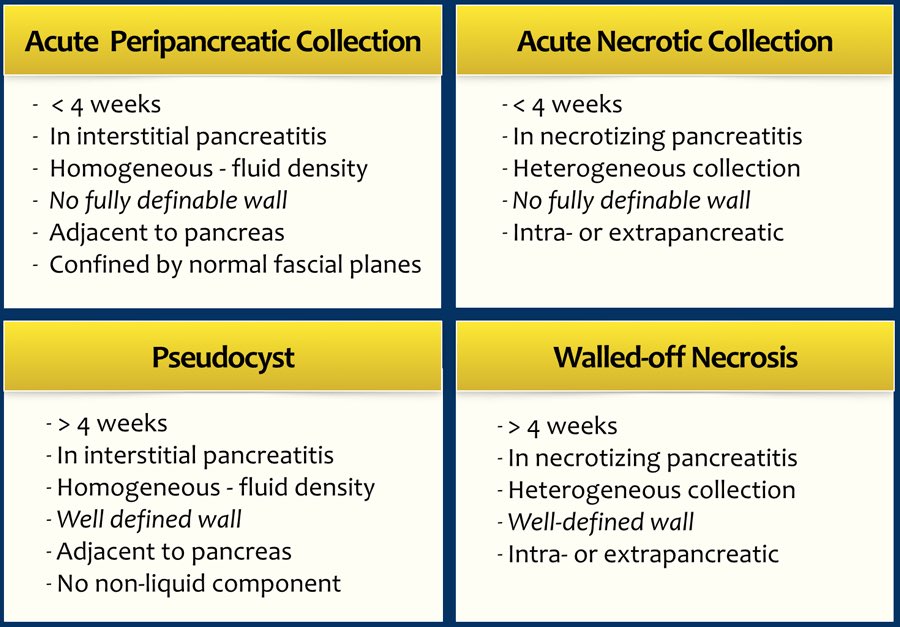
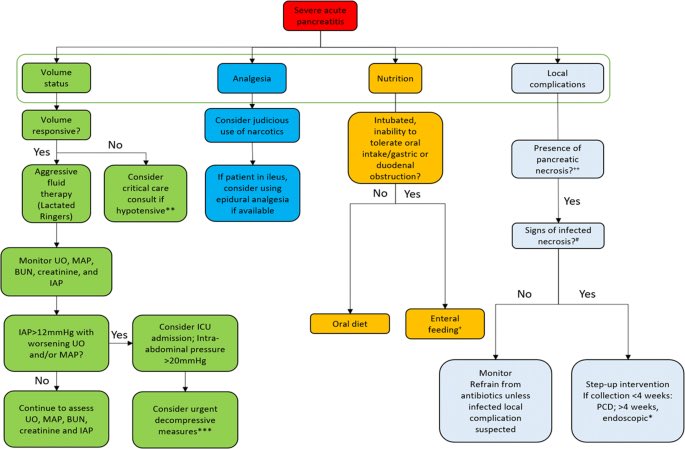
Acute pancreatitis:
NO ANTIBIOTIC UNLESS REALLY SEVERE OR EVIDENCE OF INFECTION (FNA or bubbles in CT= infected necrosis)
Step up approach always for the 4 major complications (see pix)
Always feed your pt unless vomiting or severe pancreatitis
Mortality of infected necrosis>20%
NO ANTIBIOTIC UNLESS REALLY SEVERE OR EVIDENCE OF INFECTION (FNA or bubbles in CT= infected necrosis)
Step up approach always for the 4 major complications (see pix)
Always feed your pt unless vomiting or severe pancreatitis
Mortality of infected necrosis>20%
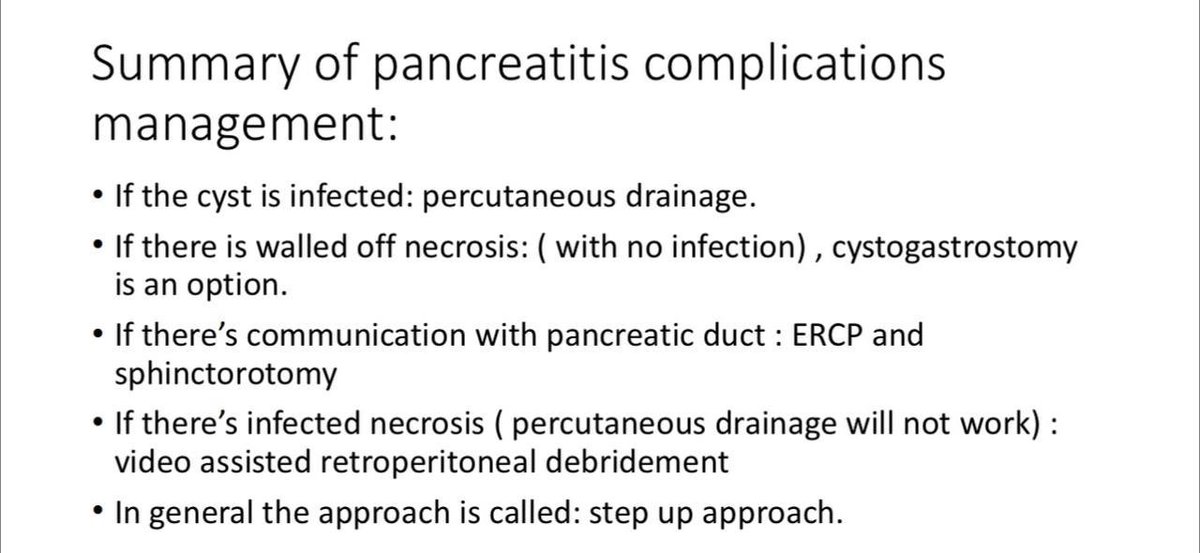

ERCP-sphinctorotomy was thought to be of benefit in acute pancreatitis (whether with cholangitis or not, whether liver function is elevated or not)
New evidence from this RCT says: NO
You need ERCP if:
✅ cholangitis
✅ persistentobstructive jaundice
New evidence from this RCT says: NO
You need ERCP if:
✅ cholangitis
✅ persistentobstructive jaundice
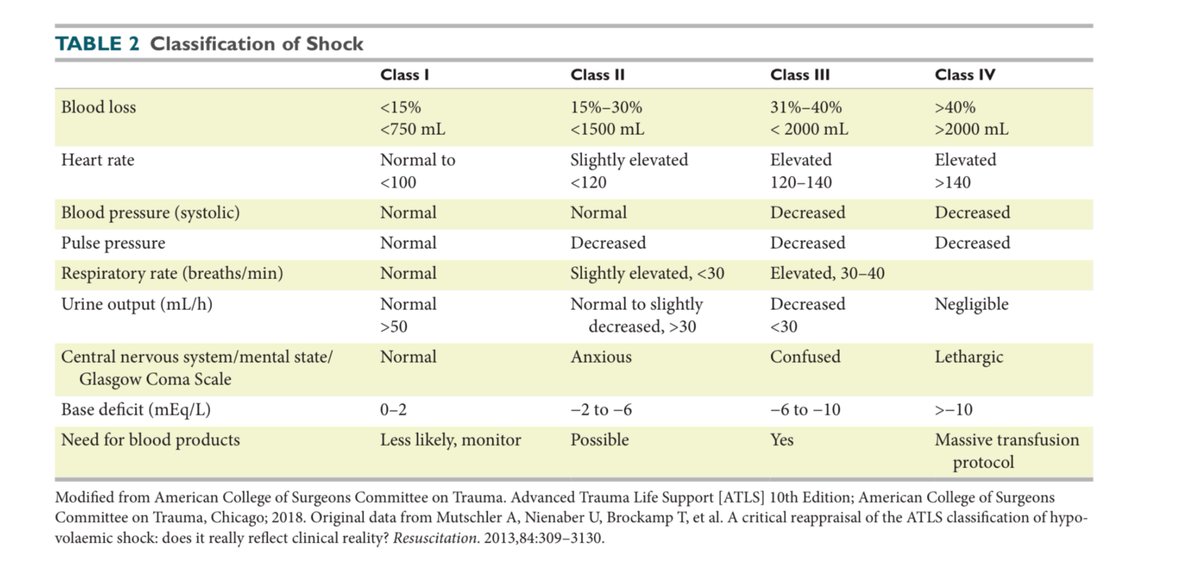
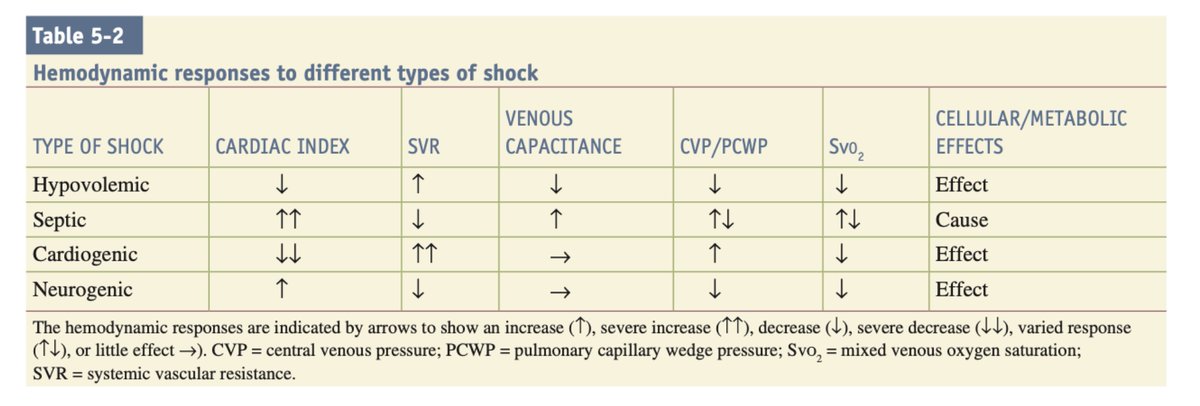
there are 1000 ways of approaching questions of shocked patients, non of those ways include NOT memorizing and understanding every bit of these 2 tables.
hemorrhage has classes, but death does have only one class, so the earlier you diagnose shock, the higher chance of living!📈
hemorrhage has classes, but death does have only one class, so the earlier you diagnose shock, the higher chance of living!📈
Please share it with your colleagues 🔥🔥 will be a great review with you guys.
يوم حل الأسئلة المجاني الأربعاء القادم.
للتسجيل:
us02web.zoom.us
us02web.zoom.us
us02web.zoom.us
us02web.zoom.us
us02web.zoom.us
us02web.zoom.usا
يوم حل الأسئلة المجاني الأربعاء القادم.
للتسجيل:
us02web.zoom.us
us02web.zoom.us
us02web.zoom.us
us02web.zoom.us
us02web.zoom.us
us02web.zoom.usا
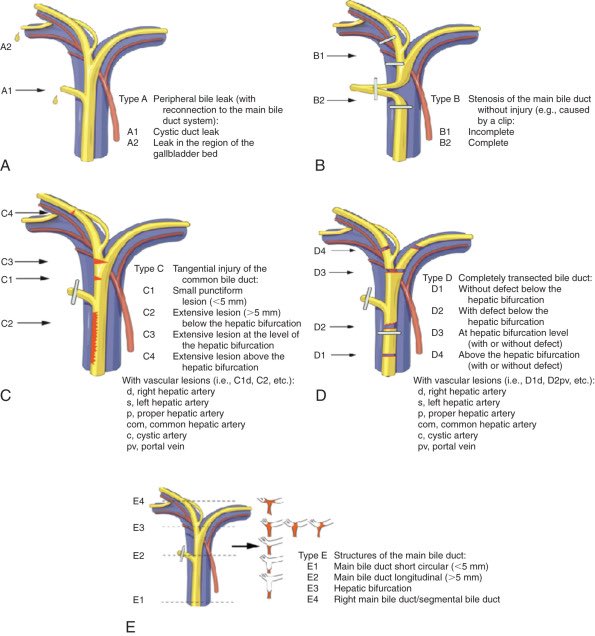
For bile duct injury follow these algorithms & keep in mind:
- always drain collections before definitive Tx.
- cystic duct leak = ERCP + stent but MRCP before to confirm Dx.
- strictures can be a long term complication, difficult to differentiate from malignancy.
- CALL 4 HELP!
- always drain collections before definitive Tx.
- cystic duct leak = ERCP + stent but MRCP before to confirm Dx.
- strictures can be a long term complication, difficult to differentiate from malignancy.
- CALL 4 HELP!
جاري تحميل الاقتراحات...