

Pulmonary Kaposi Sarcoma (KS) can involve the parenchyma, airways, pleura, and/or intrathoracic LNs. Symptoms are non-specific pulmonary sxs usually developing over a few weeks. However, endobronchial KS can be asx.
Patients w/ known mucocutaneous KS have a higher likelihood of lung involvement: in 80-90%, pulm involvement is concurrent w/ mucocutaneous disease. However, ~15% have initial lung involvement w/o heralding derm findings. (Think lesions that are 🟪/🟥.)
Now, who gets this disease? Usually, low CD4 (<150) & high HIV viral load (>10k). Remember, such immunocompromised people w/ pulmonary symptoms require a broad DDx. Given sub-acute time course, particular attention in the DDx should be given to...
infections (particularly atypical bacteria, mycobacteria, & fungi). The other important DDx bucket includes *other malignancies* (eg pulm lymphoma, primary effusion lymphoma, multicentric Castleman's). Such consideration makes sense when we see KS' radiographic findings...
Highly suggestive findings on chest CT are 1) Hilar densities extending into the parenchyma in a perivascular/peribronchial distribution, and 2) Septal/nodular pattern w/ concomitant pleural effusions ojrd.biomedcentral.com
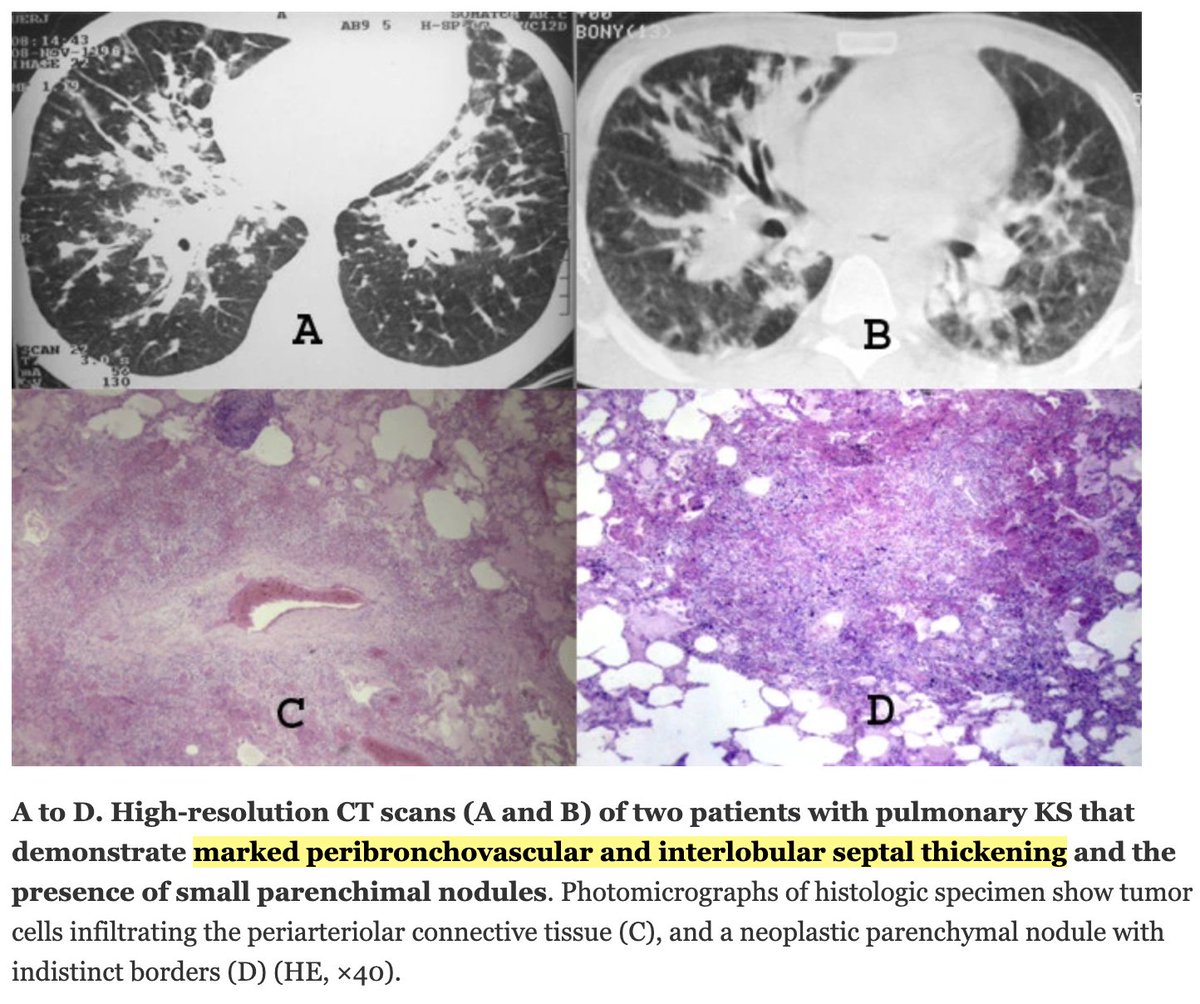
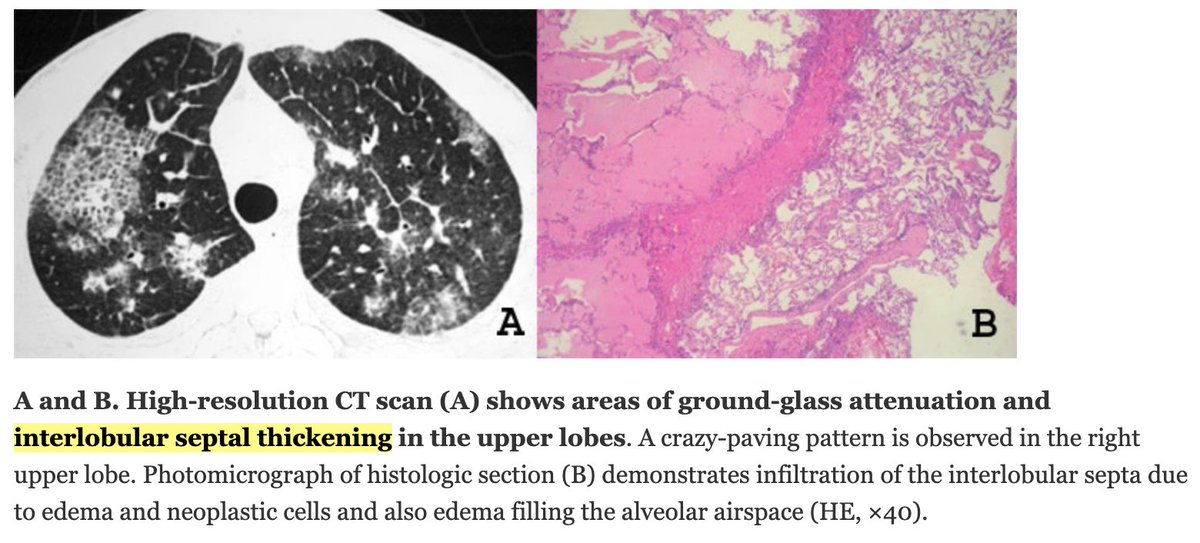
These radiographic findings fall nicely into @CPSolvers' lung nodule schema within the perilymphatic DDx bucket. This perilymphatic distribution can be further broken down into 4 areas where pulmonary lymphatics predominate. Peribronchovascular is one of these areas.
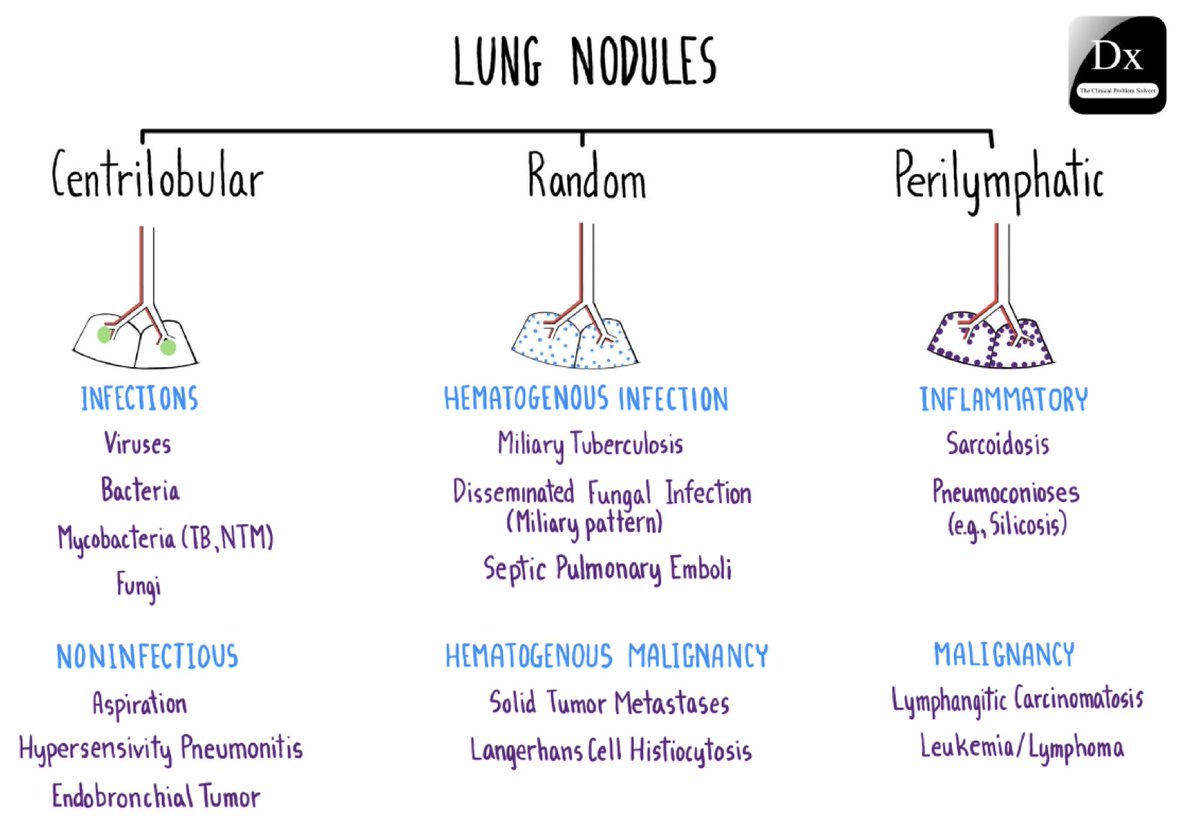
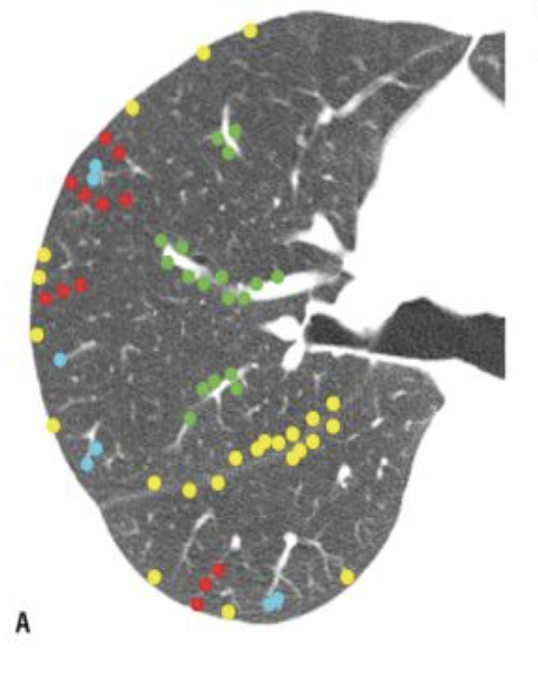
This great page shows the 4 areas of pulmonary lymphatics, including parahilar peribronchovascular interstitium (🟢), subpleural interstitium (🟡), interlobular septa (🔴), & centrilobular peribronchovascular interstitium. #fig3.4" target="_blank" rel="noopener" onclick="event.stopPropagation()">radiologykey.com
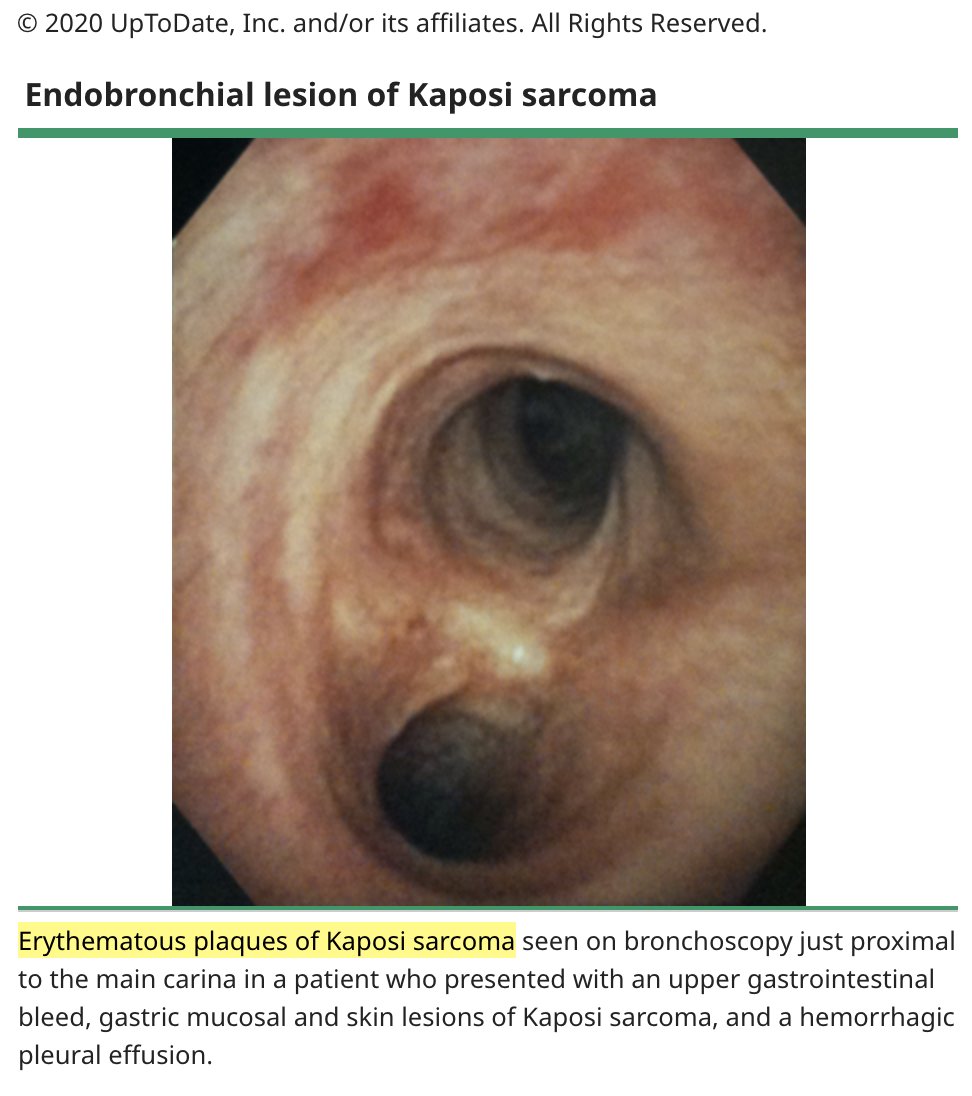
How is this zebra 🦓 diagnosed? In the setting of compatible clinical/radiographic findings, bronchoscopy is needed to identify characteristic endobronchial lesions. Bronch also helpful for BAL exclusion of infectious etiologies or other tumors.
Just like on the skin, these lesions look violet/red. However, note bacillary angiomatosis can look similar in airways. (This mimic usually p/w raised rather than flat lesions.) Endobronchial/transbronchial biopsies have low yield for diagnosis & risk hemorrhage (up to 30%).
💊 Treatment? 💊 If no pulm symptoms, only ART. If progression or symptoms, ART + chemo. Hope someone finds this interesting!
Loading suggestions...