

1/ Case discussion with a friend involved a
56 y.o with :
New ascites, malaise, low-grade fever
Hct 35.8
WBC 9.7
Plts 120
ALT 59 U/L AST 96 U/L
Alk phos 230 U/L
T bilirubin 1.0 mg/dL
Albumin 2.8 g/dL
Globulins 4.0 g/dL
My approach:
56 y.o with :
New ascites, malaise, low-grade fever
Hct 35.8
WBC 9.7
Plts 120
ALT 59 U/L AST 96 U/L
Alk phos 230 U/L
T bilirubin 1.0 mg/dL
Albumin 2.8 g/dL
Globulins 4.0 g/dL
My approach:

2/R value < 2 therefore Cholestatic
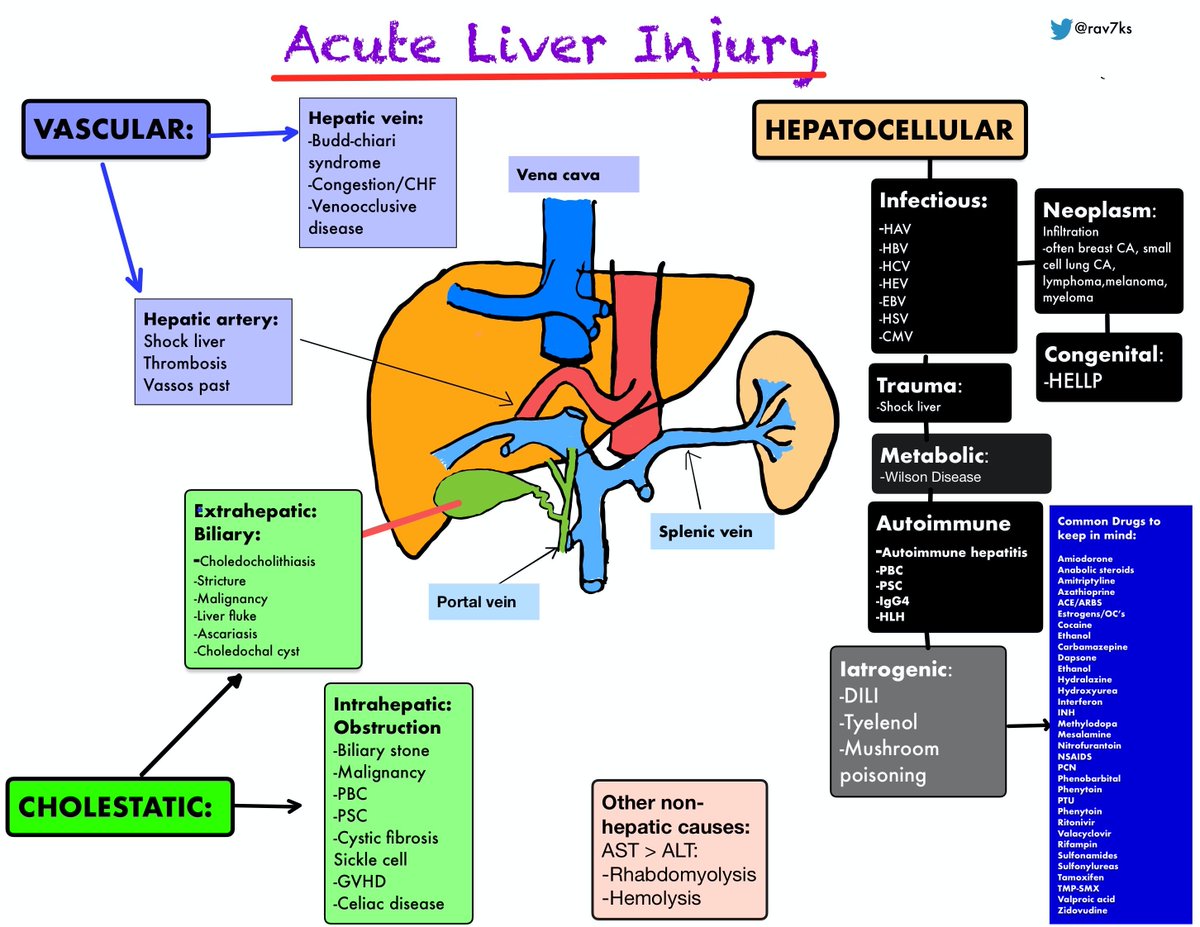
DDx 2.0 version for Acute liver injury:
DDx 2.0 version for Acute liver injury:
3/Ascites: Total protein 0.8 g/dL, albumin 0.5 g/dL
SAAG 2.3
WBC 83/mm3
Cytology negative
SAAG indicated Portal HTN which could be a pre/Intra or post hepatic issue.
#Pearl HFailure- would see ⬆️SAAG and ⬆️TP in ascitic fluid
SAAG 2.3
WBC 83/mm3
Cytology negative
SAAG indicated Portal HTN which could be a pre/Intra or post hepatic issue.
#Pearl HFailure- would see ⬆️SAAG and ⬆️TP in ascitic fluid
4/Imaging -Abd CT:
ascites, atrophic spleen, gallbladder sludge
Viral/Infectious/Autoimmune workup : Negative
ECHO: EF Normal
Liver biopsy: marked sinusoidal dilatation and congestion with hepatocyte atrophy and focal necrosis suggestive of vascular outlet obstruction
ascites, atrophic spleen, gallbladder sludge
Viral/Infectious/Autoimmune workup : Negative
ECHO: EF Normal
Liver biopsy: marked sinusoidal dilatation and congestion with hepatocyte atrophy and focal necrosis suggestive of vascular outlet obstruction
5/Summary:PT with Abnormal liver enzymes, ascitesHistory of occasional diarrheaKnown osteoporosisIrish descentShort statureBrother awaiting liver transplantationAtrophic spleen on CT

6/Diagnosis
Positive IgA transglutaminase antibody
Small bowel biopsy: celiac disease
Positive IgA transglutaminase antibody
Small bowel biopsy: celiac disease

7/With Celiac Disease- hepatobiliary diseases have been described, including elevations of liver enzyme levels, nonspecific hepatitis, nonalcoholic fatty liver disease, and autoimmune and cholestatic liver disease.
cghjournal.org
cghjournal.org

8/Celiac disease serological testing should be part of the general workup of patients with unexplained elevated liver enzyme levels if common causes of liver disease have been ruled out.

@malaksalharbi1 Reticuloendothelial block due to circulating immune complexes could also be one of the major mechanisms implied.
gut.bmj.com
cghjournal.org
gut.bmj.com
cghjournal.org
Loading suggestions...